REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
transforaminal
and
interlaminar
epidural
steroid
injections
for
the
treatment
of
chronic
lumbar
pain
Serbülent
Gökhan
Beyaz
SakaryaUniversityFacultyofMedicine,DepartmentofAnesthesiologyandPainMedicine,Sakarya,Turkey
Received21May2015;accepted22June2015 Availableonline19March2016
KEYWORDS
Transforaminal; Interlaminar; Lowbackpain; Spinalinjection; Complication
Abstract
Studydesign:Across-sectionalstudy.
Objective: We compared the 12 month outcomesof fluoroscopically guided transforaminal
epiduralsteroidinjectionswithinterlaminarepiduralsteroidinjectionsforthetreatmentof chroniclumbarspinalpain.Chroniclowerbackpainisamultifactorialdisorderwithmany pos-sibleetiologies.Thelifetimeprevalenceofspinalpainisreportedly65---80%intheneckand lowerback.Epiduralinjectionofcorticosteroidsisacommonlyusedinterventionformanaging chronicspinalpain.
Methods:Patientswhodidnotbenefitfromprevioustreatmentswereincludedinthisstudy.
Injectionswere performedaccordingtomagneticresonanceimagingfindings atthenearest leveloflumbarpathology;173patientsreceivedinterlaminarepiduralsteroidinjectionsand126 patientsreceivedtransforaminalepiduralsteroidinjections.Allofthepatientswereregularly followed upfor12 monthsusing averbalnumericratingscale. Magneticresonanceimaging findings,complications,verbalnumericratingscale,andsatisfactionscoreswererecorded.
Results:Lumbardiskpathologywasthemostfrequentlyencounteredproblem.The
interlami-narepiduralsteroidinjectionswerepreferredattheL4---L5intervertebrallevel.Verbalnumeric ratingscalescoressignificantlydecreasedduringthe12-monthperiodcomparedtobasalscores (p<0.001).Significantdifferencesbetweenthetwogroupsaccordingtoverbalnumericrating scaleandsatisfactionscoreswerenotobserved(p>0.05).Therewerenomajorcomplications; however,theinterlaminarepiduralsteroidinjectionsgrouphad22(12.7%)minorcomplications, andthetransforaminalepiduralsteroidinjectionsgrouphad12(9.5%)minorcomplications.
Conclusions: Thisstudyshowedthatinterlaminarepiduralsteroidinjectionscanbeaseffective
astransforaminalepiduralsteroidinjectionswhenperformedatthenearestleveloflumbar pathologyusingfluoroscopyin12-monthintervals.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
E-mail:[email protected]
http://dx.doi.org/10.1016/j.bjane.2015.06.003
PALAVRAS-CHAVE
Transforaminal; Interlaminar; Dorlombar; Injec¸ãoespinhal; Complicac¸ão
Comparac¸ãodastécnicastransforaminaleinterlaminardeinjec¸õesepiduraisde esteroidesparaotratamentodedorlombarcrônica
Resumo
Desenhodoestudo:Estudotransversal.
Objetivo:Comparamososdesfechosde12mesesdeinjec¸õesperiduraisdeesteroidesusandoa
técnicatransforaminal(IPETF)guiadaporfluoroscopiacomasinjec¸õesperiduraisdeesteroides usandoatécnicainterlaminar(IPEIL)paraotratamentodadorlombarcrônica.Adorlombar crônicaéumadoenc¸amultifatorialcommuitasetiologiaspossíveis.Relata-sequeaprevalência dedornacolunaduranteavidaéde65%-80%nopescoc¸oeparteinferiordascostas.Ainjec¸ão periduraldecorticosteroideséumaintervenc¸ãocomumenteusadaparacontrolaradorcrônica dacolunavertebral.
Métodos: Pacientesquenão obtiveram benefíciodetratamentosanteriores foramincluídos
nesteestudo.Asinjec¸õesforamrealizadasdeacordocomosachadosemRessonânciaMagnética (RM)aonívelmaispróximodapatologialombar;173pacientesreceberamIPEILe126pacientes receberamIPETF.Todosospacientesforamacompanhadosregularmentepor12meses,usando umaescalanuméricaverbal(ENV)paraaclassificac¸ão.AchadosemRM,complicac¸ões,escores ENVeíndicesdesatisfac¸ãoforamregistrados.
