w w w . r b o . o r g . b r
Original
Article
Clinical
and
functional
evaluation
of
forefoot
reconstruction
in
patients
with
rheumatoid
arthritis
夽
,
夽夽
Marco
Túlio
Costa
∗,
Ricardo
Cardoso
Backer,
Ricardo
Cardenuto
Ferreira
DepartmentofOrthopedicsandTraumatology,FernandinhoSimonsenWing,SchoolofMedicalSciences,SantaCasadeSãoPaulo,São Paulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23November2012 Accepted12July2013 Availableonline2April2014
Keywords:
Forefoot,human Rheumatoidarthritis Arthrodesis
a
b
s
t
r
a
c
t
Objective:toevaluatethelong-termresultsfromreconstructionoftheforefootinpatients withrheumatoidarthritiswhounderwentarthrodesisofthemetatarsophalangealjointof thehallux,resectionarthroplastyoftheheadsofthelateralmetatarsalsandcorrectionof thedeformitiesofthesmallertoesthrougharthrodesisoftheproximalinterphalangealjoint orclosedmanipulation.
Methods:seventeenpatients(27feet) whounderwent forefootreconstructionsurgeryby meansofarthrodesisofthefirstmetatarsophalangealjoint,resectionoftheheadsofthe lateralmetatarsalsandcorrectionofthedeformitiesofthesmallertoes,werestudied retro-spectively.Themeanfollow-upwas68months(12–148months);themeanagewas52years (range:20–75months);andfourpatientsweremaleand13werefemale.
Results:theresultswereclassifiedasexcellentin17feet,goodintwo,fairinfourandpoor intwo.ThemeanscoreontheAOFASscalewas70points;21feet(78%)werefoundtobe asymptomatic;andsixfeet(22%)presentedsometypeofsymptom.Threefeetpresented pseudarthrosis,andoneofthesesuccessfullyunderwentrevisionofthearthrodesis.There wasnosignificantdifferenceinscoringontheAOFASscaleorintheconsolidationrate, betweenusingaplateandscrewsandusingKirschnerwiresforfixationofthearthrodesis.
Conclusion: arthrodesisofthefirstmetatarsophalangealjointwithresectionarthroplastyon theheadsofthelateralmetatarsalsandcorrectionofthedeformitiesofthesmallertoes, whichwasusedinforefootreconstructioninrheumatoidpatients,showedgoodlong-term resultswithahighsatisfactionrateamongthepatientsandclinical-functional improve-ment.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽Pleasecitethisarticleas:CostaMT,BackerRC,FerreiraRC.Avaliac¸ãoclínico-funcionaldareconstruc¸ãodoantepénospacientes
portadoresdeartritereumatoide.RevBrasOrtop.2014;49:167–173.
夽夽
WorkperformedintheFootandAnkleGroup,DepartmentofOrthopedicsandTraumatology,FernandinhoSimonsenWing,Schoolof MedicalSciences,SantaCasadeSãoPaulo.
∗ Correspondingauthor.
E-mail:[email protected](M.T.Costa).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Avaliac¸ão
clínico-funcional
da
reconstruc¸ão
do
antepé
nos
pacientes
portadores
de
artrite
reumatoide
Palavras-chave:
Antepéhumano Artritereumatoide Artrodese
r
e
s
u
m
o
Objetivo: avaliarosresultadosemlongoprazodareconstruc¸ãodoantepénospacientes comartritereumatoidesubmetidosàartrodesedaarticulac¸ãometatarsofalângica(MTF)do hálux,artroplastiaderessecc¸ãodascabec¸asdosmetatarsoslateraisecorrec¸ãodas deformi-dadesnosdedosmenorespormeiodeartrodesedaarticulac¸ãointerfalângicaproximal(IFP) oumanipulac¸ãofechada.
Métodos:foramestudadosretrospectivamente17pacientes(27pés)submetidosàcirurgiade reconstruc¸ãodoantepécomartrodesedaprimeiraarticulac¸ãoMTF,ressecc¸ãodascabec¸as dosmetatarsoslateraisecorrec¸ãodasdeformidadesnosdedosmenores.Oseguimento médiofoide68meses(12a148),amédiadeidadefoide52anos(20a75meses)equatro pacienteseramdosexomasculinoe13dofeminino.
Resultados: osresultadosforamclassificadoscomoexcelenteem17pés,bomemdois, reg-ularemquatroeruimemdois.Apontuac¸ãomédiadaescalaAofas(AmericanOrthopaedic FootandAnkleSociety)foide70pontos,21pés(78%)encontravam-seassintomáticose seis(22%)apresentavamalgumtipodesintoma.Trêspésapresentarampseudoartrose.Um delesfoisubmetidoàrevisãodaartrodesecomsucesso.Nãohouvediferenc¸asignificativa napontuac¸ãodaescalaAofasenosíndicesdeconsolidac¸ãocomousodeplacaeparafusos oufiosdeKirschnernafixac¸ãodaartrodese.
