w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Investigation
of
MEFV
gene
polymorphisms
(G138G
and
A165A)
in
adult
patients
with
familial
Mediterranean
fever
Mustafa
Ferhat
Öksuz
a,∗,
Mutlu
Karkucak
b,
Orhan
Görukmez
c,
Gökhan
Ocako ˘glu
d,
Abdulmecit
Yıldız
e,
Mehmet
Ture
f,
Tahsin
Yakut
f,
Kamil
Dilek
aaUludagUniversity,FacultyofMedicine,DepartmentofInternalMedicine,DivisionofRheumatology,Bursa,Turkey bSakaryaUniversity,EducationandResearchHospital,DepartmentofMedicalGenetics,Sakarya,Turkey
cSevketYilmazEducationandResearchHospital,DepartmentofMedicalGenetics,Bursa,Turkey dUludagUniversity,FacultyofMedicine,DepartmentofBiostatistics,Bursa,Turkey
eUludagUniversity,FacultyofMedicine,DepartmentofInternalMedicine,DivisionofNephrology,Bursa,Turkey fUludagUniversity,FacultyofMedicine,DepartmentofMedicalGenetics,Bursa,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received13June2015 Accepted25September2015 Availableonline10March2016
Keywords:
FamilialMediterraneanfever MEFVgene
Polymorphism
a
b
s
t
r
a
c
t
Aim: VariousmutationshavebeenidentifiedintheMediterraneanfever(MEFV)genewhich isreportedtoberesponsiblefromFamilialMediterraneanfever(FMF).Inourstudy,weaimed todeterminethefrequencyoftheMEFVmutationsinourregionandtoinvestigatethe impactofG138G(rs224224,c.414A>G)andA165A(rs224223,c.495C>A)genepolymorphisms ontheclinicalfindingsofthedisease.
Methods:OnehundredandsixteenpatientsdiagnosedwithFMFand95controlsubjects wereincludedinthisstudy.WeusedtheDNAsequenceanalysismethodtoidentifythe mostprevailing10mutationslocatedinexon2and10ofMEFVgene.
Results:AsaresultoftheMEFVmutationanalysis,themostcommonmutationwasthe M694Vmutationallelewithafrequencyrateof41.8%.Whenthepatientsgroupandcontrol groupwerecomparedintermsoffrequencyofbothpolymorphicalleles(Gpolymorphic allele,observedinG138GandtheApolymorphicallele,observedinA165A),thevariation wasobservedtobestatisticallysignificant(p<0.001).ItwasfoundthattheMEFVmutation typeshavenorelationwithclinicalfindingsandamyloidosis(p>0.05).
Conclusions: Toourknowledge,ourstudyisthefirststudyintheSouthernMarmararegion thatreportsthefrequencyofMEFVmutations.Ourfindingsimplythatthepolymorphisms ofG138GandA165Amayhaveanimpactonprogressofthedisease.Wethinkthatmore studies,havinghighernumberofcasesandinvestigatingthepolymorphismsofMEFVgene, areneeded.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](M.F.Öksuz). http://dx.doi.org/10.1016/j.rbre.2016.02.004
Investigac¸ão
de
polimorfismos
no
gene
MEFV
(G138G
e
A165A)
em
pacientes
adultos
com
febre
mediterrânica
familiar
Palavras-chave:
Febremediterrânicafamiliar GeneMEFV
Polimorfismo
r
e
s
u
m
o
Objetivo: Identificaram-se váriasmutac¸ões nogene dafebremediterrânica(MEFV)que relata-sequesãoresponsáveispelafebremediterrânicafamiliar(FMF).Esteestudoteve como objetivodeterminara frequênciademutac¸õesno MEFVnaregiãosul domar de MármaraeinvestigaroimpactodospolimorfismosgenéticosG138G(rs224224,c.414A>G)e A165A(rs224223,c.495C>A)nosachadosclínicosdadoenc¸a.
Métodos:Foramincluídosnesteestudo116pacientescomdiagnósticodeFMFe95indivíduos nogrupocontrole.Utilizou-seométododeanálisedasequênciadeDNAparaidentificaras 10mutac¸õesmaisprevalenteslocalizadasnoséxons2e10dogeneMEFV.