Resultados: Patologiaemdiscolombarfoioproblemamaisfrequentementeencontrado.IPEIL
foipreferidoaonívelintervertebraldeL4-L5.OsescoresdaENVdiminuíramsignificativamente duranteoperíodode12 mesesemcomparac¸ãocomosvaloresbasais(p<0,001).Nãohouve diferenc¸assignificativasentreosdoisgruposdeacordocomaENVeosíndicesdesatisfac¸ão (p>0,05).Nãohouvegrandescomplicac¸ões,mashouvecomplicac¸õesmenoresem22(12,7%) nogrupoIPEILe12(9,5%)nogrupoIPETF.
Conclusões:EsteestudomostrouqueIPEILpodesertãoeficazcomoIPETFquandorealizadas
aonívelmaispróximodapatologialombarusandoafluoroscopiaemintervalosde12meses. ©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Lowerbackpainwithorwithoutlowerlimbpainisthemost commonproblemamongacuteandchronicpaindisorders, andhassignificantimplications.1---3Chroniclowerbackpain
isamultifactorialdisorderwithmanypossibleetiologies.4,5
Thelifetimeprevalenceofspinalpainisreportedly65---80% intheneckandlowerback.6Kuslichetal.7identified
inter-vertebraldiscs,facetjoints,ligaments,fascia,muscles,and nerverootduraasthetissuescapableoftransmittingpain inthelowerback.
Intervertebral disk herniation, spinal stenosis, inter-vertebral disk degeneration without disk herniation, degenerativespondylolisthesiswithstenosis,andpost lum-barsurgerysyndromearethemost commondiagnosesfor lowerbackandlegsymptoms.1
Disk-related pain is caused by disk degeneration, disk herniation,orbiochemicaleffectsincludinginflammation. Degeneration of thehuman intervertebral diskis a major clinicalproblemandtheleadingcauseofpainanddisability, resultinginsignificanthealthcare-relatedcosts.The degen-erativeprocessin intervertebraldiscsis associatedwitha seriesofbiochemicalandmorphologicalchangesthat com-bine toalter the biomechanical properties of the motion segment.Diskdegenerationwithorwithoutdiskherniation canleadtolowerbackpain.8
Generally, the etiology of lumbar spinal pain includes not only mechanical neural compression, but also vascu-larcompromise,inflammation,andbiochemicalandneural mechanisms.Neurotoxicityhasalsobeenattributedtomany agentsincludingphospholipaseA2andtumornecrosisfactor, whichmayplayessentialrolesinintervertebraldisk-induced nerverootdamage.9,10
Epidural injection of corticosteroids is one of the most commonly used interventions for managing chronic spinalpain.1---5,11,12However,clinicaldataregardingepidural
steroidapplicationsinTurkeywerenotavailable.Currently, epiduralinjectionsarefrequentlyperformedinterventions in the United States, and over 1 million epidural steroid injectionsareperformedannuallyworldwide.1,2,11
Oftheseveralapproachesavailabletoaccessthelumbar epiduralspace, thelumbar interlaminarapproachis com-monlyused,followedbylumbartransforaminalandcaudal epiduralsteroidinjections.3,6 Increasingemphasis isbeing
placedonfluoroscopicallyguided,target-specificinjections toimprove treatmentoutcomes; therefore,modern study designs focus on fluoroscopically guided transforaminal injectiontechniques,whichhavethetheoreticaladvantage ofdeliveringtheinjectatetothesiteofthepathologyinthe anteriorepiduralspace.13
injections(TFESI),bothfluoroscopicallyguided,overa 12-monthperiodoftreatmentforchroniclumbarspinalpain.
Methods
This a cross-sectional study was approved by the Faculty of Medicine’s Ethics Committee of Sakarya University (no 2012/45); 364patients, treatedby epiduralsteroid injec-tions for chronic lumbar pain, were evaluated. All of the studypatientswereinformedregardinginterventions, and writteninformedconsentwasobtained.
