Abst ract
Submitted: March 10, 2017 0RGL¿FDWLRQ-XQH Accepted: June 27, 2017
Effect s of chlorhexidine
pre-procedural rinse on bact erem ia in
periodont al pat ient s: a random ized
clinical t rial
Obj ect ive: Single dose of syst em ic ant ibiot ics and short- t erm use of m outhwashes reduce bacterem ia. However, the effects of a single dose of pre-procedural rinse are still controversial. This study evaluated, in periodontally diseased pat ient s, t he effect s of a pre- procedural m out h rinse on induced bact erem ia. Mat erial and Met hods: Syst em ically healt hy individuals wit h gingivit is ( n= 27) or periodont it is ( n= 27) were random ly allocat ed t hrough a sealed envelope syst em t o: 0.12% chlorhexidine pre- procedural rinse ( 13 gingivit is and 13 periodont it is pat ient s) or no rinse before dent al scaling ( 14 gingivit is and 15 periodont it is pat ient s) . Periodont al probing dept h, clinical attachm ent level, plaque, and gingival indices were m easured and subgingival sam ples were collect ed. Blood sam ples were collect ed before dent al scaling, 2 and 6 m inut es aft er scaling. Tot al bact erial load and levels of P. gingivalis were det erm ined in oral and blood sam ples by real- t im e polym erase chain react ion, while aerobic and anaerobic count s were det erm ined by cult ure in blood sam ples. The prim ary out com e was t he ant im icrobial effect of t he pre- procedural rinse. Dat a was com pared by Mann-Whit ney and Signal t est s ( p< 0.05) . Result s: I n all sam pling t im es, polym erase chain react ion revealed higher blood bacterial levels than culture (p< 0.0001), while gingivitis pat ient s present ed lower bact erial levels in blood t han periodont it is pat ient s ( p< 0.0001) . I ndividuals who experienced bact erem ia showed worse m ean clinical attachm ent level ( 3.4 m m vs. 1.1 m m ) and m ore subgingival bacteria ( p< 0.005) . The pre- procedural rinse did not reduce induced bact erem ia. &RQFOXVLRQV %DFWHUHPLD ZDV LQÀXHQFHG E\ SHULRGRQWDO SDUDPHWHUV ,Q periodont ally diseased pat ient s, pre- procedural rinsing showed a discret e effect on bact erem ia cont rol.
Ke yw or ds: Bact erem ia. Periodont al diseases. Periodont al debridem ent . Mout hwashes.
Rodrigo Dalla Pria BALEJO1 José Roberto CORTELLI2 Fernando Oliveira COSTA3 Renata Magalhães CYRINO3 Davi Romeiro AQUINO2 Karina COGO-MÜLLER4 Taís Browne MIRANDA1 Sara Porto MOURA1 Sheila Cavalca CORTELLI2
http://dx.doi.org/10.1590/1678-7757-2017-0112
1Universidade de Taubaté, Departamento de Odontologia, Taubaté, SP, Brasil.
2Universidade de Taubaté, Departamento de Odontologia, Núcleo de Pesquisa Periodontal, Taubaté,
SP, Brasil.
3Universidade Federal de Minas Gerais, Faculdade de Odontologia, Belo Horizonte, MG, Brasil. 4Universidade Estadual de Campinas, Faculdade de Ciências Farmacêuticas, Piracicaba, SP, Brasil.
I nt roduct ion
Per iod on t al d iseases con t r ib u t e t o sy st em ic
GLVRUGHUVWKDWLQYROYHLQÀDPPDWRU\PHGLDWRUVLQWKH
bloodstream and the m igration of m icroorganism s and t heir product s t hroughout t he body14,15. Bact erem ia
can be induced by sim ple daily habit s such as oral hygiene14,16 and m ast icat ion6,9 or by m ore invasive
procedures such as dental scaling13,14,20,30. The intensity RILQMXU\PLFURELRWDSUR¿OHVHYHULW\RILQÀDPPDWLRQ
and local infect ion affect bact erem ia27. This part ially
ex plain s w hy per iodon t al diseases con t r ibu t e t o bact er em ia dev elopm ent . How ev er, a sy st em at ic r ev iew in dicat ed t h at t h e h et er ogen eit y of h igh m et hodological qualit y st udies im paired com parat ive analysis, leading t he aut hors t o not e t he need for random ized, cont rolled clinical t rials t o provide m ore accurat e dat a about bact erem ia in periodont ics13.
Over t he year s, oral bact er ia have developed m echanism s t o invade and persist in t he host cells, escape host im m une surveillance, adapt t o niches at
H[WUDRUDOVLWHVDQGLQGXFHLQÀDPPDWRU\UHVSRQVHV
leading t o adverse syst em ic effect s. I n conj unct ion, av ai l ab l e ev i d en ce co r r o b o r at es t h e v i ew t h at periodont it is act s as a biologically plausible risk fact or for syst em ic diseases. I n fact , t ransient bact erem ia, syst em ic inj ury by free t oxins of oral pat hogens, and
V\VWHPLF LQÀDPPDWLRQ FDXVHG E\ VROXEOH DQWLJHQV
of oral pat hogens have been im plicat ed in t he link between oral and system ic conditions. However, there is no clear underst anding of t he m echanism s of oral
EDFWHULD LQ H[WUDRUDO LQIHFWLRQV DQG LQÀDPPDWLRQ
which lim it s effect ive t herapies. Therefore, reduct ion of t he ent rance of bact eria and t heir product s in blood st ream could represent a reliable healt h care t ool11,21.
Pre- procedural rinses are used t o reduce cross-in fect ion8 , 1 0 , 1 6, an d, based on t h eir an t im icr obial
propert ies, it is reasonable t o expect a posit ive effect on bact erem ia. However, random ized clinical t rials invest igat ing t he effect s of pre- procedural rinses on bact erem ia are scarce.