Resultados: Como resultadoda análise da mutac¸ãoMEFV, a mutac¸ãomaiscomum foi a mutac¸ãoalélicaM694V,comumataxadefrequênciade41,8%. Quandoosgruposde pacientese controlesforamcomparadosem termosde frequênciade ambosos alelos polimórficos(alelopolimórficoG,observadonoG138GeoalelopolimórficoA,observado noA165A),avariac¸ãoobservadafoiestatisticamentesignificativa(p<0,001).Verificou-se queostiposdemutac¸ãonoMEFVnãotinhamrelac¸ãocomosachadosclínicosnemcoma amiloidose(p>0,05).
Conclusões: Quesetemconhecimento,esteestudoéoprimeirorealizadonaregiãosuldo mardeMármaraquerelataafrequênciademutac¸õesnoMEFV.Osachadosindicamqueos polimorfismosG138GeA165Apodemterumimpactosobreoprogressodadoenc¸a. Acredita-sequesãonecessáriosmaisestudos,abrangendoummaiornúmerodecasoseinvestigando ospolimorfismosdogeneMEFV.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Familial Mediterraneanfever (FMF)is an autosomal reces-sively inherited inflammatory disease that affects people fromtheMediterraneanregion,includingTurks,Armenians, non-AshkenaziJewsandArabs.Itischaracterizedby recur-rentepisodesofperitonitis,fever,rashes,arthritisandother serosalinflammations.1–3 Althoughattacks areself-limited, insomepatientsFMFcausesAAtypeamyloidosisthatleads torenalfailure.Amyloidosis commonlycausesother organ damagesbesidesrenalfailure.Theprognosisisdetermined by the complication ofAA amyloidosis. The inflammatory episodesandrenalamyloidosiscanbepreventedbycolchicine therapy.2,4–6
FMF is caused by mutations in MEFV gene. This gene is located on the short arm of chromosome 16 and con-sists of 10 exons. The protein, encoded by this gene and termedpyrin/marenostrin,ispresent almost exclusively in neutrophils and their precursors. This protein is involved in regulation of inflammation, apoptosis and/or cytokine secretion.4,7,8 The most common four mutations, M694V, V726A,M680I, and M694I are found in the exon 10 ofthe gene.AnothermutationE148Qisfoundintheexon2.These fivemutationsarefoundinmorethantwothirdsofcases.2,9 A number of studies have shown that the M964V muta-tion is associated with severe disease characterized with early onset, high attack frequency, need forhigh doses of colchicine, andhigh frequencyofamyloidosis inuntreated patients. E148Q is found in populations in which FMF is rare. E148Q mutation is also common but its role in the
disease is controversial. Most FMF experts refer to it as a mutation causingmild disease.2,11–13 Many polymorphisms likeD102D(rs224225,c.306T>C),G138G(rs224224,c.414A>G), A165A(rs224223,c.495C>A),R202Q(rs224222,c.605G>A) are found withintheexon2ofMEFV gene. D102D,G138G and A165Apolymorphisms aresynonymous variant.Inastudy, Basarslan etal.14 reported thatallele frequenciesofG138G andA165Apolymorphismswerefoundtobehigherinpatients withFMF.Inanotherstudy,Akaretal.15claimedthat138Gly allelecarriersweremorepronetothedevelopmentof amy-loidosis and added that therewas no statically significant differenceintermsofG138Gpolymorphismbetweenpatients andhealthysubjects.14,15
Inthepresentstudy,weaimedtodeterminethefrequency ofMEFV mutationinthe Southern Marmararegionand to investigate the impactofG138G and A165Agene polymor-phismsontheclinicalfindingsofthedisease.
Materials
and
methods
Studysubjects
Weretrospectivelyreviewedthemedicalrecordsofpatients withFMFfollowedinthedepartmentofInternalMedicineat UludagUniversityFacultyofMedicine,Bursa,Turkey.
in MEFV gene. The control group consisted of 95 subjects inwhom theFMFwas excludedclinicallyand nomutation hasbeen identified inMEFV gene.Demographicdata were recordedforbothpatientsandcontrolgroup.Thestudywas approvedbytheUludagUniversityEthicsCommittee.
DNAisolationandanalysisofMEFVgene (exons2and10)
Bloodsampleswereobtainedfrompatientandcontrolgroups andcollectedinEDTAtubes.GenomicDNAwasextractedfrom wholebloodusingdifferentDNAisolationkitaccordingtothe manufacturer’sinstructions(Dr.ZeydanlıLifeSciences,Ltd., Turkey;RTALaboratuvarlarıBiyolojikÜrünlerIlac¸veMakine San.Tic.A.S.,Gebze,Kocaeli,Turkey).