Thecriteriaforthestudyincludedaminimumof6months lowerbackpain,unilateralorbilaterallegpainsymptoms, andnopositiveresponsestomedicalorphysicaltherapies. Medical therapies included non steroidal anti inflamma-tory drugs, andin somecases, opioids. Physicaltherapies includedinitialbedrestandpassivephysiotherapy,followed byanextension-basedexerciseprogramandlight,and iso-metriccorestrengtheningifpainwasnotrelievedafter 2 weeksofmedicaltherapies.Patientlumbarspinal patholo-gies were clinically examined. An experienced radiologist confirmedthepathologiesusingmagneticresonanceimaging (MRI).Exclusioncriteriaforthestudyincludedpatientswho refusedinterventions,didnotreceivelumbarsurgery,were pregnant,hadanycontraindicationstointerventions (coag-ulopathy,sepsis,or allergytodrugsor contrastmaterial), received lumbar spinal interventions in other clinics, had previouslyundergonelumbarsurgery,andhadneurological deficitsorcaudaequinasyndrome.
All of the patients were examined, and imaging stud-ies were reviewed prior to injection by the author. The choice ofwhether touse thetransforaminal or the inter-laminarapproachwasdeterminedbythefirstauthorinno predeterminedorder.TFESIwasperformed ifpatientshad radicularpainandpositiveMRIfindingsat oneortwo lev-els.Similarly,ILESIwasperformedifpatientshadradicular pain,lowerbackpain,andMRIfindingsatoneortwolevels. Atthetimeoftheprocedures,theauthorhadnopersonal preferenceforeitherapproach.
Alloftheinjectionswereperformedinasimilarmanner. Routinehemograms,biochemical,andcoagulation parame-ters wereevaluatedtoconfirm thattheywere withinthe normalrange,afterwhich thepatients weretakentothe operatingroom.Alloftheinjectionswereperformedbyone anesthesiologist,and6---8hoffastingwaspreferredonthe injectionday. Alloftheprocedureswereperformedunder C-arm fluoroscopic guidance. Initial anteroposterior (AP) imageswereobtainedtoidentifythelevelandinterlaminar spacein a pronepositionwitha10cmhigh pillow placed under the abdomen. On the fluoroscopic table, standard anesthesia monitoring (noninvasive blood pressure, pulse oxymeter,ECG)wasperformed,and0.9%NaClwasstarted intravenously.Theinjectionareawascleanedwithan anti-septiciodine-basedsolution,andanesthetizedwith0.5mL 2%prilocaineinjectedintotheskinandsubcutaneoustissue; 1---2mgmidazolamand25---50gfentanylwereadministered forconscioussedation.
FortheTLESIapproach,a20gaugebluntcurvedneedle (Epimed®,Johnstown,NY,USA)wasused.Thetargetpoint
wasaccessedbythesubpedicularsafetriangle14,15approach
in theobliqueposition. Inall ofthe TLESIapplications, a
mixtureof80mgtriamcinoloneacetonidein0.25% bupiva-caine was used.After placing the needle into the target point, 0.5---2mL nonionic contrast material (Iomeron 300, Patheon,ItaliaS.p.A.)wasinjectedtodeterminewhether vascularleakageorintrathecaldistributionoccurred.After theaccurate anteriorepidural flow pattern wasobserved onoblique,anteroposterior,andlateralimages,4mLofthe mixturewas injected if TLESIwas performed for asingle level.IfTLESIwasperformedformorethanonelevel,2mL ofthe mixtureper each levelwasinjected, but thetotal steroiddosewasmaintainedconstant;forexample,atotal of8mLof80mgtriamcinoloneacetonidein0.25% bupiva-cainemixturewasadministeredforalllevels.Inthecaseof vascularleakage,theneedlesitewasslightlyrepositioned andrecontrolled bycontrastmaterial. Ifvascular leakage persisted,theprocedurewascanceledforthatlevel.Ifthe interventionwas performed for morethan one level, the erroneousinjectionoftheresidualmixtureintothe subse-quentlevelwasavoidedbyflushingtheneedlewithsterile isotonicaftereachlevel.