We hy pot h esised t h at su scept ible in div idu als undergoing m anual dental scaling develop bacterem ia, which could be reduced em ploying a pre- procedural rinse. Therefore, this study evaluated whether a single dose of pre- procedural m out hrinse in periodont ally diseased pat ient s r educes bact er em ia st im ulat ed by m anual dent al scaling. We also analy zed t he occurrence and m agnitude of bacterem ia based on the
result s from cult ure and real- t im e polym erase chain react ion ( PCR) t echniques.
Mat erial and m et hods
Trial design
Th is r an dom ized, dou ble- blin d, sin gle- cen t er, parallel clinical trial was conducted at the University of Taubaté, Brazil, from August 2014 to Decem ber 2014. This st udy was regist ered at Clinicalt rials.gov ( NCT NCT02215473) and was approved by t he I nst it ut ional Et hics Com m it t ee ( prot ocol 521/ 10) . The pilot st udy was et hically approved under t his sam e prot ocol. All part icipant s provided an inform ed consent form .
St udy populat ion
Syst em ically healt hy individuals ( 18 and 45 years) diagnosed wit h eit her plaque- relat ed gingivit is1 or
m oderat e chronic periodont it is1, m ale or fem ale, wit h
at least 20 nat ural t eet h, wit h no need for ant ibiot ic prophylaxis, and wit h clinical indicat ion for dent al scaling, com posed t he st udy populat ion ( Figure 1) . A single calibrat ed ( kappa= 0.84 for periodont al probing dept h – PD and 0.82 for clinical at t achm ent level – CAL) exam iner m easured PD, CAL, plaque ( Pl)25, and
gingival indices ( GI )17 at four sit es per t oot h using
a m anual per iodont al pr obe( PCPUNC, Hu- Fr iedy, Chicago, I L, USA) . One panoram ic radiograph was obt ained for each pat ient .
Ex clu sion cr it er ia w er e: h ist or y of sy st em ic diseases; current ant ibiot ic t herapy or ant ibiot ic use in t he past 3 m ont hs; use of im m unosuppressant s; regular ant isept ic use in t he past 3 m ont hs; furcat ion lesions; periodont al t reat m ent 12 m ont hs preceding the start of the study; and rem ovable dentures, braces and risk condit ions for bact erem ia.
The sam ple size calculat ion was det erm ined based on a previous study6 and adj usted after the pilot study
( n= 2 per group) t hat included t he processing of
real-t im e PCR. Volunreal-t eers from real-t he piloreal-t sreal-t udy did noreal-t part icipat e in t he m ain st udy. The m inim um num ber of 12 individuals per group was designed t o provide
SRZHUDQGDVLJQL¿FDQFHOHYHO
According t o periodont al condit ion, t wo blocks of patients were random ly allocated to one of two groups by opaque closed and num bered envelopes containing
LGHQWL¿FDWLRQVIRUHLWKHUWKHSUHSURFHGXUDOULQVHRU
Bacterem ia induction and periodontal treatm ent
Two trained periodontists carried out the periodontal t reat m ent . Pre- procedural rinse and non- rinse groups w er e b ook ed on sep ar at e d ay s. At b act er em ia induct ion, t he individuals at t ended in t he m orning wit hout oral hygiene aft er 8 hours of no food or drink, except wat er. Part icipant s in t he pre- procedural rinse groups perform ed a single rinse wit h 15 m L of 0.12% chlorhexidine ( Periogard®, Colgat e- Palm olive, São
Bernardo do Cam po, SP, Brazil) for 30 seconds and were im m ediat ely anest het ized, and 3 m inut es aft er rinsing t he scaling and root planning was perform ed
ZLWK*UDFH\DQG0F&DOOFXUHWWHVDQG+LUVFK¿HOGW\SH ¿OHV 7KLV SUHOLPLQDU\ VFDOLQJ DLPHG DW VWLPXODWLQJ
bact erem ia, st art ed in t he sam pled sit es and was ext ended t o t he ent ire dent al hem i- arch wit hin 6 m inut es. Per iodont al t r eat m ent was concluded in addit ional visit s according t o individual needs.
%LR¿OPDQGEORRGVDPSOLQJ
One hour prior t o t he induct ion of bact erem ia, subgingival sam ples were collect ed5 and st ored at
- 8 0 ° C in em pt y m in it u bes. Blood sam ples w er e collect ed6 at 3 sequent ial t im es: before dent al scaling
( T0) , 2 m inut es ( T1) , and 6 m inut es ( T2) aft er dent al scaling had st art ed. At each t im e, 2 m L of peripheral blood was collect ed int o cit rat ed vacuum t ubes, which w er e slight ly agit at ed t o pr event t he blood fr om coagulat ing. One m illilit er was pipet t ed from t he t ube and poured int o a second t ube cont aining 1 m L of a 1% st erile solut ion of sodium polyanet hol sulfonat e (Sigm a Chem ical Co., St. Louis, MO, USA) to deactivate com plem ent prot eins. The addit ional 1 m L was st ored at - 80° C unt il PCR processing.
Real- t im e PCR procedures
p er i o d o n t o p a t h o g en P. g i n g i v a l i s, a r ea l - t i m e quant it at ive PCR ( qPCR) t echnique was carried out
LQ D Nj/ UHDFWLRQ YROXPH 7KH F\FOLQJ FRQGLWLRQV
were: 95° C for 10 m inut es, 40 cycles at 95° C for 15 seconds, and 60° C for 1 m inut e. I n t he negat ive cont r ol, t he DNA sam ple was r eplaced by st er ile Milli- Q wat er. The prim er/ probe sequences were: P. gingiv alis – forward: ACCTTACCCGGGATTGAAATG; r e v e r s e : C A A C C AT G C A G C A C C TA C ATA G A A ; p r ob e: ATGACTGATGGTGAAAACCGTCTTCCCTTC; r ef er en ce st r ain : W8 3 an d t ot al b act er ial load
– f o r w a r d : T G G A G C AT G T G G T T TA AT T C G A ; r e v e r s e : TG CG G G A CTTA A CCCA A CA ; p r o b e : CACGAGCTGACGACA( AG) CCATGCA; reference strain:
E. coli ATCC- 25922. St andard curves, using a known
am ount of each bact erial species ( 101- 108 cells) , were
em ployed t o convert t he cycle t hreshold values ( CT) int o t he num ber of bact erial cells in t he sam ples.
