Dent ist ry Division of t he Cent ral Inst it ut e and Experiment al Neurosurgery Division of t he Psychiat ric Inst it ut e, Hospit al das Clínicas, School of M edicine, Universit y of São Paulo, São Paulo SP, Brazil (HC/FM USP): 1DDS, PhD, Head, Orof acial Pain Team, Dent ist ry Division,
HC- FM USP; 2DDS, M sC, Orof acial Pain Team, Dent ist ry Division, HC/FM USP; 3DDS, Orof acial Pain Team, Dent ist ry Division, HC/FM USP; 4DDS, Post -graduat ion St udent , Orof acial Pain Team, Dent ist ry Division ,HC/FM USP; 5M D, PhD, Head, Pain M ult idisciplinary Cent er,
Neurology Division, and Experimental Neurosurgery Division, Psychiatric Institute, HC/FMUSP; 6DM D, Prof essor of Universit y of Dentistry
and M edicine of New Jersey/USA; 7DDS, M D, PhD, Pharmacology Prof essor, Universit y of Sant o Amaro (UNISA), São Paulo SP, Brazil. *The preliminary result s of t his st udy w ere present ed at 8t h World Congress on Pain, in Vancouver/Canada, August 1996.
Received 15 January 2004, received in f inal f orm 23 June 2004, Accept ed 9 August 2004.
Dr. José Tadeu Tesseroli de Siqueira - Rua M aria Cândida 135 - 02071010 São Paulo SP - Brasil. E-mail: jt t [email protected]
CLINICAL STUDY OF PATIENTS WITH
PERSISTENT OROFACIAL PAIN
José Tadeu Tesseroli de Siqueira
1, Lin Hui Ching
2,
Cibele Nasri
3, Silvia Regina Dow gan Tesseroli de Siqueira
4,
M anoel JacobsenTeixeira
5, Gary Heir
6, Luís Biela S. Valle
7ABSTRACT - Objetive: To evaluate a sample of patients with persistent facial pain unresponsive to prior treat-ment s. M et hods: Hospit al records of 26 pat ient s w it h persist ent f acial pain w ere review ed (20 f emale and
6 male). Result s: Pat ient s w ere classif ied int o t hree groups according t o t heir present ing sympt oms:
a)Group I, eight patients (30.7%) with severe, diffuse pain at the face, teeth or head; b)Group II, eight patients (30.7%) with chronic non-myofascial pain and; c)Group III, ten patients with chronic myofascial pain (38.4%). We f ind 11 diff erent diagnoses among t he 26 pat ient s: pulpit is(7), leukemia(1), oropharyngeal t umor(1), at ypical odont algia(1), Eagle’s syndrome(1), t rigeminal neuralgia(4), cont inuous neuralgia(1), t emporomandibular disorders (9), f ibromyalgia (2), t ensiont ype headache(1), conversion hyst eria(2). Af t er t he t reat -ment program all pat ient s had a six-mont h f ollow -up period w it h pain relief , except t he pat ient w it h t umor.
Conclusion: The w ide variabilit y of orof acial pain diagnosis (benign t o lif e-t hreat ening diseases) indicat es
t he necessit y t o reevaluat e pat ient s present ing recurrent pain t hat is ref ract ory t o t he usual t reat ment s.
KEY WORDS: orof acial pain, t rigeminal neuralgia, t umor, t emporomandibular disorders, at ypical f acial pain
Est udo clínico de pacient es com dor orof acial persist ent e
RESUM O - Objet ivo: Avaliar uma amost ra de doent es com dor f acial persist ent e. M ét odo: Foram
revisa-dos 26 prontuários de doentes com dor facial persistente (20 mulheres e 6 homens). Resultados: Classificação
dos doent es, após o diagnóst ico: a)Grupo I, oit o pacient es (30,7% ) com dor f acial dif usa de f ort íssima int en-sidade; b)Grupo II, oit o pacient es (30,7% ) com dor crônica de nat ureza não-miof ascial e; c)Grupo III, dez pacient es com dor crônica miof ascial (38,4% ). Foram encont rados 11 diagnóst icos dif erent es ent re os 26 pacient es: pulpit es(7), leucemia(1), t umor de orof aringe(1), odont algia at ípica(1), síndrome de Eagle(1), neuralgia idiopát ica do t rigêmeo(4), neuralgia at ípica(1), disordens t emporomandibular (9), f ibromialgia(2) cef aléia t ipo-t ensão(1), hist eria de conversão(2). O acompanhament o dos doent es, após receberem a respect iva t erapia, f oi de seis meses, com alívio da dor, excet o para o doent e com t umor de orof aringe.
Conclusão: A variabilidade das f ont es da dor f acial inclui doenças benignas e doenças graves, sendo
indis-pensável a reavaliaçâo de doent es que não respondem aos t rat ament os convencionais para a dor.
PALAVRAS-CHAVE: dor orof acial, neuralgia t rigeminal, t umor, art iculação t emporomandibular, dor f acial at ípica.