FortheILESIapproach,an18gauge,3½-in.or5in.Tuohy needlewasadvanceddirectly perpendiculartotheskin in a posterior toanterior direction, with use of the loss-of-resistancetoairtechniquetoidentifytheepiduralspace.In caseswhen traditionalmethods failedtoreachthe epidu-ral space,the parasagittalapproach waspreferred.After negativeaspirationforcerebrospinalfluidandblood,2mL nonioniccontrast material wasinjected todocument the appropriatecontrastspreadintotheepiduralspace.Next, acombinationof8mLof80mgtriamcinoloneacetonidewith 3mL0.25%bupivacainewasinjectedintheepiduralspace. Aftertheintervention,thepatientsrestedonthetable for5min,andwerethentransportedtotherecoveryroom where they stayed 2h if complications did not develop. Thecomplicationsthatoccurredduringtheprocedurewere recorded.The patientswereaskedtosit,stand,andwalk before rating their pain using the Verbal Numerical Rat-ingScale(VNRS,0-10scale).Allofthedataobtainedwere recordedonthe patient’scharts. The patients discharged fromthe hospitalwereasked toimmediatelyrefertoour painclinicifanunexpectedsituationoccurred.Onthe con-troldays(1,3,6,9,and12monthsafterinjection),patients wereinterviewedatthehospital,andprobabletherapeutic effects,VNRS,andcomplicationswererecorded.Moreover, age,gender,andMRIfindingswererecordedonthepatient’s charts for post-interventional evaluations. ModifiedNorth
Table 1 Modified North American Spine Society Patient SatisfactoryScore.
Score
Bad Nochangeofcomplaints;evenworse. Moderate EpiduralsteroidhelpedmebutIwon’tlet
thisprocedureagain.
Good MostofthecomplaintsarerelievedandI wouldagainletthisprocedureifmy complaintsreappear.
AmericanSpineSociety(NASS)patientsatisfactionscorewas recordedusinga4pointscale(Table1).
Statisticalanalysis
Alldata were analyzed usingthe statistical package SPSS version 15.0 for Windows. Kolmogorov---Smirnov test was usedtodetermineifthedemographicdataweredistributed normally.Chi-Squaretestwasusedtocomparethe satisfac-tionscoresandcomplicationsbetweenthegroups.Repeated measurements ANOVA parametric test for repeated mea-surementsanalysiswasusedtoevaluatetheimprovements inVNRSscoresbeforeandaftertheprocedure.Independent samplet-testanalysiswasperformedfordifferencesinpain reductionbetweenthetwogroups.Datawerepresentedas means±standarddeviation(SD).
Results
Inthe present study,364 patientswere enrolledbetween April 2013 and October 2014 for epidural injections. Of these,23patientsdidnotcometothehospital,1refused interventionontheoperationtable,6couldnotbereached by telephone, and 36 had a previous history of lumbar surgery. The number of patients with complete data was 299. The distribution of these patients according to the month was 299 (100%), 238 (79.6%), 211 (70.6%), 171 (57.2%),and114(38.1%),respectively.
A total of 299 patients received 485 interventions. The patients were divided into two groups according to the steroid injection approach used. The transforaminal approachgroup(theTFESIgroup)consistedof126patients with266 injectionsincludingrepeatedinjections,andthe interlaminarapproachgroup(theILESIgroup)consistedof 173patients with219 injectionsincludingrepeated injec-tions.Theaverageagewas54.66(11.69)years(range23---85 years).Demographicdatarevealednosignificantdifferences betweenthegroups(Table2).
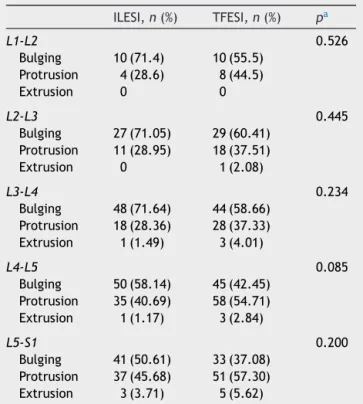
WhenMRIimageswereevaluated,numerouspathologies were detected, such as disk herniation, spinal degen-eration, spondilolisthesis, facet hypertrophy, and spinal stenosis.Diskpathologiesweredividedinto4types;namely, bulging, protrusion, extrudation, and sequestration. The most affected level was L4---L5 (Table 3). Bulging was the most common pathology, and no sequestration was
Table2 Demographicfeaturesofgroups.