Bact erial cult ure procedures
I m m ediat ely aft er collect ion, blood sam ples were spread out ont o agar plat es in duplicat e6,9. Trypt ic Soy
Agar ( TSA) , incubat ed for 2 days at 35° C, was used t o det erm ine t ot al aerobic count s, while Schaedler Blood Agar ( SBA) , incubat ed for 5- 7 days at 35° C in an anaerobic cham ber, was used t o det erm ine t ot al anaer obic count s. Bact er ial colony- for m ing unit s ( CFU) were counted by an autom ated colony- counting
syst em by a single researcher.
St at ist ical analysis
Bact erem ia occurrence ( presence and/ or increase of bact er ial levels in t he blood) w as det er m ined according t o dent al scaling. I n addit ion, bact erem ia data was com pared between the groups ( gingivitis vs. periodont it is) and am ong t he t im es of sam pling ( pre- and post- scaling) . The associat ion bet ween oral and blood bact erial levels and bet ween PD and CAL and bact erem ia were st at ist ically analyzed. The bact erial levels det erm ined by bot h laborat orial t echniques were com pared.
The prim ary out com e was t he ant im icrobial effect of a single m out h rinse use. To check t his effect on bact erem ia, t he levels of viable anaerobic and aerobic bact erial cells were com pared bet ween 0 ( T0) and 2 ( T1) m inut es, 0 ( T0) and 6 ( T2) m inut es, and 2 ( T1) and 6 ( T2) m inut es. Bact erial levels at 2 and 6 m inut es were com pared am ong t he volunt eers who perform ed the pre- procedural rinse and those who did not. As a secondary analysis, sim ilar com parisons were perform ed considering t he qPCR result s.
Mann-Whit ney and Signal t est s were used in t he above- m ent ioned com parisons ( p< 0.05) . Dat a from t he int ent ion- t o- t reat analysis did not differ from t he
per prot ocol analysis.
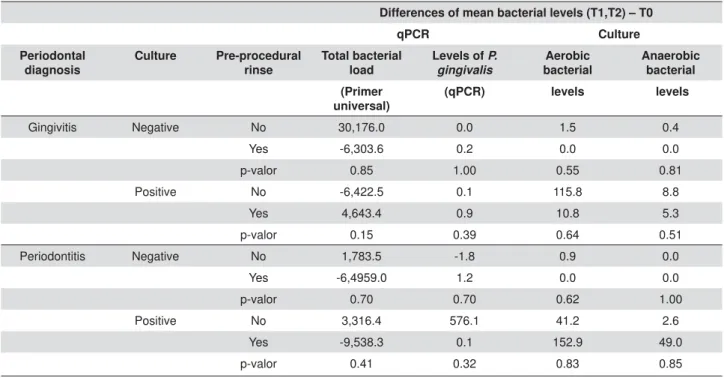
Differences of mean bacterial levels (T1,T2) – T0
qPCR Culture
Periodontal diagnosis
Culture Pre-procedural
rinse
Total bacterial load
Levels of P. gingivalis
Aerobic bacterial
Anaerobic bacterial
(Primer universal)
(qPCR) levels levels
Gingivitis Negative No 30,176.0 0.0 1.5 0.4 Yes -6,303.6 0.2 0.0 0.0 p-valor 0.85 1.00 0.55 0.81 Positive No -6,422.5 0.1 115.8 8.8 Yes 4,643.4 0.9 10.8 5.3 p-valor 0.15 0.39 0.64 0.51 Periodontitis Negative No 1,783.5 -1.8 0.9 0.0 Yes -6,4959.0 1.2 0.0 0.0 p-valor 0.70 0.70 0.62 1.00 Positive No 3,316.4 576.1 41.2 2.6 Yes -9,538.3 0.1 152.9 49.0 p-valor 0.41 0.32 0.83 0.85
0DQQ:KLWQH\WHVWSUHSURFHGXUDOULQVHSRVLWLYHYVQHJDWLYH5HVXOWVZHUHFRQVLGHUHGVWDWLVWLFDOO\VLJQL¿FDQWZKHQS
Result s
Am ong t he 2 7 per iodont it is and 2 6 gingiv it is
LQGLYLGXDOVZKRFRPSRVHGWKH¿QDOVWXG\SRSXODWLRQ
4 9 % u n der w en t a pr e- pr ocedu r al or al r in se. To evaluate the effect of the pre-procedural rinse on blood bact erial levels, differences bet ween t he m ean values observed at T1–T2 and T0 were calculated, considering bot h t he qPCR and cult ure result s. We com pared t he m ean values of individuals who rinsed t o t hose who had not rinsed. Pre- procedural rinsing did not affect t he levels of bact eria in t he blood sam ples of bot h periodont it is and gingivit is individuals ( Table 1) .
Tot al bact erial levels and levels of P. gingivalis in
blood sam ples were com pared between the periodontal diagnoses ( gingiv it is v s. per iodont it is) . Gingiv it is pat ient s exhibit ed lower blood bact erial levels, as dem onstrated by both culture and qPCR at all sam pling t im es ( T0, T1 and T2) ( p< 0.0001; Mann-Whit ney t est ) . The levels of P. gingivalis were det erm ined by
qPCR and differed between gingivitis and periodontitis patients only at T2 ( 0.3 from gingivitis and 512.5 from periodont it is sam ples) ( Table 2) .