The complex innervat ion and f unct ion of f acial st ruct ures makes t he diagnosis of f acial pain and it s t reat ment very dif f icult and f rust rat ing1,2.
Pa-t ienPa-t s w iPa-t h chronic f acial pain, even af Pa-t er receiv-ing mult iple t reat ment s, should be caref ully reas-sessed and clinically re-examined. M yof ascial pain syndromes, t emporo mandibular disorders (TM D), neuralgias, ENT diseases, dent al pain, t umors,
neu-rovascular pain or psychiat ric diseases f requent ly present w it h overlapping signs and sympt oms3,4.
Ref erred, severe, acut e pain f requent ly makes t he diagnosis dif f icult .
secondary adjacent muscle hyperact ivit y. Pat ient s can present w it h muscular hyperact ivit y result ing f rom persist ent acut e or chronic pain, and elicit sec-ondary muscle pain7-9. Theref ore, t he eliminat ion
of t he primary source of pain is essent ial but , in chronic pain, is not alw ays enough f or cont rol of pain. An incorrect and inef f ect ive t reat ment may perpet uat e or generat e chronic pain. The under-st anding of secondary pain mechanisms of cran-iof acial pain is necessary f or t he f ormulat ion of an accurat e diagnosis10.
The goal of t his st udy is t o demonst rat e t he vari-abilit y of possible diagnoses in a sample of pat ient s w it h persist ent f acial pain and how t he orof acial pain specialt y t eam w as able t o assist in t heir diag-nosis and management .
M ETHOD
This is a ret rospect ive st udy of a sample of pat ient s w it h persist ent f acial pain unresponsive t o previous t reat ment s w ho w ere ref erred t o an orof acial pain t eam
of a large t eaching hospit al. The st udy w as approved by t he Et hics Commission of t he hospit al.
The records of 26 consecut ive pat ient s, 20 f emale and 6 male, w ere analyzed. Pat ient s w ere select ed accord-ing t o t he descript ion of t heir chronic pain sympt oms and classif ied in accordance w it h t he crit eria of t he In-t ernaIn-t ional AssociaIn-t ion f or In-t he SIn-t udy of Pain11and ref
-erences of t he American Academy of Orof acial Pain12.
This sample represent s 4% of all new pat ient s w it h oro-f acial pain complaint s admit t ed t o t he Orooro-f acial Pain Clinic during t he period of t his st udy (August 1992 -December 1996). In order t o ensure consist ency in int er-view met hods, t he diagnoses w ere conf irmed by clini-cal examinat ion perf ormed by members of a t rained and calibrat ed int erdisciplinary pain t eam.
The st andardized diagnost ic prot ocol w as applied t o all pat ient s equally. It consist s of a st andardized int er-view and syst emat ic evaluat ion of cervical, cranial, f acial, oral and dent al st ruct ures. The general charact erist ics f or dif f erent ial diagnosis of t he diseases are present ed in Table 1. Diagnoses w ere:
Pulpitis – History of daily, throbbing, diffuse pain,
trig-ger by hot or cold and w aking t he pat ient during t he
Table 1. Dif f erent ial diagnosis in pain f requent ly observed in t he orof acial region1,2,7,12,14.
Idiopat hic Pulpit is Orof acial Temporo Fibromyalgia Eagle’s
t rigeminal (ref erred neoplasia mandibular syndrome
neuralgia dent al pain) disorders
Pain Elet ric Trobbing Variable Dull, st abbing Dull Dull
shock-like (at ypical)
Pain durat ion Seconds M inut es Variable M inut e t o hours Const ant Short
-t o hours durat ion