ILESI(n=173) TFESI(n=126) pa
Years 58.08(13.49) 51.45(12.50) 0.001 GenderM/F 50/123 41/85 0.623 Weight 69.38(10.25) 66.48(11.84) 0.527 Height 161(8.7) 164(11.6) 0.376 Numberof
injections
173 219 0.001
Painduration, years
2.2 1.9 0.172
ILESI, interlaminar epidural steroid injections; TFESI, trans-foraminalepiduralsteroidinjections.
aChi-squaretest.
Table3 TheMRIfindingsof299patientstheLESI.
ILESI,n(%) TFESI,n(%) pa
L1-L2 0.526
Bulging 10(71.4) 10(55.5) Protrusion 4(28.6) 8(44.5) Extrusion 0 0
L2-L3 0.445
Bulging 27(71.05) 29(60.41) Protrusion 11(28.95) 18(37.51) Extrusion 0 1(2.08)
L3-L4 0.234
Bulging 48(71.64) 44(58.66) Protrusion 18(28.36) 28(37.33) Extrusion 1(1.49) 3(4.01)
L4-L5 0.085
Bulging 50(58.14) 45(42.45) Protrusion 35(40.69) 58(54.71) Extrusion 1(1.17) 3(2.84)
L5-S1 0.200
Bulging 41(50.61) 33(37.08) Protrusion 37(45.68) 51(57.30) Extrusion 3(3.71) 5(5.62)
Dataarepresentedasn(%).LESI,lumbarepiduralsteroid injec-tion.
a Chi-squaretest.
detected;144patientshadonlydiskpathologies.Inaddition todiskpathologies,64patientshaddegenerativechanges, 125 patients had diffuse degeneration, 73 patients had spinalstenosesofvarioustypes,and27patientshadfacet jointhypertrophy.
L4---L5 was the most injected level in both groups (Table4).Theaveragepre-injectionVNRSscoreintheILESI group was7.8 (1.9)and intheTFESI group was7.6(2.2). Thepost-injectionVNRSscoresinbothgroupsat1,3,6,9, and12monthsalsodecreased(p<0.001,Fig.1).Although theVNRSscoresgraduallyincreasedafterthefirstmonth, nosignificantdifferencecouldbedetected.TheVNRSand satisfactionscoreswerenotsignificantlydifferentbetween thegroups(p>0.05forbothscores).
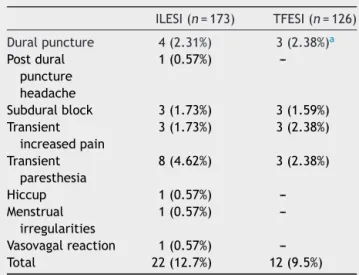
Nocatastrophic complications wereobserved in either the ILESI or TFESI group. The ILESI group had 22 (12.7%) minor complications, and the TFESI group had 12 (9.5%) minorcomplications (Table5). Duringthetherapy period,
12
10
*
* * * *
8
6
VNRS 4
2
0
0 1 3
Month
6 9 12
ILESI TFESI
Table4 Repeatedinjectionsforlumbarepiduralsteroidinjections.
Singleinjection Firstrepeated injections
Secondrepeated injections
Totalinjections
TFESI
Onelevel 26/26 16/32 --- 42/58
Twolevel 70/140 11/44 4/24 85/208
ILESI
Onelevel 130/130 40/80 3/9 173/219
Dataarepresentedaspatientnumber/injectionnumber.
ILESI,interlaminarepiduralsteroidinjections;TFESI,transforaminalepiduralsteroidinjections.
Table5 DistributionofcomplicationsforILESIandTFESI.
ILESI(n=173) TFESI(n=126)
Duralpuncture 4(2.31%) 3(2.38%)a
Postdural puncture headache
1(0.57%)
---Subduralblock 3(1.73%) 3(1.59%) Transient
increasedpain
3(1.73%) 3(2.38%)
Transient paresthesia
8(4.62%) 3(2.38%)
Hiccup 1(0.57%) ---Menstrual
irregularities
1(0.57%)
---Vasovagalreaction 1(0.57%) ---Total 22(12.7%) 12(9.5%)
ILESI, interlaminar lumbar epidural steroid injection; TFESI, transforaminalepiduralsteroidinjection.