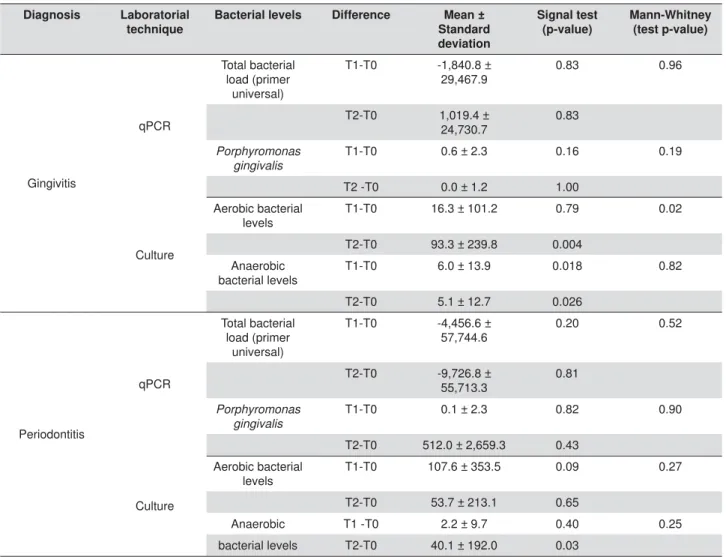
To ident ify whet her t here was a bet t er t im e for sam pling, w e calculat ed t he differ ences bet w een T1 and T0 values and bet ween T2 and T0 values. Therefore, we checked whether a progressive increase or decr ease occur r ed ov er t im e. For T2, cult ur e bact er ial count s fr om gingiv it is pat ient s show ed 93.3 m ore bact eria ( CFU) t han T0, indicat ing t hat 6
m inut es aft er t he beginning of dent al scaling is t he best t im e t o ident ify bact erem ia. At t his sam e t im e, t he cult ure result s from periodont it is pat ient s only show ed differ ences r egar ding anaer obic bact er ia. For P. gingivalis, t heqPCR result s did not reveal any differences am ong sam pling t im es ( Table 3) .
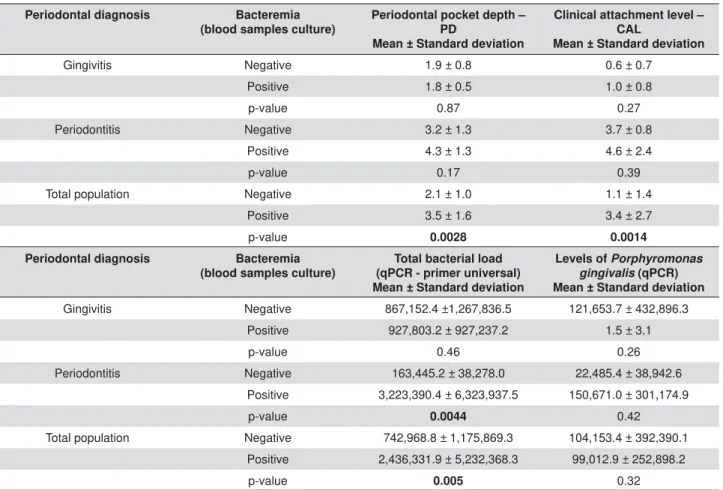
PD and CAL were com pared bet ween posit ive and negat ive bact erem ia individuals. For t he whole st udy populat ion, t he m ean values differed according t o t he occurrence of bact erem ia ( Mann-Whit ney t est ; p= 0.0028 for PD and p= 0.0014 for CAL) . PD and CAL were higher am ong individuals who exhibit ed posit ive blood sam ples in cult ure ( PD 3.5 m m vs. 2.1 m m and CAL 3.4 m m vs. 1.1 m m ) . Wit hin each periodont al diagnosis, w e did not obser ve sim ilar differ ences ( p> 0.05) ( Table 4) .
We a l so i n v est i g a t ed t h e r el a t i o n b et w een
VXEJLQJLYDO EDFWHULDO SUR¿OHV WRWDO EDFWHULDO ORDG
and P. gingivalis) and bact erem ia. I ndividuals who
experienced bact erem ia show ed m ore bact eria in subgingival sam ples ( Mann-Whit ney t est ; p< 0.005) . I n addition, periodontitis individuals who were positive for bact erem ia also showed higher t ot al bact erial levels in the subgingival area ( p= 0.004) . On the other hand, t here was no associat ion bet ween levels of subgingival bact eria and bact erem ia am ong gingivit is individuals. I solat ed, t he levels of P. gingivalis did not
vary according t o bact erem ia occurrence ( Table 4) .
Laboratorial technique
Diagnosis N T0 T1 T2
qPCR
Total bacterial load (primer
universal)
Levels of P. gingivalis
(qPCR)
Total bacterial load (primer
universal)
Levels of P. gingivalis
(qPCR)
Total bacterial load (primer
universal)
Levels of P. gingivalis
(qPCR) Gingivitis 27 7,353.2 0.2 45,512.4 0.9 48,372.7 0.3 Periodontitis 27 18,898.9 0.5 76,442.3 0.6 71,172.1 512.5
Mann-Whitney (p-value)
<0.0001 0.38 <0.0001 0.0874 <0.0001 0.0036
Culture
Diagnosis 27 Aerobic bacterial
levels
Anaerobic bacterial levels
Aerobic bacterial levels
Anaerobic bacterial levels
Aerobic bacterial levels
Anaerobic bacterial
levels Gingivitis 27 7.4 0.6 23.7 6.6 100.7 5.7 Periodontitis 113.8 142.3 521.5 744.5 467.5 782.4
Mann-Whitney (p-value)
<0.0001 0.0046 <0.0001 0.0099 <0.0001 0.0035
Mann-Whitney test (quantitative polymerase chain reaction - qPCR vs. culture for gingivitis and periodontitis). A difference was statistically
Discussion
Bacterem ia is the presence of viable m icroorganism s in t he blood st ream . I n t he presence of periodont al diseases, t he dam aged t issues cont ribut e t o bact erial dissem inat ion from oral sit es t hroughout t he body, linking oral healt h t o syst em ic healt h. Therefore, it seem s relevant t o st udy t he relat ion of bact erem ia t o periodont al st at us and dent al scaling. Furt her, few st udies have invest igat ed t he cont rolling effect of t he pre- procedural rinse on induced bact erem ia.