Conclusão: a artrodese daprimeira articulac¸ão MTFcomartroplastia deressecc¸ão das cabec¸asdosmetatarsoslateraisecorrec¸ãodasdeformidadesnosdedosmenores,usada nareconstruc¸ãodoantepédospacientesreumatoides,demonstroubonsresultados em longoprazo,comelevadoíndicedesatisfac¸ãodospacientesemelhoriaclínico-funcional.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Rheumatoidarthritisisachronic andprogressivesystemic disease that presents incapacitating manifestations in the musculoskeletalsystemand may affectthe footand ankle in up to 90% of the cases. Half of them are located in the forefoot.1,2 The involvement of the forefoot is
char-acterized by chronic synovitis in the metatarsophalangeal (MTP)joints,capsulardistensionandlossofintegrityofthe collateral ligaments.3 Presenceofchronic capsule-ligament
instability, destruction ofthe joint cartilage and reabsorp-tion of the subchondral bone lead to typical deformities inthe forefoot.Hallux valgusis the commonestcondition in the first ray. The smaller toes typically present in rigid clawform,andwithsubluxationordislocationofthelateral MTPjoints.Progressionofthedeformitiesalsoleadsto dis-tal migrationof the plantarpad and favors appearance of metatarsalpain,ulcerationsandpainfulplantarcalluses,1–3
whichcausedifficultyinwalkingandinusingconventional footwear.
Surgical treatment is indicated when the conserva-tive measures fail to relieve the symptoms, and it has the main objectives of relieving the pain caused by syn-ovitis and joint destruction, correcting the deformities, improving the gait pattern and adapting the feet to shoes.1–3
Historically,avarietyofprocedureshavebeendescribedfor treatingrheumatoidforefeetandtheyhavetypicallyinvolved
correctionofdeformitiesoftheMTPjointofthesmallertoes bymeansofresectionarthroplastyofthemetatarsalheads orthebaseoftheproximalphalanx,orboth.Deformitiesin the smallertoescan becorrected bymeans ofresectionof thedistalportionoftheproximalphalanx,arthrodesisofthe proximal interphalangeal jointor closed manipulation and intramedullaryfixation.Theoptionsforcorrectionofhallux valgusincluderesectionarthroplastyofthemetatarsalhead ortheproximalphalanxofthehallux;jointreplacementusing metallicorsiliconeimplants;andarthrodesisoftheMTPofthe hallux.1–3
Withevolutionofthesurgicaltechniquesandbetter under-standingofthedeformities,arthrodesisoftheMTPjointofthe halluxhasbecomethetreatmentmethodmostusedfor cor-rectingdeformitiesofthefirstray.4–6Thisprocedurestabilizes
theMTPofthehalluxandallowsthistoreceivegreater pres-sureduringgait.Throughthis,actionbydeformingforceson theMTPjointsofthesmallertoesisprevented,therebyhelping towarddiminishingmetatarsalpainandpromotinglong-term resultsthataremoresatisfactory(painrelief,maintenanceof alignmentandpatientsatisfaction).5–9
Sample
and
methods
Seventeenpatients(27feet)withadiagnosisofrheumatoid arthritisandsevereforefootdeformitywereincludedinthis study.These patients underwent reconstructive surgery by meansofthetechniqueofarthrodesisofthefirstMTPjoint ofthehalluxandresectionarthroplastyoftheheadsofthe lateralmetatarsals,performedbytheFootandAnkleGroup ofSanta Casa de Misericórdia de São Paulo, between Jan-uary1998andMarch2010.All ofthesepatientshadsevere halluxvalgusdeformitiesassociatedwithpain,rigid deformi-tiesofthesmallertoesandmetatarsaltransferpainonthe headsofthelateralmetatarsals.Patientswhounderwent sur-gicalcorrectionbymeansofthetechniqueunderexamination butwhosepostoperativefollow-upwaslessthan12months wereexcluded.Themeanslengthoffollow-upwas68months (range:12–148).Fourpatientsweremaleand13werefemale. Themeanageatthetimeofthesurgerywas52years(range: 20–75years).
Severehalluxvalgusassociatedwithincapacitatingpain, rigiddeformitiesofthesmallertoesandmetatarsaltransfer ofpainontheheadsoflateralmetatarsalsledtothesurgical indication,whilepatientswhosepostoperativefollow-upwas lessthan12monthswereexcluded.
Thepatientswereevaluatedbymeansofpersonal inter-views and clinical examinations. They were asked about whether theyhad any painin theirforefeet; whether they wereabletouseconventionalclosedfootwear;andwhattheir degreeofsatisfactionwas,regardingthefinalresultsfromthe surgicalprocedure.Intheclinicalexamination,wenotedthe alignment,thepositionofthefootwhenbearingweightand thepresenceorabsenceofhalluxdeformities.Followingthis, withthepatientsittingontheexaminationtable,we investi-gatedthepresenceofmetatarsalpainandpainatthemedial eminenceofthehallux.Themedicalfileswerereviewedto establishthe preoperativecomplaints,location ofthe pain, severityofthedeformitiesandpresenceofearlyorlate post-operativecomplications.