Dataaregivenn(%).
a Thecontrastagentwereintrathecalspreadinthreepatients
whoduralpuncture.
threepatientsintheILESIgroup(1.73%)andeightpatients intheTFESIgroup(6.35%)underwentlumbarsurgery.
Discussion
This study was conducted to evaluate and compare
the effects of two different lumbar steroid injection approaches.Thelengthofthestudyperiodwas12months, and the study population included chronic lumbar pain patients.
Pre-procedural analysis of patient information did not show any significant difference in symptom duration betweenthetwogroups.TheaverageageintheILESIgroup wassignificantlyhigherthanthat intheTFESI group. Pre-intervention VNRS scores in the ILESI group were higher thanthoseintheTFESIgroup,althoughwithoutstatistical significance. In terms of comparableparameters, the MRI findings were not significantly different between the two groups(Table3).
Atthe12monthfollow-up,theVNRSscoressignificantly decreasedafterepiduralsteroidinjectionsinbothgroups. Thisdecreasewasreflectedclinicallyasincreased satisfac-tion scores. Most of the patients (85.1%) improved after
injection,andexpressedimprovedwell-being.However,the symptomsworsenedin13.9%ofthepatientswhoratedtheir conditionasbad.
Inanotherrecentstudy,interlaminarinjectionprovided superiorpainreliefinupto92%ofpatients,whereas trans-foraminal injection provided pain relief in up to 90.5% of patients; however, in 9.5% of patients the condition worsened after TFESI, indicating that both steroid injec-tions largely provided pain relief.16 The decreased VNRS
scores in the TFESI group were not significantly differ-ent from the ILESI group. High satisfaction scores could beexplainedbytheinjectatematerialbeingadministered close to the pathology sites. Conversely, the ILESI group consistedofolderpatientswithmulti-levelpathologiesand morecomplexconditions,whichmighthavecontributedto thedifferences.
Thecurrentstudyisimportantbecausebothgroupshad similarly high satisfactionscores (85.1%), which might be duetoeffective fluoroscopyorinjectionsiteproximity.In 2002,Wangetal.17 conductedastudyon69patientswith
symptomatic lumbar diskhernia. On follow-ups after the epiduralsteroidinjections,radicularpainwasdecreasedfor 20---27months,andsurgicalinterventionwasavoidedduring thisperiod.
In 2007, Acherman et al.18 conducted a study on 90
patients comparing the transforaminal, interlaminar, and caudal approaches, and concluded that the transforami-nalapproachwasthemosteffective.However,theresults weresimilarinallthreegroups(TFESI,ILESI,caudal epidu-ral steroid injection groups). Each group consisted of 30 patients;13patientsintheTFESIgroupand12intheILESI group were not satisfied and only 1 patient experienced improvement.ThepathologysitelevelinILESIwasthesame forallpatients,whichmighthavecausedthedifferences.
Inthecurrentstudy,therewerenosignificantdifferences betweenTFESIandILESIlevelsasshownintheTable5.
In 2006, Schaufele et al.13 conducted a study on 20
patientscomparingthetwoapproachesofepiduralsteroid injections, and concluded the TFESI was more effective. However,significant limitationsexisted in theirstudy;the populationnumberwasverysmall(n=20),andtheageof patientswasunknown. The similaritytothis studyis that theyinjectedthesteroidatthesameleveloflumbar pathol-ogy.In2004,Butterman19comparedsurgerywithILESIusing
painfor6weeksbeforesurgery.In1995,areviewbyKoes et al.20 examined eight randomized trials that evaluated
the effectiveness of ILESI on disk herniation, sciatica, or radiculopathyinthelumbarspine.Oftheeightrandomized trialsevaluating lumbar radiculitis, five were positive for short-termrelief,whereasonlyonestudywaspositivefor long-termrelief.In2003,Boswelletal.4 conducteda
sys-tematicreviewofILESIpatients,andshowedanabsenceof long-termside-effects.