Int ensit y Severe Slight t o severe Severe M oderat e M oderat e M iddle Localizat ion Good Dif f use Dif f use Good, Dif f use Dif f use Dif f use Charact erist ics Trigger zone, Diurnal or Ref erred pain TM J or muscle, Generalized Usually pain
diurnal noct urnal f requent ly pain t o body pain, is in t he
dent al neurological movement , spont aneous t hroat / sensit ivit y, look signs, WBC limit ed open mout h f loor f or dent al abnormalit ies mout h
problem
Local t reat ment No Dent al Surgical Physical therapy, Physical Cort icoid
t reat ment s, splint s, t herapy inject ion,
local anesthesia anest het ic surgery
blocks t he pain inject ion,
General Ant i- NSAIDs, Chemot herapy, NSAIDs TAD, NSAIDs
t reat ment convulsivant s analgesics radiot herapy myorelaxant s HSCT
Trigger Non-noxious M echanical, Jaw movement Palpat ion, jaw Palpat ion, Sw alling
st imulus f oods, cold, f unct ion f unct ion
heat , suit
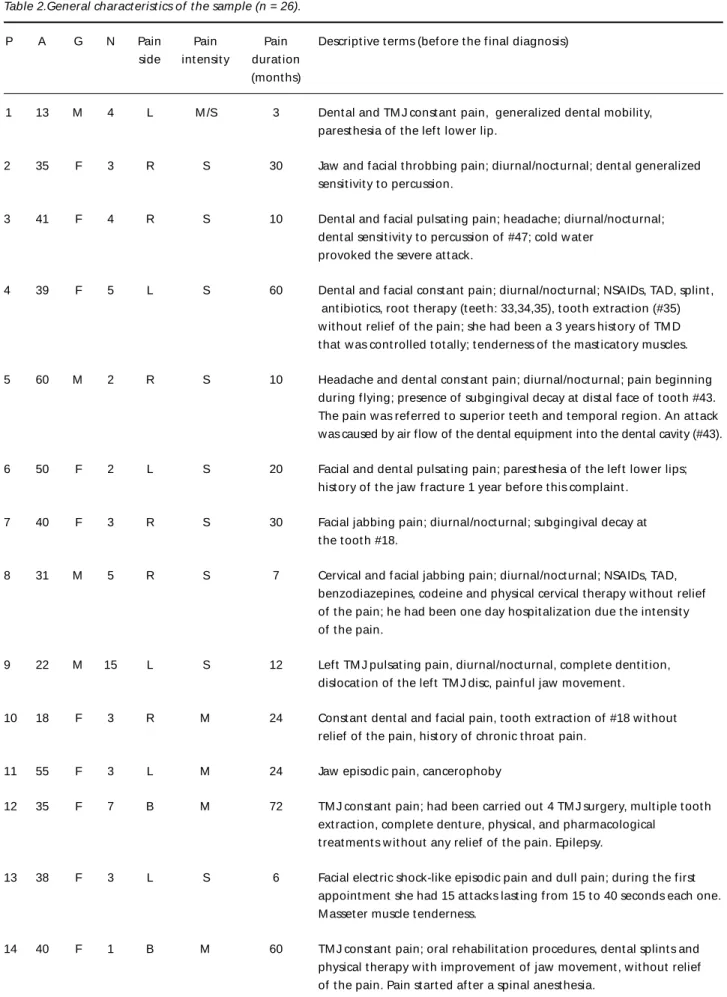
Table 2.General charact erist ics of t he sample (n = 26).
P A G N Pain Pain Pain Descript ive t erms (bef ore t he f inal diagnosis) side int ensit y durat ion
(mont hs)
1 13 M 4 L M /S 3 Dent al and TM J const ant pain, generalized dent al mobilit y, parest hesia of t he lef t low er lip.
2 35 F 3 R S 30 Jaw and f acial t hrobbing pain; diurnal/noct urnal; dent al generalized sensit ivit y t o percussion.
3 41 F 4 R S 10 Dent al and f acial pulsat ing pain; headache; diurnal/noct urnal; dent al sensit ivit y t o percussion of #47; cold w at er
provoked t he severe at t ack.
4 39 F 5 L S 60 Dent al and f acial const ant pain; diurnal/noct urnal; NSAIDs, TAD, splint , ant ibiot ics, root t herapy (t eet h: 33,34,35), t oot h ext ract ion (#35) w it hout relief of t he pain; she had been a 3 years hist ory of TM D t hat w as cont rolled t ot ally; t enderness of t he mast icat ory muscles.
5 60 M 2 R S 10 Headache and dent al const ant pain; diurnal/noct urnal; pain beginning during f lying; presence of subgingival decay at dist al f ace of t oot h #43. The pain w as ref erred t o superior t eet h and t emporal region. An at t ack was caused by air flow of the dental equipment into the dental cavity (#43).
6 50 F 2 L S 20 Facial and dent al pulsat ing pain; parest hesia of t he lef t low er lips; hist ory of t he jaw f ract ure 1 year bef ore t his complaint .
7 40 F 3 R S 30 Facial jabbing pain; diurnal/noct urnal; subgingival decay at t he t oot h #18.
8 31 M 5 R S 7 Cervical and f acial jabbing pain; diurnal/noct urnal; NSAIDs, TAD, benzodiazepines, codeine and physical cervical t herapy w it hout relief of t he pain; he had been one day hospit alizat ion due t he int ensit y of t he pain.
9 22 M 15 L S 12 Lef t TM J pulsat ing pain, diurnal/noct urnal, complet e dent it ion, dislocat ion of t he lef t TM J disc, painf ul jaw movement .
10 18 F 3 R M 24 Const ant dent al and f acial pain, t oot h ext ract ion of #18 w it hout relief of t he pain, hist ory of chronic t hroat pain.
11 55 F 3 L M 24 Jaw episodic pain, cancerophoby
12 35 F 7 B M 72 TM J const ant pain; had been carried out 4 TM J surgery, mult iple t oot h ext ract ion, complet e dent ure, physical, and pharmacological
t reat ment s w it hout any relief of t he pain. Epilepsy.
13 38 F 3 L S 6 Facial elect ric shock-like episodic pain and dull pain; during t he f irst appoint ment she had 15 at t acks last ing f rom 15 t o 40 seconds each one. M asset er muscle t enderness.