Radiographicexaminationswereperformedin dorsoplan-tarandlateralviewsontheforefootwithload-bearing.The preoperative radiographs were recovered from the radio-graphicarchivesoftheMedicalandStatisticalFilingService (SAME)ofSantaCasadeMisericórdiadeSãoPaulo.Theimages wereevaluatedwithregardtopresenceorabsenceof consol-idationand thetypeoffixationusedforarthrodesisofthe MTPofthehallux.Thehalluxvalgusangle(HVA),10i.e.the
angleformedbetweenthelinesthatbisectthediaphysisof theproximalphalanxandthediaphysisofthefirstmetatarsal, andtheanglebetweenthefirstandsecondmetatarsals (inter-metatarsalangleI-II(IMAI-II),10i.e.theangleformedbetween
the linesthat bisect the diaphyses ofthe first and second metatarsals)weremeasured.
Wecompared the fixation method used for arthrodesis of the MTP of the hallux with the radiographic parame-ters obtainedfrom the final radiographsand observed the consolidationratesandangularcorrectionsobtained.We cor-relatedthefixationmethodwiththefunctionalclinicalresults accordingtotheAOFASscale11fortheMTPjointofthe
hal-lux.
TheAOFASfunctionalscale11 wasusedtoquantitatively
measure the postoperativeresults inorder toevaluate the MTPjointofthehallux.Thisscalerangesfrom0to100points andtakesinto considerationitemsrelatingtopain,activity level,deformityandmobility.Wedividedtheresultsintotwo groups:scoreslessthan70pointsandscoresgreaterthanor equalto70points.Wecomparedthesegroupsinrelationto ageatthetimeofthesurgery;initialdegreeofdeformity (eval-uatedbymeasuringtheHVAandIMAI-II);andthepresence orabsenceofconsolidationonthecurrentradiographs.
The resultswere also classified in accordance with the criteriadrawnup byMannandThompson,4 whoevaluated
thepresenceofpainintheforefootandthecapacitytouse closed footwear. The surgical result was considered to be excellentwhenthepatientsdidnotcomplainofpainwhen theywerestandinguprightandwerecapableofusing conven-tionalclosedfootwear;goodwhentheydidnotpresentpainful complaints,but wereonlyabletomakeuseofopenshoes; moderatewhentherewassomeresidualpainbut lessthan beforetheoperation;andpoorwhentherewasno improve-mentorevenworseningofthepain.
Patients’ satisfaction with the surgical procedure was assessedusingthescaleofJohnsonetal.12Itwasinvestigated
whethertheywerecompletelysatisfied,satisfiedwithslight reservations,satisfiedwithmajorreservationsordissatisfied.
Surgicaltechnique
ThefirstMTPjointwastreatedbymeans ofadorsal longi-tudinal incision of around5cm, centered on the joint and deepened over the medial edge of the long extensor ten-donofthehallux.Thecapsuleandthecollateral ligaments werereleased;thejointcartilageoftheproximalphalanxand metatarsalheadwereremoved;andmedialexostectomywas performed.Thearthrodesiswasfixedusingaplateandscrews, single screwsbetween fragments or two 2.0mm Kirschner wires.Kirschnerwireswereusedif,accordingtothesurgeon’s assessmentduring the operation,the bonequality didnot allowfixationofgreaterrigidity.Arthrodesiswasperformed inthepositionrecommendedintheliterature,withvalgusof around10◦,dorsiflexionof20◦andneutralrotation.1–6
TheMTPjointofthesmallerfingerswasexposedbymeans oftwodorsalincisionsofaround5cminthesecondandfourth intermetatarsal spaces.The collateral ligament,the dorsal portion of the capsule and intermetatarsal ligament were released circumferentiallyaroundthe baseofthe proximal phalanxandthemetatarsalheadandneck.Themetatarsal headswereresectedinthedistalofthemetaphysiswiththe aidofasaw,startingwiththesecondmetatarsaland progres-sivelyrepeatingthisfortheotherlateralmetatarsals,taking caretomaintainthemetatarsalformula.
After the operation, all the patients used sandals with weight-bearingontheforefoot,andloadingwasallowedas tolerated. The dressing was changed every weekuntil the stitcheswereremoved,15–20daysafterthe operation.The patientcontinuedtousethesandalsuntiltherewere radio-graphic indications of consolidation of the arthrodesis of theMTP ofthehallux (between10 and12 weeksafterthe operation),whenthesandalswerewithdrawnanduseof com-fortable footwear was allowed. TheKirschner wires ofthe smallertoes were removed asoutpatientprocedures,eight weeksaftertheoperation.TheKirschnerwiresofthe MTP ofthehallux wereremoved onlyafterconsolidationofthe arthrodesis.