TheDNAfragmentscontainingtwoexonsoftheMEFVgene (exons2and10)wereamplifiedbypolymerasechainreaction (PCR)usingthespecificprimers.PCRsampleswereanalyzed bydirectsequencingofexons2and10oftheMEFVgenein anABI-3130DNAanalyzer(AppliedBiosystems,USA).After Sequencing,thedatawereanalyzedusingDNAsequencing analysisv5.2softwareformostfrequentmutations(E148Q, M694V,M680I,V726A,K695R,M694I,R761M,A744S)and poly-morphismsofexon2(G138GandA165A).
Statisticalanalysis
Ages were represented as median (minimum–maximum) values and were compared between groups using the Mann–WhitneyUtest.Inthecomparisonofcategorical vari-ables,Pearson’schi-square,Yateschi-squaretest,andFisher’s exacttestwereused.Allstatisticalanalyseswereperformed withSPSS13.0(Chicago,IL).Statisticalsignificancewassetat p<0.05.
Results
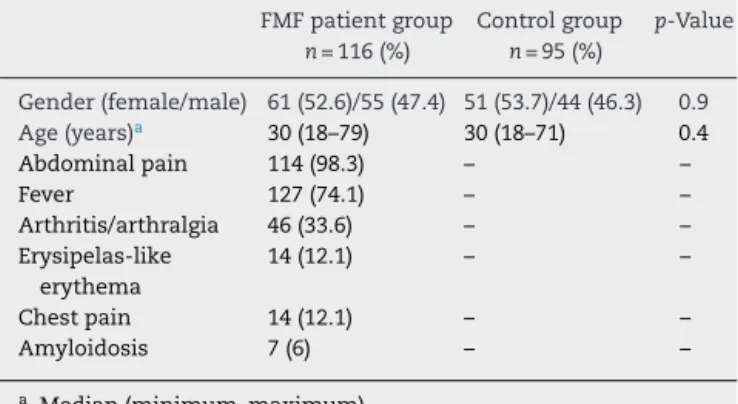
Thestudyconsistedof116adultswithFMFcases(61female,55 male)and95controlsubjects(51female,44male).Therewas nosignificantdifferenceingenderoragebetweenthegroups (p=0.9andp=0.4,respectively).Thedemographicandclinical featuresofFMFpatientsareshowninTable1.Inaddition,10 patients(8.6%)hadchronickidneydiseaseand15(12.7%)had proteinuria.
ThefrequencyofthefivethemostcommonMEFV muta-tionsinthisstudyareshowninTable2.
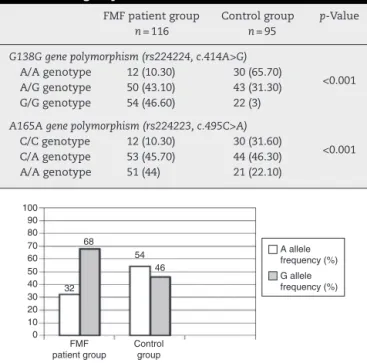
The distribution of genotypes of MEFV gene (homozy-gote,heterozygote,andcompoundheterozygote)isshownin Table3.Thedistributionofgenotypes(G138GandA165A)was significantlydifferentbetweenthegroupsofFMFpatientsand controls(p<0.001,Table4).FortheG138Ggenepolymorphism, thefrequencyoftheGallele was68%inFMFpatientgroup and46%incontrolgroup(Fig.1).FortheA165Agene polymor-phism,thefrequencyoftheAallelewas67%inFMFpatient groupand45%incontrolgroup(Fig.2).Theallelicfrequencies ofbothpolymorphismswerestatisticallysignificantdifferent betweenthegroups(p<0.001).
There was no significant relation between none of the mutations nor the polymorphisms (G138G and A165A)
Table1–ClinicalcharacteristicsoftheFMFpatientgroup andcontrolgroup.
FMFpatientgroup n=116(%)
Controlgroup n=95(%)
p-Value
Gender(female/male) 61(52.6)/55(47.4) 51(53.7)/44(46.3) 0.9
Age(years)a 30(18–79) 30(18–71) 0.4
Abdominalpain 114(98.3) – –
Fever 127(74.1) – –
Arthritis/arthralgia 46(33.6) – –
Erysipelas-like erythema
14(12.1) – –
Chestpain 14(12.1) – –
Amyloidosis 7(6) – –
a Median(minimum–maximum).