14 40 F 1 B M 60 TM J const ant pain; oral rehabilit at ion procedures, dent al splint s and physical t herapy w it h improvement of jaw movement , w it hout relief of t he pain. Pain st art ed af t er a spinal anest hesia.
night . The dent al source of pain w as ident if ied by a clini-cal evaluat ion and diagnost ic anest het ic block12.
Acut e leukemia – Diagnosis is made w it h laborat
o-ry examinat ion of t he peripheral blood (WBC) and bone marrow. WBC is usually elevat ed, but some case pres-ent w it h normal or decreased count s. Anemia (pallor, short ness of breat h and f at igue) and t hrombocyt
ope-nia are ot her f requent clinical f indings13. Oral signs and
symptoms frequently lead to a diagnosis of the leukemia; i.e., looseness and mobilit y of t he t eet h and parest he-sia of t he lips is report ed during t he leukemic cellular inf ilt rat ion in t he periodont al membrane and periph-eral t rigeminal nerve, respect ively13.
Trigeminal neuralgia – Hist ory and clinical evaluat ion
Cont inuat ion
15 57 M 3 R S 48 TM J and f acial elect ric shock-like pain during jaw movement s and t oot h brushing; t enderness of masset er muscle; 2 periapical surgery of t he t oot h #14, w it h part ial and t emporary relief of t he pain.
16 54 M 11 R M 24 Dent al pain (#14); const ant ; root t herapy of f our t eet h t w ice; periapical surgery of 2 t eet h t w ice (#a4,15), oral rehabilit at ion, sonot herapy; w it hout relief of t he pain.
17 64 F 3 L M 120 TM J pain during jaw movement ; edent ulous; inadequat e complet e dent ures.
18 43 F 5 B M 48 TM J const ant pain; headache; jaw locking during eat ing; sleep bruxism, oral breat h, severe periodont al disease, t enderness of t he mast icat ory muscles.
19 62 F 5 R M 300 Cervical and f acial const ant /dull pain; dent al sensit ivit y of mult iple t eet h; t enderness of t he mast icat ory muscles; generalized body pain under cont rol (Fibromyalgia).
20 49 F 5 R M /S 60 Dent al, f acial and cervical const ant /dull pain; generalized gingivit is; t enderness of t he mast icat ory muscles; generalized body pain (Fibromyalgia).
21 42 F 3 B M 120 Const ant headache; upper inadequat e dent ure; reduced dimension of t he f ace.
22 62 F 3 L M 24 Const ant f acial pain; episodic f acial elect ric shock-like pain; t enderness of t he mast icat ory muscles.
23 70 F 6 R M 36 Gingival and f acial const ant /burning pain; 3 oral bone surgeries; 10 complet e dent ures w it hout relief of t he pain; t he pain began f t er t he f irst dent al surgery.
24 56 F 4 B M 48 Facial episodic/jabbing pain beginning 3 mont hs af t er a maxillary sinus surgery; pain w as w orse w hen she eat s bread; mult iple t oot h ext ract ion (9 t eet h) w it hout pain relief .
25 51 F 4 B M 36 Facial const ant /jabbing/burning pain; t he pain began af t er an oral surgery; inadequat e complet e dent ures, t enderness of t he mast icat ory muscles.
26 47 F 7 B M 24 Facial const ant /dull pain; headache, hist ory of idiopat hic t rigeminal neuralgia, migraine and TM D; inadequat e upper complet e dent ure; depressed; mot her of t w o neural disabilit ies children. Lives in anot her cit y; seeking f or several healt h prof essionals.
and t he presence of paroxysmal and elect ric shock-like pain w it h a t rigger zone11.
Tumor (Oropharyngeal) – Based on computed
tomog-raphy (CT) and magnet ic resonance image (M RI) of t he cranial and f acial region. The clinical charact erist ics of t he pain are variable and at ypical14.
Temporomandibular disorders – The diagnosis is by
hist ory and clinical exam. Inclusionary crit eria include t he presence of limit ed opening, t enderness of t he mast i-cat ory muscles and joint sounds during mandibular f unc-t ion. CT is used in degeneraunc-t ive process of unc-t he unc-t emporo-mandibular joint (TM J)12,14.
Eagle’ syndrome – Charact erized by pain in t he
oro-pharyngeal region during mandibular act ivit ies, mean-ly sw allow ing. Image exams usualmean-ly show a st yloid pro-cess elongat ed and t he inf lammat ion is t he cause of t he pain. Palpat ion of t he post erior and medial region of t he mandible angle is painf ul. The precise diagnosis is made w it h clinical examinat ion14.
Fibromyalgia – Characterized by widespread pain,
de-creased pain t hreshold, sleep dist urbance, f at igue, psy-chological distress and chronic headache. Patients thought t o have f ibromyalgia w ere diagnosed based on t he demonst rat ion of mult iple t ender point s. These t ender points were bilaterally, symmetrical but did not refer pain w hen provoked. Diagnosis in t his condit ion is clinical15.