Results
Allthepatientswereevaluatedbythesameexaminer,who didnotparticipateinthetreatment.ThemeanAOFASscore fortheMTPjointofthehalluxobtainedinthefinal evalua-tionwas70pointsoutofapossible90points(range:25–88).It wasconsideredthatthemaximumAOFASscorefortheMTP ofthehalluxwas90pointsbecauseofthelossofjointmobility inthefirstMTPafterarthrodesis,whichimpededtheuseof thisparameterasameansofevaluatingpostoperative func-tion.WhenthepainparameteroftheAOFASscorefortheMTP ofthehalluxwasevaluatedseparately,themeanvaluewas observedtobe34outofthe40pointspossible(range:20–40). Weobservedtwocases(twofeet)withdeepinfectioninthe operativewoundinthedorsumofthefootandskinnecrosisat thesiteofthearthrodesisoftheMTPofthehallux.Thesecases occurredinpatientswhoweresmokers,andbothunderwent serialdebridementand intravenousantibiotictherapyuntil theinfectiousconditionhadbeenresolved.Therewasalsoone case(onefoot)withsuperficialinfection,whichwasresolved bymeansoforalantibiotictherapyandserialdressings.One footpresentedvascularcomplicationsduringtheimmediate postoperativeperiodandevolvedwithnecrosisand amputa-tionofthethirdtoe.
We observed the presence of pseudarthrosis in three feet,aslatecomplications.Oneofthemunderwentrevision surgery,withsubsequentconsolidation.Theother twofeet inwhichconsolidationofthearthrodesisoftheMTPofthe halluxwasnotachievedoccurredinpatientswhopresented deepinfectionofthe operativewoundand skinnecrosisas earlycomplications.Oneofthesecasesevolvedwithchronic osteomyelitis.Thesynthesis materialand devitalized bone wereremoved,andprolongedintravenousantibiotictherapy wasadministered,whichledtoresolutionoftheinfectious condition.However,thispatientcontinuedtopresentpainful symptomsinthefirstMTPjointandtherewasrecurrenceof thevalgusdeformityofthehallux.Intheothercase,complete resolutionoftheinfectiousconditionwasachievedthrough debridementandantibiotictherapy,althoughpseudarthrosis wasseentobepresentlaterinthepostoperativefollow-up. Both ofthe casesthat presenteddeep infection and pseu-darthrosisoccurredinpatientswhosmoked.
Inthemostrecentclinicalexamination,14patients(21feet) (78%)didnothaveanycomplaints.Sixpatients(6feet)(22%) presentedsometypeofsymptom.Threepatients(3/27feet;
Table1–Meanangularcorrectionamongthepatients withrheumatoidarthritiswhounderwent
reconstructionoftheforefootbymeansofarthrodesisof themetatarsophalangealjointofthehallux.
Pre-op(mean) Post-opfinal
(mean)
Angular correction
(mean)
HVA 41◦ 17◦ 24◦
IMAI-II 15◦ 11◦ 4◦
HVA,halluxvalgusangle;IMAI-II,intermetatarsalanglebetween thefirstandsecondmetatarsals.
11%)wereobservedtopresentplantarmetatarsalpainalone; twopatients(2/27;7%)presentedpainanddeformityinthe halluxalone.Oneofthesewasoneofthecasesthatevolved withpseudarthrosis.Theotherpatient(onefoot), who pre-senteddeepinfectionandpseudarthrosisoftheMTPofthe hallux,evolvedwithpainanddeformityinthehalluxin asso-ciationwithmetatarsalpainandwasasmoker.
UsingthecriteriaofMannandThompson,4theresultswere
classifiedasexcellentin19feet(71%),goodintwo(7%), moder-ateinfour(15%)andpoorintwo(7%).Regardingthepatients’ satisfactionwiththesurgicalprocedureaccordingtothescale ofJohnsonetal.,1210patients(15feet)werefoundtobe
com-pletelysatisfiedwiththeresultsfromthesurgery,five(10feet) weresatisfiedwithslightreservationsandtwo(twofeet)were dissatisfied.
Theangularcorrectionobtainedinthepatientswho under-wentforefootreconstructionisdemonstratedinTable1,along withthepre-andpostoperativemeanvaluesfortheHVAand IMAI-II.
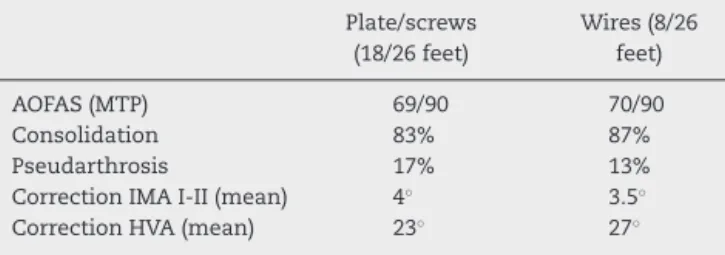
Weevaluatedthefixationmethodusedinarthrodesisof theMTPofthehalluxandcorrelatedtheradiographic param-eters with the clinical-functional results according to the AOFASscale,asdemonstratedinTable2.Wedidnotfindany significantdifferencesinAOFASscoresoncomparingthe fix-ationofthearthrodesisontheMTPofthehalluxusingaplate andscrewsversusKirschnerwires.Likewise,wedidnotfind anydifferencesinconsolidationratesbetweenthesetwo fixa-tionmethods.Themeanangularcorrectionswerealsosimilar. Theclinical-functionalresultsexpressedusingtheAOFAS scaleweredividedintotwogroups:scoreslowerthan70points
Table2–Comparisonbetweenthetypesoffixationin relationtotheclinicalandradiographicparametersof patientswithrheumatoidarthritiswhounderwent forefootreconstruction.