Table2–Theallelefrequenciesofthemostfrequently seenmutations.
Mutation Allelefrequencya
M694V 41.8%(97/232)
M680I(G/C) 14.6%(34/232)
V726A 6%(14/232)
K695R 3.4%(8/232)
E148Q 2.1%(5/232)
a Totalallele=232.
and clinical findings like fever, abdominal pain, arthritis/ arthralgia,erysipelas-likeerythema,chronickidneydisease, proteinuria,oramyloidosis(p>0.05forall).
Discussion
Inthepresentstudy,weevaluatedthefrequenciesoftheMEFV gene mutations, the allele frequency of G138G and A165A
Table3–ThedistributionofMEFVmutations.
MEFVmutations Numberofpatients %
M694V/N 38 32.7
M694V/M694V 20 17.2
M680I(G/C)/N 11 9.4
M694V/M680I(G/C) 10 8.6
V726A/N 7 6
K695R/N 6 5.4
M680I(G/C)/M680I(G/C) 5 4.3
M694V/V726A 5 4.3
E148Q/N 4 3.4
M694V/M694I 2 1.7
M680I(G/C)/V726A 2 1.7
M694V/E148Q 1 0.9
M694V/R761M 1 0.9
M680I(G/C)/R761M 1 0.9
K695R/K695R 1 0.9
A744S/N 1 0.9
R761M/N 1 0.9
Total 116 100
Table4–MEFVgenotypedistributionamongFMFgroup andcontrolgroup.
FMFpatientgroup n=116
Controlgroup n=95
p-Value
G138Ggenepolymorphism(rs224224,c.414A>G)
<0.001
A/Agenotype 12(10.30) 30(65.70)
A/Ggenotype 50(43.10) 43(31.30)
G/Ggenotype 54(46.60) 22(3)
A165Agenepolymorphism(rs224223,c.495C>A)
<0.001
C/Cgenotype 12(10.30) 30(31.60)
C/Agenotype 53(45.70) 44(46.30)
A/Agenotype 51(44) 21(22.10)
100 90 80 70 60 50 40 32 68 A allele frequency (%) G allele frequency (%) 30 20 10 0 Control group FMF patient group 54 46
Fig.1–DistributionoftheallelefrequenciesofMEFVgene polymorphismsG138Ggenepolymorphism(rs224224, c.414A>G)intheFMFpatientandcontrolgroups.Thewhite barsrepresentthefrequencyoftheAallele,andthegray barsrepresentthefrequencyoftheGalleleinbothgroups.
polymorphismsandclinicalmanifestationsofthediseasein 116adultFMFpatientslivinginBursalocalizedinthe South-ernMarmararegionofTurkey.Wefoundsignificantlyhigher frequencyofGalleleofG138GandAalleleofA165A polymor-phisms.However,wecouldnotfindasignificantassociation betweenthesepolymorphismsandclinicalfeaturesinthese patients.
The estimated prevalence of the disease in Turkey is 0.1%.However,becausemanypatientsareundiagnosed,itis thoughtthattheprevalencemaybehigher.Adisease-specific laboratorytestforthediagnosisofFMFisnotyetavailable. Today, the diagnosis is provided on the basis of patient’s
100 90 80 70 60 50 40 33 67 30 20 10 0 Control group FMF patient group C allele frequency (%) A allele frequency (%) 55 45
Fig.2–DistributionoftheallelefrequenciesofMEFVgene polymorphismsA138Agenepolymorphism(rs224223, c.495C>A)intheFMFpatientandcontrolgroups.Thewhite barsrepresentthefrequencyoftheCallele,andthegray barsrepresentthefrequencyoftheAalleleinbothgroups.
clinicalfeaturessuchasclinicalfindings,ethnicity,family his-toryandcolchicineresponse,etc.10,16
ByTurkishFMFStudyGroup,clinicalfindingsinpatients older than 18 years are listed as follows; abdominal pain (93.7%),fever(92.5%),arthritis(27.1%)anderysipelas-likerash (10.4%). In another study by Kasifoglu et al., clinical find-ings were listed as abdominal pain (94.6%), fever (91.9%), arthritis(39.8%)anderysipelas-likerash(23.7%).17,18 Clinical signs/symptomsotherthanfeverareobservedinsimilarrates inthestudies.Becauseofregularuseofcolchicineand tak-ing nonsteroidal anti-inflammatorydrug withthe onset of abdominalpain,frequencyoffever maybedetermined rel-ativelylower.