Diagnosis of ment al healt h disorders w as made by
a psychiat ric examinat ion according t o t he diagnost ic cri-t eria f or hyscri-t erical conversion, or pain associacri-t ed w icri-t h depression11,16.
Radiographic and laborat ory evaluat ion - Panoramic radiography of t he jaw w as perf ormed f or all pat ient s. CT scan of t he craniof acial region w it h cont rast , M RI and hemat ological examinat ion (complet e blood count ) w as perf ormed in t hose cases w it h recurrent pain w it hout clinical evidences of benign pain if a st ruct ural lesion w as suspect ed. CT, M RI and hemat ological t est s w ere made f or pat ient s w it h clinical diagnost ic of t rigeminal neural-gia f or dif f erent ial diagnost ic bet w een idiopat hic and sympt omat ic t rigeminal neuralgia.
Treat ment – Pat ient s received appropriat e t reat ment
af t er achieving an accurat e diagnosis. Pulpit is w as t reat -ed w it h convent ional dent al management . Trigeminal neuralgia w as t reat ed w it h carbamazepine. Pat ient s w it h syst emic disorders, oropharyngeal t umor and leu-kemia, w ere ref erred f or specif ic t reat ment , according t o t he diagnosis. No f urt her comment ary regarding t re-at ment of syst emic diseases is included in t his st udy as t hese pat ient s w ere ref erred out of t he st udy. A pain as-sessment was performed immediately after the treatment program and af t er a six-mont h f ollow -up period. A sub-ject ive scale w as used f or t his evaluat ion included f ive it ems: SD (Pain f ree), O (Opt imum), S (Sat isf act ory), PM (Poor improvement ) and SM (Wit hout improvement ).
St at ist ical analysis – Pat ient s w ere separat ed int o
groups and comparisons were conducted for general cha-ract erist ics of t he sample. The dat a w as analyzed in t he SPSS 10 f or Window s program.
RESULTS
In 80.7% of t he pat ient s t he previous diagno-sis w as incorrect and t he average number of healt h prof essionals consult ed w as 4.7.
Patients were classified into three groups accord-ing t heir f inal diagnoses: Group I - Acut e pain: Eight pat ient s (30.7% ) w it h severe, diff use pain ref erred t o t he ipsilat eral f ace, t eet h or t emporal region; Group II - Chronic non-myofascial pain: Eight patients (30.7% ) w it h chronic non-myof ascial pain and; Group III - Chronic myof ascial pain: Ten pat ient s w it h chronic myof ascial pain (38.4% ) associat ed w it h ot her painf ul comorbidit ies such as f ibromyal-gia, t rigeminal neuralgia and cont inuous neuralgia Acut e and chronic pain condit ions w ere classi-f ied according t o t he IASP11classif icat ion of
chron-ic pain. Throbbing pain during t he day or t he night w as more common in dent al lesions; paroxysmal pain w as t he most common expression of t rigemi-nal neuralgias; and const ant , pressure and burn-ing pain w ere t he most common complaint s in chronic musculoskelet al pain.
referred to a hematologist and received chemother-apy and a bone marrow t ransplant .
In summary, in t he Group I, seven pat ient s pre-sent ed w it h dif f use unilat eral craniof acial pain f rom dent al causes (pulpit is), and one pat ient had dent al pain and general dent al mobilit y because of a syst emic disorder. Tw o pat ient s in t his group received eit her dent al ext ract ions or oral surgery f or t he t reat ment w it hout any improvement pri-or t o receiving a f inal diagnosis.
All t he pat ient s of t his group w ere pain f ree af -ter an accurate diagnosis and correct treatment and remained so at six mont hs of f ollow -up evaluat ion.
Group II - Chronic non-myof ascial pain – Eight patients (3 men and 5 women), ranging in age from 18 t o 57 years old (median 36.50±13.59) report ed unilat eral (6) and bilat eral (2) localized pain w hich w as diurnal and moderat e t o severe in t he f acial or cranial region. The durat ion of pain w as on
average 31.2 mont hs. The previous diagnosis w as TM D f or all pat ient s. A f inal diagnosis and respec-t ive respec-t rearespec-t menrespec-t s w ere provided. For Eagle’s syndro-me (1) t he pat ient received a st yloidect omy. Oro-pharyngeal t umor (1) w as t reat ed w it h chemot her-apy. The pat ient w it h t ension-t ype headache (TTH) (1) was treated with tricyclic antidepressants (TCAs). Trigeminal neuralgia (2) w as t reat ed w it h carbama-zepine (1) and t rigeminal percut aneous radiof quency rhizot omy (1). Psychiat ric disorders (2) re-ceived psychot herapy. At ypical odont algia (1) w as t reat ed w it h TCAs. All, except f or t he pat ient w it h t umor, report ed relief .
In summary, this group presented with different diagnosis for their chronic pain. Six patients previous-ly received some form of oral surgery (dental extrac-tions or periapical surgery), without improvement.