Plate/screws (18/26feet)
Wires(8/26 feet)
AOFAS(MTP) 69/90 70/90
Consolidation 83% 87%
Pseudarthrosis 17% 13%
CorrectionIMAI-II(mean) 4◦ 3.5◦
CorrectionHVA(mean) 23◦ 27◦
Table3–Distributionofthefeetoperatedaccordingto theAOFAScriteriaandcomparisonwiththeclinicaland radiographicparametersofpatientswithrheumatoid arthritiswhounderwentforefootreconstruction.
AOFAS<70 points(10/27
feet)
AOFAS≥70
points(17/27 feet)
Meanageinyears 63 46
Consolidationof
arthrodesisoftheMTPof thehallux
70% 100%
InitialIMAI-II(mean) 15◦ 15◦
InitialHVA(mean) 29◦ 48◦
MTP, metatarsophalangealjoint; IMA I-II,intermetatarsal angle betweenthefirstandsecondmetatarsals;HVA,halluxvalgusangle.
andscoregreaterthanorequalto70points,asdemonstrated inTable 3. We observed differences between thesegroups regardingthemeanage atthe timeofthe surgeryandthe consolidationratesassessedfromthefinalradiographs.The meanagewas46yearsinthegroupwithAOFASscoresgreater thanor equalto70points, whilethe meanageamongthe feetwithscoresless than70 pointswas63 years.Thefeet withhigherAOFASscoresalsoachieved100%consolidation, whereasthegroupwithscoreslessthan70pointsachieved 70%consolidationinthefinalradiographicevaluation.
Discussion
Manysurgicalprocedureshavebeendescribedfortreating hal-luxvalgusanddeformitiesofthesmallertoesinpatientswith rheumatoidarthritis.In1912,Hoffman13describedresection
ofallofthemetatarsalheadsbymeansofasingleplantar inci-sion.Otherauthors14–16modifiedtheoperativetechniqueover
timeanddemonstrateddifferentresultsaccordingtothetype ofincision(dorsalorplantar),14,15repositioningoftheplantar
padorexcisionofthemetatarsalheadsorproximalphalanx ofthetoes.14,15
Initially,treatmentofthefirstraycontinuedtobethemost controversialpointinforefootreconstructioninrheumatoid patients.14 Overtime,resectionofthebaseoftheproximal
phalanx(Kellerprocedure)15andresectionoftheheadofthe
first metatarsal (Mayo procedure)17 became popular. These
procedureshavedemonstratedhighrecurrenceratesfor hal-luxvalgus,metatarsalpainandplantarcalluses.15,18
Henryand Waugh7 and Mann and Thompson4
demon-stratedthatstablerealignmentofthefirstrayisadetermining factorforobtainingbetterresultsfromreconstructingthe fore-footinthesepatients,giventhatarthrodesisoftheMTPofthe halluxincreasestheplantarpressureonthemedialcolumn ofthefootduringgaitandpreventstheactionofdeforming forcesontheMTPjointsofthesmallertoes,therebyhelping todiminishmetatarsalpain.
Throughthis,arthrodesisofthe MTPjointofthehallux hasbecomethetreatmentmethodmostusedforcorrecting deformitiesofthehalluxandhasledtobetterresultsinterms ofpainrelief,functionalimprovement,maintenanceof align-mentandpatientsatisfaction.6,8,9
Inourstudy,wefoundamongthe27feetevaluatedthat71% oftheresultswereexcellentand7%weregood,withamean follow-upof68months,accordingtothecriteriadeveloped by Mann and Thompson.4 This demonstrates the
clinical-functionalimprovementandpatients’satisfactionwiththis typeofprocedure.MannandThompson4foundthat78%of
their resultswere excellent among18 feet thatunderwent arthrodesis ofthe MTP ofthe hallux and resection of the metatarsalheads,withameanfollow-upof49months.Using thesameassessmentcriteria,butwithresectionarthroplasty oftheheadsofallthemetatarsals,ratherthanarthrodesisof theMTPjointofthehallux,Thomasetal.19foundthatonly
30%oftheirresultsweregoodorexcellentinevaluating37 feetwithameanfollow-upof65months.
Mostofthestudieshaveevaluatedtheclinical-functional resultsfromforefootreconstructionsurgerybymeansofthe AOFASscalefortheMTPjointofthehallux.Coughlin6founda
meanAOFASscoreof69pointsamong47feetthatthey evalu-ated;Kadambandeetal.8studied66feetandreportedamean
AOFASscoreof65points;andHeitkemperetal.9obtainedthe
bestresults:ameanscoreof81pointsamong20feetthatwere evaluatedwithameanfollow-upof42months.