Despit e it s usual spont aneous resolut ion, am ong syst em ically com prom ised individuals, bact erem ia is t h e m ain cau se of sep t ic sh ock3. Reg ar d less
of t heir pat hogenic pot ent ials in t he oral cav it y, once colonized in t he ext ra- oral sit es, oral bact eria oft en becom e ERQD ¿GH pat hogens, especially in im m une- com prom ised individuals, causing disease m anifest at ion. Oral bact eria had been involved wit h
m any syst em ic condit ions, such as respirat ory t ract infect ions, m eningit is, and brain, lung, liver, and splenic abscesses11.
Dent al scaling was associat ed wit h higher blood bact erial levels at bot h 2 ( 60,977.3) and 6 m inut es ( 59,722.4) , as revealed by qPCR. We observed a sim ilar increase regarding t ot al count s of aerobic and anaerobic viable bact eria ( 648.20 at 2 m inut es and 678.20 at 6 m inut es) . According t o Horliana, et al.13
( 2014) , approxim at ely half ( 49.4% ) of periodont al procedures induce bact erem ia. Periodont al probing and dent al scaling cause bact erem ia by st im ulat ing soft diseased t issues in t he per iodont al pocket14.
Therefore, periodont al diseases are a predisposing factor for bacterem ia due to the infectious environm ent of t he periodont al pocket and t he lack of epit helial in t eg r it y1 6. I n t h is st u d y, t h e r elat ion b et w een SHULRGRQWDOEUHDNGRZQDQGEDFWHUHPLDZDVFRQ¿UPHG
Pat i en t s w i t h p o si t i v e cu l t u r ed b l o o d sam p l es
Diagnosis Laboratorial
technique
Bacterial levels Difference Mean ±
Standard deviation
Signal test (p-value)
Mann-Whitney (test p-value)
Gingivitis
qPCR
Total bacterial load (primer
universal)
T1-T0 -1,840.8 ±
29,467.9 0.83 0.96
T2-T0 1,019.4 ± 24,730.7
0.83
Porphyromonas gingivalis
T1-T0 0.6 ± 2.3 0.16 0.19
T2 -T0 0.0 ± 1.2 1.00
Culture
Aerobic bacterial levels
T1-T0 16.3 ± 101.2 0.79 0.02
T2-T0 93.3 ± 239.8 0.004 Anaerobic
bacterial levels T1-T0 6.0 ± 13.9 0.018 0.82 T2-T0 5.1 ± 12.7 0.026
Periodontitis
qPCR
Total bacterial load (primer
universal)
T1-T0 -4,456.6 ±
57,744.6 0.20 0.52
T2-T0 -9,726.8 ± 55,713.3
0.81
Porphyromonas gingivalis
T1-T0 0.1 ± 2.3 0.82 0.90
T2-T0 512.0 ± 2,659.3 0.43
Culture
Aerobic bacterial
levels T1-T0 107.6 ± 353.5 0.09 0.27 T2-T0 53.7 ± 213.1 0.65
Anaerobic T1 -T0 2.2 ± 9.7 0.40 0.25 bacterial levels T2-T0 40.1 ± 192.0 0.03
Signal test checked if the following differences, T1–T0 and T2–T0, were different from zero. Mann-Whitney test compared difference T1–
7ZLWKGLIIHUHQFH7±75HVXOWVZHUHFRQVLGHUHGVWDWLVWLFDOO\VLJQL¿FDQWZKHQSFRQ¿GHQFHLQWHUYDO
Table 3- Mean difference between time samplings (T1–T0) and (T2–T0) for all monitored bacterial levels according to periodontal diagnosis
show ed w orse periodont al clinical st at us ( PD and CAL) . I n addit ion, periodont al diagnosis im pact ed t he m agnit ude of bact erem ia. Periodont it is pat ient s showed higher blood bact erial levels ( cult ure and qPCR) t han gingivit is pat ient s. Kinane, et al.14 ( 2005)
also observed t hat t he incidence and m agnit ude of
EDFWHUHPLDZHUHVLJQL¿FDQWO\KLJKHULQSHULRGRQWLWLV
t han in gingivit is pat ient s. Moreover, 6 m inut es aft er scaling, periodont it is pat ient s also exhibit ed higher blood levels of P. gin giv alis. Aft er dent al scaling,
ot her aut hor s found P. g in g iv alis t o be am ongst
t he m ore frequent periodont al bact erial species in cult ivat ed blood sam ples20,22. Furt her, P. gingiv alis
DNA is frequent ly found in non- oral sit es – such as atherom atous plaques – in patients with periodontitis, suggesting a translocation from oral sites26. I n addition,
st udies suppor t a r ole for P. g in g iv alis- m ediat ed periodontal disease as a risk factor for several system ic diseases including diabetes, preterm birth, stroke, and at herosclerot ic cardiovascular disease12.
Mechanical procedures, such as t hose t est ed in t his st udy, are com m only used as part of periodont al
t h er ap y. I n ad d i t i on , p er i od on t al d i seases ar e associat ed wit h higher levels of subgingival bact eria5, ZKLFKEDVHGRQWKLVVWXG\FRXOGLQÀXHQFHEDFWHUHPLD
Ou r f i n d i n g s d em o n st r a t ed t h a t p a t i en t s w h o experienced bact erem ia had higher bact erial levels
LQVXEJLQJLYDOELR¿OPVDPSOHV7KLV¿QGLQJVKRXOGEH
furt her invest igat ed in fut ure st udies.