Despitelackofinformationintermsofoverallmutation frequency in studies conducted inour country, the muta-tionfrequenciesofdifferentregionswerereportedinstudies fromthoseregions.TurkishFMFStudyGroupassessedmany patientsandhealthypeoplein2005.Accordingtothisreport, genetic analysiswas performedin 1090patientsand most commonmutationswere detectedintothefollowingrates, M694V51.4%,M680I14.4%andV726A 8.6%.17 Basedonthe studyconductedbyTurkishFMFStudyGroup,itisconsidered thatthegeneticdiagnosisofFMFcanbemadeby determina-tionofthesethreemutationsinthemajorityofpatients(about 74%).
InstudiesconductedinvariousregionsofTurkey,similar resultstotheratesspecifiedbyTurkishFMFStudyGrouphave beenreported.Gunesacaretal.19reportedthatthemost com-monmutationsin90patientsaroundC¸ukurovaregionwere M694V(51.66%),M680I (17.22%),V726A(10.55%),and M694I (1.66%). In a study made by Akar et al.20 in Central Ana-toliaRegion,mutationfrequenciesofM694V,M680I,V726A, and M694Iweredetermined as43.5%,12%,11.1%and2.8%, respectively.InanotherstudyfromErzurum,Ertekinetal.21 determinedM694V(51.3%)asthemostcommontypeof muta-tion.ItwasfollowedbyM680(7.3%),V726A(4.9%),E148Q(4.9%) andR761H(2.4%),respectively.Accordingtoastudymadeby Yilmazetal.22aroundAnkara,thefrequenciesofmutations inpatientswerefoundasfollows;51.55%M694V,9.22%M680I, 8.8%V726A,3.55%E148Q,and0.44%M694I.Inrecentstudies, themutationfrequenciesofM694V,M680I,V726Awere deter-minedas33.7%,15.5%,5%,respectivelybyYigitetal.23inBlack Searegion;themutationfrequenciesofM694V,E148Q,V726A, andM680Iweredeterminedas47.6%,16.75%,12.95%,11.94%, respectivelybyAkinetal.2intheAegeanregion.Inanother recentstudyfromAnkara,Do ˘ganetal.3 reportedthe muta-tionfrequenciesasfollows:42.05%M694V,19.27%E148Q,and 16.27%M680I.Inourstudy,mutationfrequenciesaresimilar totheresultsofTurkishFMFStudyGroup.
homozygousforM694Vmutationare atrisk ofearlyonset disease anddeveloping complicationofamyloidosis.18 Itis alsowell knownthatamyloidosisisariskforrenalfailure. It is reported that the initiation of colchicine significantly reducedcomplicationsinpatientsclinicallydiagnosedatan earlystage.25,26
In a report of Turkish FMF Study group, joint com-plaints were significantly more frequent in M694V/M694V homozygouspatientswhiletherewasnostaticallysignificant differenceincorrelationanalysisbetweenmutationsand clin-icalfindingssuchasfever,abdominalpain,andamyloidosis.17 Inourstudy,itiswasobservedthattherewasnostatically significant relation between mutation types and frequen-ciesofchronickidneydisease,amyloidosis,proteinuria,and symptoms like fever, abdominal pain, arthritis, arthralgia, erysipelas-like erythema. To our knowledge, our study is importantbecauseofbeingfirststudytoreportthefrequency ofMEFVmutationsintheSouthernMarmararegion.