Theseauthors’observationswereconfirmedinourstudy. WefoundameanAOFASscoreof70pointsfortheMTPjoint ofthehallux,withameanfollow-upof68months.The fac-torthat contributed towardthegreatest lossofpointswas themobilityoftheMTPjointofthehallux,since arthrode-sisimpedesthe movementofthisjoint.Thistookaway 10 pointsfromtheAOFASscore,thuspreventingthemaximum score from exceeding90 points. Presenceofsome residual painintheforefoot,whichwasobservedinsixofthe27feet, andincapacitytouseconventionalclosedshoeseveninthe absenceofpainfulsymptoms,asobservedintwoofthe27feet, tookawaypointsregardingtheissuesofpainandfunction. Theseareexpectedconditionsamongpatientswith rheuma-toidarthritis,becauseofthechronicandprogressivenatureof thedisease,whichimpedescompleteeliminationofthe symp-toms,evenwhenusingacarefulvalidatedsurgicaltechnique.3
AlthougharthrodesisoftheMTPofthehalluxhasgained popularity overrecent years and hasbecomethe standard procedureforreconstructingrheumatoidforefeet,few stud-ieshavequantifiedtheradiographicalignmentofthefirstray. MannandThompson4observedameancorrectionof23◦for
thehalluxvalgusangle,whiletheintermetatarsal angleI-II presentedameancorrectionof4◦.Coughlin6 alsoobserved
similarvaluesinhisseriesof47feet,withameancorrection of18◦forthehalluxvalgusangleand3◦fortheintermetatarsal
angle I-II.Kadambandeet al.8 studied 66feet and founda
mean correctionof23◦ forthe hallux valgusangle and 8◦
fortheintermetatarsalangleI-II.Wefoundresultssimilarto thoseintheliteratureinthepresentstudy.Inourseries,the halluxvalgusanglewascorrectedbyameanof24◦,whilethe
intermetatarsalangleI-IIwascorrectedby4◦.
Other studies havealreadycorrelated arthrodesisofthe MTPofthehalluxwithcorrectionoftheintermetatarsalangle I-II20–22andhaveobservedameancorrectionof3◦to8◦inthis
Thedifferentfixationmethodsusedforarthrodesisofthe firstMTPjointwere alsoevaluatedandcomparedwiththe clinical-functionalandradiographicresults.Weobservedthat, independentofwhetherfixationhadbeendoneusingaplate andscrewsorwithKirschnerwires,theclinicalresultswere similar according tothe AOFAS scorefor the MTP joint of thehallux.Likewise,the consolidationratesandthe mean angularcorrectiondidnotdemonstrateanysignificant differ-encesbetweenthe groups.However,biomechanicalstudies havedemonstratedthesuperiorityoffixationusingcrossed screwsbetweenfragmentsorassociationsofplateandscrews withothermethods.Neufeld etal.23 comparedthree
stabi-lization methods for arthrodesisof the MTP of the hallux incadaversanddemonstratedthattheassemblypresented greaterrigiditywhencrossedscrewswereused.Politietal.24
comparedfivetypesoffixationinbiomechanicaltrialsusing syntheticboneanddemonstratedthatfixationwithaplate inassociationwithtwoscrewsbetweenfragmentswasmore stablethan fixation with the plate alone, and that assem-blieswith twocrossed Kirschnerwires presentedthe least rigidity.Althoughtheuseofaplateandscrewshas demon-stratedgreaterrigidityandstabilityinbiomechanicalstudies, wedidnotfindany clinicalstudiescomparingthe consoli-dationratesandclinical-functionalresultsbetweendifferent fixation methods.Moreover, it is known that factors relat-ingtothepatientmayalsoinfluencetheclinical-functional result. Appropriate collaboration during the postoperative period and care to avoid smoking and other risk factors arefundamentalforachievingconsolidationinanygroupof patients.25
Incomparingtheclinical-functionalresultsaccordingto the AOFAS score for the MTP joint of the hallux with the radiographicresults,we observedthatthe consolidationof the arthrodesis influenced the results. The patients who presentedpseudarthrosisatthe finalevaluationhadworse resultsaccordingtotheAOFASscore.