Bact erem ia is a t ransit ory event . Most posit ive
EORRGVDPSOHVDUHLGHQWL¿HGEHWZHHQVHFRQGVDQG
5 m inut es aft er dent al scaling27, and no m ore t han
30 m inut es30. However, t he t im e of sam pling is st ill a
critical aspect of bacterem ia research. I n this study, for gingivit is pat ient s, 6 m inut es was t he ideal sam pling tim e for identifying viable bacteria. This sam e sam pling t im e was t he best for ident ifying anaerobic viable bacteria am ong periodontitis individuals. On the other
KDQGWKHEDFWHULDOWLPHRIVDPSOLQJKDGQRLQÀXHQFH
on bact erial DNA ( qPCR – t ot al bact erial load and P.
gingivalis) in bot h periodont al diagnoses. Therefore,
t his st udy failed t o ident ify an ideal sam pling t im e for bot h t echniques and bot h periodont al diagnosis. The inclusion of a low num ber of t im es of sam pling
Periodontal diagnosis Bacteremia
(blood samples culture)
Periodontal pocket depth – PD
Mean ± Standard deviation
Clinical attachment level – CAL
Mean ± Standard deviation
Gingivitis Negative 1.9 ± 0.8 0.6 ± 0.7 Positive 1.8 ± 0.5 1.0 ± 0.8
p-value 0.87 0.27
Periodontitis Negative 3.2 ± 1.3 3.7 ± 0.8 Positive 4.3 ± 1.3 4.6 ± 2.4
p-value 0.17 0.39
Total population Negative 2.1 ± 1.0 1.1 ± 1.4 Positive 3.5 ± 1.6 3.4 ± 2.7
p-value 0.0028 0.0014
Periodontal diagnosis Bacteremia
(blood samples culture)
Total bacterial load (qPCR - primer universal) Mean ± Standard deviation
Levels of Porphyromonas gingivalis (qPCR) Mean ± Standard deviation
Gingivitis Negative 867,152.4 ±1,267,836.5 121,653.7 ± 432,896.3 Positive 927,803.2 ± 927,237.2 1.5 ± 3.1
p-value 0.46 0.26
Periodontitis Negative 163,445.2 ± 38,278.0 22,485.4 ± 38,942.6 Positive 3,223,390.4 ± 6,323,937.5 150,671.0 ± 301,174.9
p-value 0.0044 0.42
Total population Negative 742,968.8 ± 1,175,869.3 104,153.4 ± 392,390.1 Positive 2,436,331.9 ± 5,232,368.3 99,012.9 ± 252,898.2
p-value 0.005 0.32
0DQQ:KLWQH\WHVWEDFWHUHPLDSRVLWLYHYVEDFWHUHPLDQHJDWLYH5HVXOWVZHUHFRQVLGHUHGVWDWLVWLFDOO\VLJQL¿FDQWZKHQS FRQ¿GHQFHLQWHUYDO
Table 4- Comparative mean periodontal clinical (periodontal pocket depth – PD and clinical attachment level – CAL) and microbiological
represent s a lim it at ion of t he st udy.
Regardless of t im e, t he levels of bact eria were higher when t he sam ples were analyzed by qPCR. To ident ify bact erem ia, Kinane, et al.14 ( 2005) com bined
t w o labor at or ial t ech n iqu es. Ev en t h ou gh t h ese aut hors used convent ional PCR, cult ures revealed t he lowest bact erem ia rat e. Chang, et al.4 ( 2013)
published a syst em at ic review on t he subj ect and point ed out t hat PCR is an appropriat e research t ool for st udying bact erem ia. However, Benit éz- Páez, et al.2 ( 2013) highlight ed t hat , in induced bact erem ia, UHVHDUFKHUVGRQRWDOZD\V¿QGHQRXJK'1$IRU3&5 DPSOL¿FDWLRQ,QWKHVWXG\E\0DUtQHWDO19 ( 2016)
neither culture nor qPCR detected any type of bacteria in t he blood sam ples, while Rat t o-Tespest ini, et al.23
( 2016) did not observe any superiority by qPCR over cult ure. Based on t his concept , w hen possible, it seem s reasonable t o com bine cult ures and m olecular analyses to clarify unanswered questions. However, in t his st udy, t he com binat ion of t wo t echniques enabled
WKH LGHQWL¿FDWLRQ RI WRWDO YLDEOH EDFWHULD DQG WRWDO
bact erial DNA, for P. gingiv alis no PCR procedures
were able t o ident ify viable bact eria cells. This could be int erpret ed as anot her lim it at ion of t his st udy t o be handled in t he fut ure.
Healt h car e pr ocedu r es, su ch as per iodon t al t h e r a p e u t i c s c a l i n g , c a n i n d u c e t r a n s i t o r y bact erem ia13,14. I n dent ist ry, t he use of ant im icrobial
m out hrinses has different aim s, however, t he num ber of st u d ies ev alu at in g t h e ef f ect iv en ess of p r e-procedural rinses on bact erem ia is scarce, especially when considering RCT design in periodont al research. Du e t o it s w ell- k n ow n an t im icr obial pr oper t ies, 0.12% chlorhexidine is one of t he m ost recom m end pre- procedural m out hrinse29. Therefore, t his st udy
evaluat ed blood bact erial levels aft er dent al scaling, according t o pre- procedural rinse. Unfort unat ely, a single 0.12% chlorhexidine pre- procedural rinse failed to reduce bacterem ia occurrence am ong periodontally diseased individuals. Sim ilarly, DuVall, et al.7 ( 2013)
and Maharaj, et al.18 (2012) did not observe a decrease
in bact erem ia rat es using t his sam e pre- procedural rinse. I n the study by Maharaj, et al.18 (2012), patients
were random ly assigned to 0.12% chlorhexidine rinse, syst em ic ant ibiot ics, or cont rol. The cont rol group received no int ervent ion before dent al ext ract ion. Sim ilarly, t his st udy did not int ervene before dent al scaling in t he cont rol group. Maharaj , et al.18 ( 2012)
found no difference bet ween t he rinse and cont rol
groups regarding bact erem ia. DuVall, et al.7 ( 2013)
random ized their patients into m outhrinse, antibiotics, or cont rol. I n t his part icular st udy, t he cont rol group was given a placebo. There is no clear inform at ion as t o whet her t he m ent ioned placebo was in t he form of capsules or rinse. I n t his st udy, however, we decided not t o use a placebo rinse because previous st udies report ed increased bact erial count s in cult ures aft er a 15- day placebo use6,9. I n fut ure st udies, we shall
handle t his lim it at ion. On t he ot her hand, wit h a higher concent rat ion of chlorhexidine ( 0.2% ) , Tuna, et al.28 ( 2012) report ed a reduct ion in t he incidence of
bact erem ia following dent al ext ract ion. Am ong t hese last st udies, only ours m onit ored periodont al st at us, w hich could have par t ially affect ed t he obser ved r esult s. Sahr m ann, et al.24 ( 2015)also evaluat ed
t he periodont al clinical st at us of a st udy populat ion com posed of per iodont it is pat ient s subm it t ed t o periodont al inst rum ent at ion wit h wat er or PVP- iodine rinse. Oral borne bact erem ia was observed in 53% of t he cont rol group and in 11% of t he t est group.