Failureto set out exactly the genotype–phenotype rela-tionshipwiththeknown classicalmutations,hasattracted attentiontothepolymorphismsofwhichclinicalsignificance is not well-known. In literature, the relationship between polymorphismsofG138G(rs224224),A165A(rs224223),R202Q (rs224222)inexon2ofMEFVgeneanddiseaseandits compli-cationsisreportedinasmallnumberofpublications.14,15,27
Inastudyfromourcountry,Öztürketal.reportedthat car-riageofR202Qpolymorphismdidnothaveanyeffectsinterms ofFMFdisease,butalsoitwasstatedthatthemutationsin exon10ofthisgeneaffectedthesymptomsofthedisease.27
In a study by Akar et al.,15 124 patients with FMF and 81 healthy controlswere included and Ala138Gly polymor-phismwasinvestigated.Betweenpatientandcontrolgroups, therewasnostaticallysignificantdifferenceintermsofand Ala138Glypolymorphism. However,when 47 patients with amyloidosis were compared with other patients in whom amyloidosis was not detected, significant difference was observedintermsofAla138Glypolymorphismand polymor-phicalleleof138GlyinpatientswithFMFwasreportedtobe associatedwithamyloidosis.InthestudybyBasarslanetal.,14 the frequenciesofpolymorphic alleles ofG138G (rs224224) andA165A(rs224223)inpatientswerehigherthanthecontrol group.
Inourstudy,significantdifferencewasdetectedinterms ofG138G and A165Apolymorphisms in comparisonofthe patientsandhealthysubjects.Inaddition,inourstudy,unlike the other studies, relationship between G138G and A165A polymorphismsandclinicalfeaturessuchasfever,abdominal pain, arthritis/arthralgia, erysipelas-like erythema, chronic renaldisease,proteinuria,andamyloidosiswasinvestigated. However,therewasnostaticallysignificantassociation.Small numberofpatientsandpatients’ages(allofthemwereover 18)inourgroupmayhaveaffectedourresults.
Inthisstudytherewassignificantdifferencesbetweenthe patientandcontrolgroupsintermsofG138GandA165A poly-morphisms.These findingsneedtobeevaluatedinfurther studies withlargernumber ofcasesand follow-up data to determinetherelationshipbetweenphenotypeandthe impli-cationsforthedevelopmentofdiseasecomplicationsclearly. Amongthelimitationsofourstudyarethecrosssectional design,therelatively smallsamplesize,and smallnumber
of patientswith amyloidosis (7 patients), and exclusion of patientsunder18yearsold.Webelievethatfurtherstudies withlargersamplesizesandlongitudinaldesignareneeded toelucidatetheexactroleofmutationsandpolymorphisms intheclinicalcontextandtheprognosisofFMFpatients.
In conclusion, to our knowledge, our study is the first reportoftheSouthMarmararegiondeterminingfrequencies ofMEFVmutations,andthefrequenciesofMEFVmutations inourregionwereobservedatsimilarratesasinthe litera-ture.Besides,polymorphicallelesofG138GandA165Awere observed in a higher frequencyin FMF patients compared withcontrols.However,wedidnotobserve anyassociation betweenthesemutationsorpolymorphismsinthesepatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.EceA,C¸akmakE,UlucaÜ,Kelekc¸iS,Yolbas¸ ˙I,Günes¸A,etal. TheMEFVmutationsandtheirclinicalcorrelationsin childrenwithfamilialMediterraneanfeverinsoutheast Turkey.RheumatolInt.2014;34:207–12.
2.AkinH,OnayH,TurkerE,CoguluO,OzkinayF.MEFV mutationsinpatientswithFamilialMediterraneanFever fromtheAegeanregionofTurkey.MolBiolRep.2010;37: 93–8.
3.Do ˘ganHO,KocaY,ErdenG,KaraaslanY,BozatH.Evaluating MEFVmutationfrequencyinTurkishfamilialMediterranean feversuspectedpatientsandgendercorrelation:a
retrospectivestudy.MolBiolRep.2012;39:6193–6. 4.DundarM,EmirogullariEF,KirazA,TaheriS,BaskolM.
CommonFamilialMediterraneanFevergenemutationsina Turkishcohort.MolBiolRep.2011;38:5065–9.
5.Saatc¸iU,OzenS,OzdemirS,BakkalogluA,BesbasN, TopalogluR,etal.FamilialMediterraneanfeverinchildren: reportofalargeseriesanddiscussionoftheriskand prognosticfactorsofamyloidosis.EurJPediatr. 1997;156:619–23.
6.CaglayanAO,DemiryilmazF,OzyazganI,GumusH.MEFV genecompoundheterozygousmutationsinfamilial Mediterraneanfeverphenotype:aretrospectiveclinicaland molecularstudy.NephrolDialTransplant.2010;25:2520–3. 7.GulecCeylanG,TekedereliI.MEFVgenemutationsina
sampleofTurkishpopulation:aretrospectivestudy.Turkiye KlinikleriJMedSci.2011;31:1317–23.