Ageatthetimeofthesurgeryalsoinfluencedthe clinical-functionalresultaccordingtotheAOFASscoreforthe MTP jointofthehallux,sincethepatientsincludedinthegroup withAOFASscoresgreater thanor equalto70 presenteda mean age of46 years,whereas the group with scoresless than 70 had a mean age of63 years.Thesmaller number ofmusculoskeletalabnormalitiesandlowerinitialsystemic involvementofthe disease in the youngerpatients proba-bly explain these findings,given that rheumatoid arthritis isachronicand progressivediseaseand thatthedegreeof osteoarticularinvolvementincreaseswiththedurationofthe disease.3
Surgical treatment forpatients with rheumatoid arthri-tis is a challenge for orthopedic surgeons because of the potentialriskofpostoperativecomplications.3Thesepatients
presenthigherriskofcomplicationsbecauseofthesystemic nature of the disease, use of immunosuppressant medi-cations and severity of their deformities.26 Typically, they
presentsignificantosteopenia,whichbooststheriskof fail-ure of bone fixation during surgical interventions, as well asfrequently presenting associatedvasculitis, which leads tofragilityofthesubcutaneoustissueandcompromisesthe healing of surgical wounds.3 The percentage of
complica-tionsobservedinourserieswascompatiblewithwhathas
been presentedinthe literature. Thepersistence or recur-rence ofmetatarsal pain that was observed infour of the 27 feet (15%) was concordant with the percentage found in other studies, which has ranged from 10% to 36%.5,7–9
This may be minimized through meticuloussurgical tech-nique: correct positioning is attained for the arthrodesis of the MTP of the hallux and all the fragments or bone spiculesareremovedduringresectionofthelateralmetatarsal heads. However, thechronic and progressivenature ofthe disease prevents this complication from being completely eliminated.3
PseudarthrosisfromarthrodesisoftheMTPofthehalluxis alsoanexpectedcomplicationamongthesepatients.3Inthe
literature,theseratesmayrangefrom0to26%,4–6,8,27whichis
compatiblewiththerateof11%(3/27feet)foundinthepresent study.Acarefulsurgicaltechniqueinpreparingthe arthrode-sisanduseofreliablefixationmethodswithgreaterrigidity andstabilitycontributetowarddiminishingtheseratesand increasingthepercentageconsolidation.
The great majority of these patients also use powerful immunosuppressant drugs, which theoretically boosts the risk ofinfection and problems with the healing of opera-tive wounds.3 In a reviewarticle, Nassar and Cracchiolo26
demonstrated that the rate of problems with the healing of operative woundsin patients with rheumatoid arthritis who undergosurgicalproceduresintheforefootmayrange from 0% to 11%, and also that superficial or deep infec-tion ofthe operativewoundmayoccur in0%to8%ofthe cases. In the present study, we found that 8% (2/27 feet) hadproblemswithwoundhealing,whichwascharacterized bydeep skinnecrosisand delayedhealingoftheoperative wound.Wealsofoundinfectionin12%(twofeetwithdeep infection and one with superficial infection). These num-bers were concordant with those publishedby Nassar and Cracchiolo26anddemonstratedthatthepotentialriskof
com-plicationswasinherenttosurgicaltreatmentamongpatients withrheumatoidarthritis,becauseofthesystemicnatureof thedisease,thechronicuseofimmunosuppressantsandthe severityofthedeformities,whichadddifficultytothesurgical procedures.26
Although wefound the expectedcomplication ratesfor forefootreconstructionsurgeryinpatientswithrheumatoid arthritis, and these rates were concordant with what was found in the previous literature;4–8,26,27 we observed that
smokingwasadeterminingfactorforcomplicationstoappear inourstudy,despitethesmallnumberofcases.Theharmful effectsofcigarettesonorthopedicsurgeryhavealreadybeen widelystudiedandproven.28Thus,ithasbeendemonstrated
thatsmoking increasestheriskofpseudarthrosis,29
dimin-ishesbonedensity,30 causesproblemsrelatingtohealingof
operative wounds and increases the risk ofinfection.31 In
Conclusions
ThetechniqueofarthrodesisofthefirstMTPjointin associ-ationwithresectionarthroplastyoftheheadsofthelateral metatarsalsandcorrectionofthedeformitiesofthesmaller toes,whichwasusedtoreconstructthesevereforefoot defor-mitiesofthesepatients withrheumatoid arthritis,showed goodlong-termresultswithahigh satisfactionrateamong thepatientsandclinical-functionalimprovementaccording totheAOFASscale fortheMTPjoint ofthehallux andthe evaluationcriteriaproposedbyMann.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. JaakkolaJI,MannRA.Areviewofrheumatoidarthritis affectingthefootandankle.FootAnkleInt.
2004;25(12):866–74.
2. JengC,CampbellJ.Currentconceptsreview:therheumatoid forefoot.FootAnkleInt.2008;29(9):959–68.
3. TriebK.Managementofthefootinrheumatoidarthritis.J BoneJointSurgBr.2005;87(9):1171–7.
4. MannRA,ThompsonFM.Arthrodesisofthefirst
metatarsophalangealjointforhalluxvalgusinrheumatoid arthritis.JBoneJointSurgAm.1984;66(5):687–92.
5. MannRA,SchakelIIME.Surgicalcorrectionofrheumatoid forefootdeformities.FootAnkleInt.1995;16(1):1–6.
6. CoughlinMJ.Rheumatoidforefootreconstruction.A long-termfollow-upstudy.JBoneJointSurgAm. 2000;82(3):322–41.
7. HenryAP,WaughW,WoodH.Theuseoffootprintsin assessingtheresultsofoperationsforhalluxvalgus.A comparisonofKeller’soperationandarthrodesis.JBoneJoint SurgBr.1975;57(4):478–81.