%DFWHUHPLDVLJQL¿FDQWO\UHGXFHGDIWHU393LRGLQHXVH
Based on t his st udy, alt hough it is relevant for cr oss- infect ion cont r ol8 , 1 0, pr e- pr ocedural r insing
show ed lim it ed clinical r elevance for bact er em ia cont rol. I nt erest ingly, t he result s from t he daily use of m out hrinse can differ from t hose observed aft er a single use. An essent ial- oil m out hrinse used for 15 days reduced bacterem ia after m astication in gingivitis indiv iduals6, 9. How ev er, in per iodont it is pat ient s,
subgingival irrigat ion wit h essent ial- oils com bined wit h one-week rinsing was not enough t o decrease bact erem ia following quadrant scaling20. Therefore,
it could be speculat ed t hat t o reduce bact erem ia, ant im icrobials would be prescribed 15 days before dent al scaling and possibly cont inued for t he durat ion
RIWKHWUHDWPHQW6SHFL¿FDOO\DSUHSURFHGXUDOULQVH
should be done aim ing to control aerosol contam ination and int ra- oral infect ion.
appr opr iat e m an agem en t of bact er ial biof ilm in t he subgingival ar ea could cont r ibut e t o pr event bact er em ia in per iodont ally diseased indiv iduals. Pre- procedural rinse did not reduce, effect ively, levels of bact er ia in t he blood. Ot her st rat egies should be adopt ed t o reduce bact erem ia in periodont ally diseased individuals.
Conclusions
Dental scaling induced bacterem ia in both gingivitis and periodont it is. However, bact erem ia increased as periodontal com prom ising increased. The m agnitude of bact erem ia was great er am ong periodont it is pat ient s. I n periodont ally diseased pat ient s, pre- procedural rinsing showed a discrete effect on bacterem ia control.
Funding st at em ent
7KLVUHVHDUFKZDV¿QDQFLDOO\VXSSRUWHGE\&13T ± 1DWLRQDO &RXQFLO IRU 6FLHQWL¿F DQG 7HFKQRORJLFDO
Developm ent , Federal Dist rict , Brazil – Product ivit y Research fellows PQ and PROCAD grant 552264/
7KH IXQGLQJ VRXUFH KDG QR LQÀXHQFH RQ VWXG\
design; collect ion, analy sis and int er pr et at ion of dat a; writ ing and subm ission of t he report ; and in t he decision t o subm it t he art icle for publicat ion.
References
$UPLWDJH*&'HYHORSPHQWRIDFODVVL¿FDWLRQV\VWHPIRUSHULRGRQWDO diseases and condit ions. Ann Periodont ol. 1999; 4: 1- 6.
2- Benit éz- Páez A, Álvarez M, Belda- Ferre P, Rubido S, Mira A, Tom ás I . Det ect ion of t ransient bact eraem ia following dent al ext ract ions by 16S rDNA pyrosequencing: a pilot st udy. PLoS One. 2013; 8: e57782. 3- Cart er C. I m plem ent ing t he severe sepsis care bundles out side t he I CU by out reach. Nurs Crit Care. 2007; 12: 225- 30.
4- Chang SS, Hsieh WH, Liu TS, Lee SH, Wang CH, Chou HC, et al. Mult iplex PCR syst em for rapid det ect ion of pat hogens in pat ient s wit h presum ed sepsis – a syst em at ic review and m et a-analysis. PLoS One. 2013; 8: e62323.
5- Cort elli JR, Aquino DR, Cort elli SC, Fernandes CB, Carvalho- Filho J, Franco GC, et al. Etiological analysis of initial colonization of periodontal pat hogens in oral cavity. J Clin Microbiol. 2008; 46: 1322- 9.
6- Cort elli JR, Cogo K, Aquino DR, Cort elli SC, Ricci- Nit t el D, Zhang 3HWDO9DOLGDWLRQRIWKHDQWLEDFWHUHPLFHI¿FDF\RIDQHVVHQWLDORLO rinse in a Brazilian populat ion: a cross- over st udy. Braz Oral Res. 2012; 26: 478- 84.
7- DuVall NB, Fisher TD, Hensley D, Hancock RH, Vandewalle KS. 7KHFRPSDUDWLYHHI¿FDF\RIFKORUKH[LGLQHDQGDPR[LFLOOLQWR reduce t he incidence and m agnit ude of bact eraem ia during t hird m olar ext ract ions: a prospect ive, blind, random ized clinical t rial. Oral Surg Oral Med Oral Pat hol Oral Radiol. 2013; 115: 752- 63.