8.OzalkayaE,MirS,SozeriB,BerdeliA,MutlubasF,CuraA. FamilialMediterraneanfevergenemutationfrequenciesand genotype-phenotypecorrelationsintheAegeanregionof Turkey.RheumatolInt.2011;31:779–84.
9.EtemEO1,DeveciSD,ErolD,YuceH,ElyasH.Familial Mediterraneanfever:aretrospectiveclinicalandmolecular studyintheEastofAnatoliaregionofTurkey.Open RheumatolJ.2010;29:1–6.
10.CeylanGG,CeylanC,OzturkE.Frequencyofalterationsinthe MEFVgeneandclinicalsignsinfamilialMediterraneanfever inCentralAnatolia,Turkey.GenetMolRes.2012;11:
1185–94.
12.JarjourRA.FamilialMediterraneanfeverinSyrianpatients: MEFVgenemutationsandgenotype-phenotypecorrelation. MolBiolRep.2010;37:1–5.
13.TopalogluR,OzaltinF,YilmazE,OzenS,BalciB,BesbasN, etal.E148Qisadisease-causingMEFVmutation:a phenotypicevaluationinpatientswithfamilial Mediterraneanfever.AnnRheumDis.2005;64:750–2. 14.BasarslanF,YengilE,GogebakanB.Evaluationofthepatients
withthediagnosisoffamilialMediterraneanfeverinclinical andgeneticaspects.SYMRNAMedJ.2013;2:1–6.
15.AkarE,YalcinkayaF,AkarN.IstheAla138Glyalterationof MEFVgeneimportantforamyloidosis?HumMutat. 2001;17:71.
16.TouitouI.ThespectrumoffamilialMediterraneanfever(FMF) mutations.EurJHumGenet.2001;9:473–83.
17.TuncaM,AkarS,OnenF,OzdoganH,KasapcopurO, YalcinkayaF,etal.,TurkishFMFStudyGroup.Familial Mediterraneanfever(FMF)inTurkey:resultsofanationwide multicenterstudy.Medicine(Baltimore).2005;84:
1–11.
18.KasifogluT,BilgeSY,SariI,SolmazD,SenelS,EmmungilH, etal.AmyloidosisanditsrelatedfactorsinTurkishpatients withfamilialMediterraneanfever:amulticentrestudy. Rheumatology(Oxford).2014;53:741–5.
19.GunesacarR,KasapH,ErkenE,OzerHT.Comparisonof amplificationrefractorymutationsystemandpolymerase chainreaction-restrictionfragmentlengthpolymorphism techniquesusedfortheinvestigationofMEFVgeneexon 10pointmutationsinfamilialMediterraneanfeverpatients
livinginC¸ukurovaregion(Turkey).GenetTest.2005;9: 220–5.
20.AkarN,MisirogluM,YalcinkayaF,AkarE,CakarN,TümerN, etal.MEFVmutationsinTurkishpatientssufferingfrom familialMediterraneanfever.HumMutat.2000;15:118–9. 21.ErtekinV,Selimo ˘gluMA,PirimI.FamilialMediterraneanfever
inachildhoodpopulationinEasternTurkey.PediatrInt. 2005;47:640–4.
22.YilmazE,OzenS,BalciB,DuzovaA,TopalogluR,BesbasN, etal.MutationfrequencyoffamilialMediterraneanfeverand evidenceforahighcarrierrateintheTurkishpopulation.Eur JHumGenet.2001;9:553–5.
23.YigitS,BagciH,OzkayaO,OzdamarK,CengizK,AkpolatT. MEFVmutationsinpatientswithfamilialMediterranean feverintheBlackSearegionofTurkey:Samsunexperience. JRheumatol.2008;35:106–13.
24.GiancaneG,TerHaarNM,WulffraatN,VastertSJ,BarronK, HentgenV,etal.Evidence-basedrecommendationsfor geneticdiagnosisoffamilialMediterraneanfever.Ann RheumDis.2015;74:635–41.
25.AkpolatT,ÖzkayaO,ÖzenS.HomozygousM694Vasarisk factorforamyloidosisinTurkishFMFpatients.Gene. 2012;492:285–9.
26.Yalc¸inkayaF,TekinM,TümerN,OzkayaN.Protracted arthritisoffamilialMediterraneanfever(anunusual complication).BrJRheumatol.1997;36:1228–30.