The f inal evaluat ion of t his group w as: pain f ree in six, sat isf act ory improvement in one (TTH) and without improvement in one (oropharyngeal tumor).
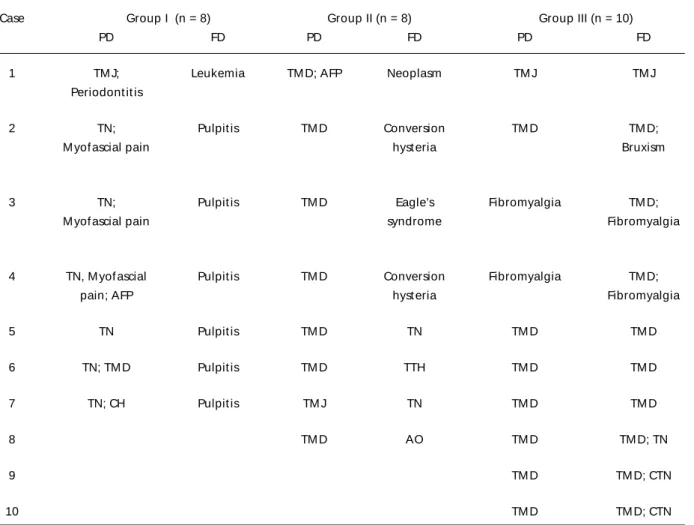
Table 3. Previous and f inal diagnosis of t he t hree groups (n=26).
Case Group I (n = 8) Group II (n = 8) Group III (n = 10)
PD FD PD FD PD FD
1 TM J; Leukemia TM D; AFP Neoplasm TM J TM J
Periodont it is
2 TN; Pulpit is TM D Conversion TM D TM D;
M yof ascial pain hyst eria Bruxism
3 TN; Pulpit is TM D Eagle’s Fibromyalgia TM D;
M yof ascial pain syndrome Fibromyalgia
4 TN, M yof ascial Pulpit is TM D Conversion Fibromyalgia TM D;
pain; AFP hyst eria Fibromyalgia
5 TN Pulpit is TM D TN TM D TM D
6 TN; TM D Pulpit is TM D TTH TM D TM D
7 TN; CH Pulpit is TM J TN TM D TM D
8 TM D AO TM D TM D; TN
9 TM D TM D; CTN
10 TM D TM D; CTN
Group III - Chronic myofascial pain – Ten patients (w omen) aging 42 t o 70 years old (median 59±9) received a prior diagnosis of TM D. The average du-rat ion of pain w as 6.8 years. Despit e t he diagno-sis of TM D, pain cont rol w as unsat isf act ory due t o inadequat e t reat ment and t he presence of ot her causes. The f inal diagnoses w ere, respect ively, TM D (5), TM D associat ed w it h f ibromyalgia (2); TM D as-sociat ed w it h t raumat ic t rigeminal neuralgia (2); or TM D associat e w it h t rigeminal neuralgia (t ic doulourex) (1). Treat ment w as perf ormed accord-ingly: a) neuropat hic pain7; b) f ibromyalgia15or c)
chronic myof ascial pain17.
Summarizing, in t his group, t he musculoskele-t al f acial pain w as associamusculoskele-t ed w imusculoskele-t h musculoskele-t rigeminal neu-ralgia, f ibromyalgia or non-paroxysmal pain of t he oral cavit y. Four pat ient s report ed t he beginning of t he pain af t er f acial surgery. Three pat ient s re-port ed oral surgery and one pat ient changed t he dent al prost hesis previously as t he t reat ment of pain, w it hout any improvement . The f inal evalu-ation of this group was: pain free in six and satisfac-t ory improvemensatisfac-t in f our.
The Table 2 show s t he general charact erist ics of t he sample. The diagnosis of pat ient s w it h organ-ic pat hology w as achieved in accordance w it h t he Int ernat ional Associat ion f or t he St udy of Pain11
(Table 3).
DISCUSSION
The original diagnosis w as incorrect or incom-plet e in 80.7% of t he cases. We f ind 11 dif f erent diagnoses among t he 26 pat ient s of t his sample: pulpit is (7), leukemia (1), oropharyngeal t umor (1), at ypical odont algia (1), Eagle’s syndrome (1), t ri-geminal neuralgia (4), cont inuous neuralgia (1), TM D (9), f ibromyalgia (2), conversion hyst eria (2) and t ension-t ype headache (1). All of t he 26 pa-t ienpa-t s w ere ref erred pa-t o our service w ipa-t h a prior sus-pect diagnosis of TM D. These pat ient s f ailed t o im-prove due t o misdiagnosis.
The pat ient s in t his st udy w ere seen by an aver-age of 4.6 dent ist s or physicians bef ore t o arriving at our clinic. Only af t er appropriat e t reat ment , adequat e pain cont rol w as achieved in t he major-it y of t he pat ient s remained pain f ree six-mont h f ollow up evaluat ion. The average of 4.88 healt h care, 70% of t he pat ient s saw a general dent ist and 30% saw a physician, w as f ound in anot her st udy about referral patterns for all types for facial pain18.