8 - Fer es M, Figu eir edo LC, Fav er i M, St ew ar t B, Vizio W. Th e effectivenness of a preprocedural m outhrinse containing cetylpyridinium FKORULGHLQUHGXFLQJEDFWHULDLQWKHGHQWDORI¿FH-$P'HQW$VVRF 2010; 141: 415- 22.
9- Fine DH, Furgang D, McKierm an M, Tereski- Bischio D, Ricci- Nit t el D, Zhang P, et al. An invest igat ion of t he effect of an essent ial oil m out hrinse on induced bact erem ia: a pilot st udy. J Clin Periodont ol. 2010; 37: 840- 7.
10- Gm ür C, I rani S, At t in T, Menghini G, Schim idlin PR. Survey on oral hygiene m easures for int ubat ed pat ient s in Swiss int ensive care unit s. Schweiz Monat sschr Zahnm ed. 2013; 123: 394- 409.
11- Han YW, Wang X. Mobile m icrobiom e: oral bact eria in ext ra- oral LQIHFWLRQVDQGLQÀDPPDWLRQ-'HQW5HV
12- Hayashi C, Gudino CV, Gibson FC 3rd, Genco CA. Pat hogen- induced
LQÀDPPDWLRQDWVLWHVGLVWDQWIURPRUDOLQIHFWLRQEDFWHULDOSHUVLVWHQFH DQGLQGXFWLRQRIFHOOVSHFL¿FLQQDWHLPPXQHLQÀDPPDWRU\SDWKZD\V Mol Oral Microbiol. 2010; 25: 305- 16.
13- Hor liana AC, Cham br one L, Foz AM, Ar t ese HP, Rabelo MS, Pannut i CM, et al. Dissem inat ion of periodont al pat hogens in t he bloodst ream aft er periodont al procedures: a syst em at ic review. PLoS One. 2014; 9: e98271.
14- Kinane DF, Riggio MP, Walker KF, MacKenzie D, Shear er B. Bact eraem ia following periodont al procedures. J Clin Periodont ol. 2005; 32: 708- 13.
15- Kinane DF, Zhang P, Benakanakere M, Singlet on J, Biesbrock A, Nonnenm acher C, et al. Experim ent al gingivit is, bact erem ia and syst em ic biom arkers: a random ized clinical t rial. J Periodont al Res. 2015; 50( 6) : 864- 9.
16- Lockhart PB, Brennan MT, Thornhill M, Michalowicz BS, Noll J, Bahrani-Mougeot FK, et al. Poor oral hygiene as a risk factor for infective endocarditis-related bacterem ia. J Am Dent Assoc. 2009; 140: 1238-44. 17- Loe H, Silness J. Periodont al disease in pregnancy. I . Prevalence and severity. Act a Odont ol Scand. 1963; 21( 6) : 533- 51.
1 8 - Mah araj B, Coovadia Y, Vay ej AC. A com parat iv e st u dy of am oxicillin, clindam ycin and chorhexidine in t he prevent ion of post-ext ract ion bact eraem ia. Cardiovasc J Afr. 2012; 23( 9) : 491- 4. 19- Marín MJ, Figuero E, González I , O’Connor A, Diz P, Álvarez M, et al. Com parison of t he det ect ion of periodont al pat hogens in bact eraem ia aft er t oot h brushing by cult ure and m olecular t echniques. Med Oral Pat ol Oral Cir Bucal. 2016; 21: 276- 84.
20- Morozum i T, Kubot a T, Abe D, Shim izu T, Kom at su Y, Yoshie H. Effect s of irrigat ion wit h an ant isept ic and oral adm inist rat ion of azit hrom ycin on bact eraem ia caused by scaling and root planning. J Periodont ol. 2010; 81: 1555- 63.
21- Papapanou PN. Syst em ic effect s of periodont it is: lessons learned fr om r esear ch on at her oscler ot ic vascular disease and adv er se pregnancy out com es. I nt Dent J. 2015; 65: 283- 91.
2 2 - Pér ez- Ch ap ar r o PJ, Gr aci eu x P, Laf au r i e GI , D o n n i o PY, Bonnaure- Mallet M. Genot ypic charact erizat ion of Por phy r om onas
gin giv alis isolat ed fr om subgingival plaque and blood sam ple in
posit ive bact eraem ia subj ect s wit h periodont it is. J Clin Periodont ol. 2008; 35: 748- 53.
23- Ratto-Tespestini AC, Pérez- Chaparro PJ, Rom ito GA, Figueiredo LC, Faveri M, Carillo P, et al. Com parison of independent and dependent cult ure m et hods for t he det ect ion of t ransient bact erem ia in diabet ic subj ect s wit h chronic periodont it is. Biom edica. 2016; 36: 156- 61. 24- Sahrm ann P, Manz A, At t in T, Zbinden R, Schim idlin PR. Effect of applicat ion of a PVP- iodine solut ion before and during subgingival u lt r ason ic in st r u m en t at ion on p ost - t r eat m en t b act er aem ia: a random ized single- cent r e placebo- cont r olled clinical t r ial. J Clin Periodont ol. 2015; 42: 632- 9.
26- Szulc M, Kust rzycki W, Janczak D, Michalowska D, Baczynska D, Radwan- Oczko M. Presence of periodont opat hic bact eria DNA in at herom at ous plaques from coronary and carot id art eries. Biom ed Res I nt . 2015; 2015: 825397.
27- Tom ás I , Diz P, Tobías A, Scully C, Donos N. Periodont al healt h st at us and bact eraem ia from daily oral act ivit ies: syst em at ic review/ m et a-analysis. J Clin Periodont ol. 2012; 39: 213- 28.
28- Tuna A, Delilbasi C, Arslan A, Gurol Y, Tazequn Tekkanat Z. Do ant ibact erial m out hrinses affect bact eraem ia in t hird m olar surgery? A pilot st udy. Aust Dent J. 2012; 57: 435- 9.