8. KadambandeS,DebnathU,KhuranaA,HemmadyM, HariharanK.Rheumatoidforefootreconstruction:1st metatarsophalangealfusionandexcisionarthroplastyof lessermetatarsalheads.ActaOrthopBelg.2007;73(1):88–95.
9. HeitkemperS,PingsmanA,QuitmannA,PatsalisT. Correctionofrheumaticforefoot.Thevalueofacombined arthrodesisofthefirsttoeandresectionofmetatarsalheads 2-5.Orthopade.2007;36(5):478–83.
10.CoughlinMJ.Halluxvalgus.JBoneJointSurgAm. 1996;78(6):932–66.
11.KitaokaHB,AlexanderIJ,AdelaarRS,NunleyJA,MyersonMS, SandersM.Clinicalratingsystemsfortheankle-hindfoot, midfoot,hallux,andlessertoes.FootAnkleInt.
1994;15(7):349–53.
12.FornellC,JohnsonM,AndersonE,ChaJ,BryantB.The AmericanCustomerSatisfactionIndex:nature,purpose,and findings.JMarketing.1996;60(1):7–18.
13.HoffmannP.Anoperationforseveregradesofcontractedor clawedtoes1911.ClinOrthopRelatRes.1997;(340):4–6.
14.BartonNJ.Arthroplastyoftheforefootinrheumatoid arthritis.JBoneJointSurgBr.1973;55(1):126–33.
15.VahvanenV,PiirainenH,KettunenP.Resectionarthroplasty ofthemetatarsophalangealjointsinrheumatoidarthritis.A follow-upstudyof100patients.ScandJRheumatol. 1980;9(4):257–65.
16.PatsalisT,GeorgousisH,GöpfertS.Long-termresultsof forefootarthroplastyinpatientswithrheumatoidarthritis. Orthopedics.1996;19(5):439–47.
17.ClaytonML,LeidholtJD,ClarkW.Arthroplastyofrheumatoid metatarsophalangealjoints:anoutcomestudy.ClinOrthop RelatRes.1997;(340):48–57.
18.GoldieI,BremellT,AlthoffB,IrstamL.Metatarsalhead resectioninthetreatmentoftherheumatoidforefoot.ScandJ Rheumatol.1983;12(2):106–12.
19.ThomasS,KinninmonthAW,KumarCS.Long-termresultsof themodifiedHoffmanprocedureintherheumatoidforefoot.J BoneJointSurgAm.2005;87(4):748–52.
20.CroninJJ,LimbersJP,KuttyS,StephensMM.Intermetatarsal angleafterfirstmetatarsophalangealjointarthrodesisfor halluxvalgus.FootAnkleInt.2006;27(2):104–9.
21.PydahSK,TohEM,SirikondaSP,WalkerCR.Intermetatarsal angularchangefollowingfusionofthefirst
metatarsophalangealjoint.FootAnkleInt.2009;30(5):415–8.
22.CostaMT,LopesNetoDL,KojimaFH,FerreiraRC.Avaliac¸ão doângulointermetatarsalapósaartrodesedaprimeira articulac¸ãometatarsofalangeanaparatratamentodohálux valgo.RevBrasOrtop.2012;47(3):363–7.
23.NeufeldSK,ParksBG,NaseefGS,MelamedEA,SchonLC. Arthrodesisofthefirstmetatarsophalangealjoint:a biomechanicalstudycomparingmemorycompression staples,cannulatedscrews,andadorsalplate.FootAnkleInt. 2002;23(2):97–101.
24.PolitiJ,JohnH,NjusG,BennettGL,KayDB.First
metatarsal-phalangealjointarthrodesis:abiomechanical assessmentofstability.FootAnkleInt.2003;24(4):332–7.
25.BennettGL,SabettaJ.Firstmetatarsalphalangealjoint arthrodesis:evaluationofplateandscrewfixation.FootAnkle Int.2009;30(8):752–7.
26.NassarJ,CracchioloIIIA.Complicationsinsurgeryofthefoot andankleinpatientswithrheumatoidarthritis.ClinOrthop RelatRes.2001;(391):140–52.
27.GrondalL,HedstromM,StarkA.Arthrodesiscomparedto Mayoresectionofthefirstmetatarsophalangealjointintotal rheumatoidforefootreconstruction.FootAnkleInt.
2005;26(2):135–9.
28.MollerAM,PedersenT,VillebroN,MunksgaardA.Effectof smokingonearlycomplicationsafterelectiveorthopaedic surgery.JBoneJointSurgBr.2003;85(2):178–81.
29.CastilloRC,BosseMJ,MacKenzieEJ,PattersonBM,LEAPStudy Group.Impactofsmokingonfracturehealingandriskof complicationsinlimb-threateningopentibiafractures.J OrthopTrauma.2005;19(3):151–7.
30.LawMR,HackshawAK.Ameta-analysisofcigarettesmoking, bonemineraldensityandriskofhipfracture:recognitionofa majoreffect.BMJ.1997;315(7112):841–6,4.