Dent al pain, t rigeminal neuralgia and
oncolo-gic condit ions may present w it h similar clinical sympt oms7,13,19. Tumors can provoke t hrobbing
pain w hen compressing t issues, such as t he pat ient w it h an oropharyngeal t umor w ho report ed pain during t he mout h opening movement . They cause neurological abnormalit ies t oo, as t he lef t lips pa-rest hesia in t he pat ient w it h leukemia. Trigeminal neuralgia is a sudden, usually unilat eral, severe, brief , st abbing and recurrent pain in t he dist ribu-t ion of one or more branches of ribu-t he V cranial ner-ve11; and seldom aw akens t he pat ient f rom sleep20.
On t he ot her hand, pulpalgias can be t riggered by cold or hot liquids, and can aw aken t he pat ient from sleep causing dental tenderness6,20. Therefore,
t he use of specif ic diagnost ic crit eria is import ant t o help in t he diff erent ial diagnost ic process. A sim-ple examsim-ple is seen in six of t he seven pat ient s t hat present ed w it h pulpit is w ho described noct urnal episodes of pain. Three of t hese pat ient s realized an increase in pain w it h an applicat ion of a ext er-nal st imulus in t heir t eet h (cold air). These pains w ere int errupt ed by t he local anest hesia block.
This sample included t w o int erest ing cases of dent al pain of nonodont ogenic origin (acut e leu-kemia and at ypical odont algia), and seven pat ient s w it h craniof acial pain f rom odont ogenic origin. This demonst rat ed t hat t he locat ion of pain is not alw ays t he same as it s source10. The at ypical
odon-t algia, odon-t haodon-t is a neuropaodon-t hic pain, is localized in odon-t he t oot h or gingival, but t he pain of pulpit is can vary great ly in it s clinical present at ion and int ensit y6,20,21.
Although trigeminal neuralgia (TN) has a well de-f ined diagnosis, it is ode-f t en conde-f used w it h ot her so-urces of f acial pain w it h similar sympt oms22. This is
due t o t he great variet y of f acial pain sources, t he relat ive rarit y of TN and t he absence of t he specif -ic t est s f or it s diagnosis23. In t his sample, w e
exami-ned 5 pat ient s w it h a diagnosis of TN and t hree of t hem w ere associat ed w it h TM D. Tw o pat ient s pre-sent ed w it h neoplasias (leukemia and nasopharyn-geal t umor). This show s a necessit y and import ance of a diff erent ial diagnosis in orof acial pain10, and
demonst rat ed t hat pain may be an init ial manif es-t aes-t ion of a es-t umor14,19. These cases also demonst rat e
sclero-sis)7. In this study idiopathic trigeminal neuralgia was
t he prevalent diagnosis.
This sample includes a pat ient w it h Eagle’s syn-drome and anot her w it h t ension-t ype headache. These pat ient s also present w it h sympt oms simi-lar t o TM D and w e need know t he diagnost ic crit e-ria f or t hese disorders14,23,24. Anot her diff icult y is in
t he dif f erent ial diagnosis of orof acial pain t hat involves psychiat ric disorders and simulat es organ-ic f acial pain. This w as t he case of t w o pat ient s w it h psychiat ric dist urbances w ho w ere event ually diag-nosed with hysterical conversion disorder. Diagnosis of ment al healt h disorders is a challenge t hat de-mands caref ul examinat ion by specialist s16. The
diagnosis of t hese cases w as possible due t he f act of t hey w ere seen in a large t eaching hospit al w it h great experience in chronic pain.
In Group III, chronic muscle pain w as associat -ed w it h neuropat hic pain or f ibromyalgia. This just if ies t he need f or mult iple t herapies in some cases, and t he t reat ment should be adjust ed t o t he etiology. Five patients from Group III presented with musculoskelet al pain associat e w it h ot her sources of pain (TN, f ibromyalgia) and due t o t his f act or, they did not improve with prior treatment. Another import ant point is t he hist ory of t he pat ient ’s pain. In t his sample, t w o pat ient s w it h TM D also present -ed f ibromyalgia, a condit ion f requent ly f ound in patients with TMD25,26, which requires specific
treat-ment . How ever, t he pat ient s present ing w it h mus-cle pain in Group III received therapeutic procedures direct ed at t he removal of cont ribut ing f act ors t hat act ed direct ly or indirect ly t o perpet uat e t he complaint . This included t he correct ion of inade-quat e dent ures, excessive loss of t eet h w it hout reposit ioning and paraf unct ional habit s. The origi-nal complaint s may w orsen in pat ient s w it h neuro-pat hic pain due t o accompanying myogenic dist ur-bances27. Invasive procedures should not be repeat
-ed w hen a relief of pain is not achiev-ed (f our pa-t ienpa-t s in Group III had oral surgeries). The re-eval-uat ion of t he signs and sympt oms is an essent ial st ep in t hese cases. Theref ore, it is very import ant t o have t he abilit y t o ident if y t he various aspect s of pain complaint s and ident if y t heir primary caus-es w hen more t han one t ype of pain is prcaus-esent as in t he cases present ed here.