These results are supported by two randomized con-trolled studies,21,22,5 but Karppinen et al.21 reported less
positive outcomes. Thus, numerous studies on TFESI and ILESIhavebeenpublished,whichindicatepositiveor neg-ative results with over 6 months of efficacy. Recently, TFESIprovidedmoreefficientresults,butILESIstudieswere conductedas randomizedcontrolled studies usinga blind techniqueforsinglelevelinjections.InanILESIstudyusing theblindtechnique,thesuccessratewas70%,meaningthat 30%23ofthepatientswerenotsatisfied.Howeverinthe
cur-rent study,fluoroscopy wasused in both TFESI andILESI. Inaddition,ILESIwasperformed attheclosest sitetothe pathology.Our resultsshowed thatTFESI hadmuchlower scoresthanILESI,becausethepatientswereolderandtheir pathologiesweremulti-leveled.
Hopwood and Abram24 described 33 factors associated
withthesuccessrateoflumbarepiduralsteroidinjections, andsuggested thatall factors shouldbeconsidered when treatingchroniclumbarpainpatientswithepiduralsteroids. However,theexperienceofthepersonperformingthe pro-cedureremainsaveryimportantfactorthatinfluencesthe success/satisfactionrate.2
InareviewbyParretal.1evaluatingdiskherniationand
radiculitis, none of the randomized ILESI trialswere per-formedunderfluoroscopy.Amongvariousreviews,epidural steroidinjectionswerenotperformedunderfluoroscopyin anyof thepublished,randomizedcontrolledstudies.1,3,4,20
Recently,authorstendedtopreferTFESIunderfluoroscopy, becausethedrugwasdirectly administeredtotheprecise pathologysitelevel.
Fewer complications were encountered in the TFESI groupthantheILESIgroup(9.5%and12.7%,respectively), andmajorcomplicationsrequiringhospitalizationwerenot observed.When performingTFESI,theduralmaybe punc-tureddespiteappropriateneedleplacement.Subduraland intrathecalspreadofcontrastisrarelyobservedwith trans-foraminalinjections,andthuscanbeeasilyoverlooked.In theTFESIgroup,sixpatientshadduralpunctureduringan intervention,but none of thepatients had complainedof headaches.However, in theILESI group, only one patient had dural puncture, and was treated with an epidural bloodpatch.Accidentalduralpuncturesmayleadtospinal headaches.15 A particularly concerning complication of a
duralpunctureistheinstillationofanestheticintothe sub-duralspace,whichmayleadtoasubduralneuralblockade. Priorreportshavesuggestedanincidenceof0.82%for sub-dural injections during interlaminar epidural injections.25
To recognize a potential dural puncture, interventionists need to distinguish the intrathecal, subdural, and epidu-ralcontrastflowpatterns.Goodmanetal.26reporteddural
puncturecomplicationsduringtheTFESI,particularlyduring thesubduralinjection,whichisprobablyunder-reportedby practitioners.
Thestrengthofthisstudywasthatthesameperson per-formedalloftheinterventionsunderfluoroscopyguidance, and the study population waslarge. However,limitations including selection bias, recall bias,and incomplete data sets existed. Patients were not randomized for inclusion in this study, because group heterogeneity was the most importantlimitationinthisstudy.Assessingglobaland back-specificfunctioninadditiontoVNRSscoreswouldbeabetter methodforqualifying anydifferencesinclinicaloutcomes betweenILESIandTFESI.
Advanced age may cause increased multiple-level pathologies that aggravatelumbar spinal pain.After a 12 monthfollow-up,weconcludedthatILESIcanbeaseffective asTFESIifperformedunderfluoroscopyattheclosestlevel tothelumbarpathology.Nevertheless,furtherrandomized studiescomparingthetwoapproachesperformedunder flu-oroscopyattheclosestleveltothelumbarpathologiesare necessary.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
Acknowledgments
Alloftheauthorscriticallyrevisedthemanuscriptfor impor-tantintellectualcontentandapprovedthefinalmanuscript. Thisstudyhadnosponsorandnoexternalfunding.
References
1.ParrAT,DiwanS,AbdiS.Lumbarinterlaminarepidural injec-tionsinmanagingchroniclowbackandlowerextremitypain:a systematicreview.PainPhysician.2009;12:163---88.
2.Beyaz SG.Interlaminar lumbar epidural steroidinjections in degenerativelumbarspinalstenosispatients.JClinAnalMed. 2014;5:234---8.
3.Furman MB, Kothari G, Parikh T, et al. Efficacy of fluoro-scopically guided, contrast-enhanced lumbosacral interlam-inar epidural steroid injections: a pilot study. Pain Med. 2010;11:1328---34.
4.BoswellMV,HansenHC,TrescotAM,etal.Epiduralsteroidsin themanagementofchronicspinalpainandradiculopathy.Pain Physician.2003;6:319---34.
5.ManchikantiL,BoswellMV,DattaS,etal.Comprehensivereview oftherapeutic interventionsinmanagingchronicspinal pain. PainPhysician.2009;12:E123---98.
6.BogdukN.Epiduralsteroidsforlowbackpainandsciatica.Pain Digest.1999;9:226---7.
7.KuslichSD,UlstromCL,MichaelCJ.Thetissueoriginoflowback painandsciatica:areportofpainresponsetotissuestimulation duringoperationsonthelumbarspineusinglocalanesthesia. OrthopClinNorthAm.1991;22:181---7.
8.Wheeler AH, MurreyDB. Chroniclumbarspine and radicular pain:pathophysiologyandtreatment.CurrPainHeadacheRep. 2002;6:97---105.
9.Olmarker K, Nordborg C, Larsson K, et al. Ultrastructural changesinspinal nerveroots inducedbyautologousnucleus pulposus.Spine(PhilaPa1976).1996;21:411---4.
11.ManchikantiL.Thegrowthofinterventionalpainmanagement inthenewmillennium:acriticalanalysisofutilizationinthe medicarepopulation.PainPhysician.2004;7:465---82.
12.ErginA. Epiduralsteroid injectionsand lowbackpain. Agri. 2005;17:23---7.
13.Schaufele MK, Hatch L, Jones W. Interlaminar versus transforaminalepiduralinjectionsforthetreatmentof symp-tomaticlumbarintervertebraldischerniations.PainPhysician. 2006;9:361---6.
14.KaramanH,Kavak GO,Tüfek A, etal. Thecomplications of transforaminallumbarepiduralsteroidinjections.Spine(Phila Pa1976).2011;36:E819---24.
15.GoodmanBS,PosecionLW,MallempatiS,etal.Complications andpitfallsoflumbarinterlaminarandtransforaminalepidural injections.CurrRevMusculoskeletMed.2008;1:212---22. 16.NawaniDP,AgrawalS,AsthanaV.Singleshotepiduralinjection
for cervical and lumbosaccral radiculopathies: a preliminary study.KoreanJPain.2010;23:254---7.
17.WangJC,LinE,BrodkeDS,etal. Epiduralinjectionsfor the treatmentofsymptomaticlumbarherniateddiscs.JSpinal Dis-ordTech.2002;15:269---72.
18.AckermanWE 3rd,Ahmad M. The efficacyof lumbar epidu-ralsteroidinjectionsinpatientswithlumbardischerniations. AnesthAnalg.2007;104:1217---22.
19.ButtermannGR. Treatmentoflumbardischerniation: epidu-ralsteroidinjectioncomparedwithdiscectomy.Aprospective, randomizedstudy.JBoneJointSurgAm.2004;86-A:670---9. 20.Koes BW, Scholten RJ, Mens JM, et al. Efficacy of epidural
steroid injections for low-back pain and sciatica: a sys-tematic review of randomizedclinical trials. Pain. 1995;63: 279---88.
21.KarppinenJ,MalmivaaraA,KurunlahtiM,etal.Periradicular infiltration for sciatica: a randomizedcontrolled trial.Spine (PhilaPa1976).2001;26:1059---67.
22.VadVB,BhatAL,LutzGE,etal.Transforaminalepiduralsteroid injectionsinlumbosacralradiculopathy:aprospective random-izedstudy.Spine(PhilaPa1976).2002;27:11---6.
23.WhiteAH,DerbyR,WynneG.Epiduralinjectionsforthe diag-nosisand treatmentoflow-backpain. Spine(PhilaPa1976). 1980;5:78---86.
24.HopwoodMB,AbramSE.Factorsassociatedwithfailureof lum-barepiduralsteroids.RegAnesth.1993;18:238---43.
25.Lehmann LJ,PallaresVS. Subduralinjectionofa local anes-theticwithsteroids:complicationofepiduralanesthesia.South MedJ.1995;88:467---9.