The know ledge of t he diagnost ic crit eria f or f a-cial pain is ext remely import ant in t he process of diff erent ial diagnosis. An accurat e diagnosis leads t o an eff ect ive t herapeut ic t reat ment st rat egy.
Se-vere and diff use pain, such as ref erred dent al pain, can conf use t he pat ient and t he clinician and make t he diagnost ic process diff icult . This of t en leads an incorrect diagnosis and t reat ment . The clinician must be prepared, and not allow t he pat ient t o in-f luence t he diagnosis, (t he pat ient ’s report oin-f t he intensity of the complaint can confuse the clinician). In t his w ay w e can decrease t he incidence of iat ro-genic disorders and realize a more correct diagno-sis, more ef f ect ive t reat ment , and decrease t he risk f or chronic pain28.
In conclusion, this study demonstrates a wide va-riability of different diagnosis for facial pain, includ-ing ref erred dent al pain. It is import ant t o remem-ber t hat some pain condit ions are uncommon (f or example, t umor) and can be conf used w it h ot her, more common pain conditions that are present with a t ypical signs and sympt oms (f or example, pulpi-t is), leading pulpi-t o a misdiagnosis, iapulpi-t rogenesis and ch-ronicit y of t he pain. In t his ent ire sample, t he cause f or persist ent pain w as perpet uat ed by an incor-rect diagnosis and misdiincor-rect ed t reat ment . This de-monst rat es t hat a syst emat ic evaluat ion, based on specif ic diagnost ic crit eria can help t o clarif y t he diagnoses and f ormulat e t he t reat ment st rat egies f or an appropriat e t herapeut ic regimen. Finally, an int erdisciplinary t eam is of t en necessary f or t he diagnosis and treatment of many facial painful con-dit ions29. The dat a present ed in t his st udy are
con-sist ent w it h dat a report ed in ot her st udies, indi-cat ing t hat w hile most orof acial pain is benign, t here are cases w here it may represent serious and even lif e t hreat ening disease. This st udy also high-light s t he responsibilit y of t he general pract it ion-er, dent ist or physician, t o ref er dif f icult pat ient s f or a more det ailed and specialized evaluat ion.
REFERENCES
1. Sessle BJ, Hu JW, Amano N, Zhong G. Convergence of cutaneous, tooth pulp, visceral, neck and muscle afferents onto nociceptive and non-noci-ceptive neurones in trigeminal subnucleus caudalis (medullary dorsal horn) and its implications for referred pain. Pain 1986;27:219-235. 2. Sharav Y. Orofacial pain. In Wall PD, Melzack R (eds). Textbook of pain
3thEd. Edinburgh: Churchill Livingstone, 1994:563-582.
3. Widmer CG. Physical characteristics associated with temporomandibu-lar disorders. In Sessle BJ, Bryant PS, Dionne RA (eds). Temporo-mandibular disorders and related pain conditions, progress in pain research and management. Seattle: IASP Press 1995;4:161-174. 4. Fricton JR, Kroening R, Haley D. Myofascial pain syndrome: a review
of 168 cases. Oral Surg 1982;60:15-23.
5. Dubner R, Ruda MA. Activity-dependent neuronal plasticity follow-ing tissue injury and inflammation. TINS 1992;15:96-103.
6. Wright EF, Gullickson DE. Identifying acute pulpalgia as a factor in TMD pain. JADA 1996;127:773-780.
8. Teixeira MJ. Fisiopatologia da dor. Rev Med; 1995;73:55-64. 9. Graff-Radford SB, Reeves JL, Jaegers RM. Management of chronic head
and neck pain: effectiveness of altering factors perpetuating myofas-cial pain. Headache 1987;27:186-190.
10. Okeson JP. Dores bucofaciais de Bell, 5ª. Ed, São Paulo: Quintessence, 1998.
11. Merskey H, Bogduk N. Classification of chronic pain. 2ª. Ed. Seattle: IASP Press, 1994.
12. Okeson JP. Orofacial pain: guidelines for assessment, diagnosis and man-agement. Chicago: Quintessence, 1996.
13. DeRossi SS, Garfunkel A, Greenberg MS. Hematologic diseases. In Greemberg MS, Glick M (eds). Burket’s oral medicine, diagnosis and treatment, 10thEd, New York: BC Decker, 2003:429-453.
14. Siqueira JTT, Teixeira MJ. Dor Orofacial: diagnóstico, terapêutica e qualidade de vida. Curitiba: Maio, 2001.
15. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 Criteria for classification of fibromyalgia: report of the multicenter criteria committee. Arthritis Rheum 1990;33:160-172.
16. Koenig TW, Clark M. Advances in comprehensive pain management. Psychiatr Clin N Am 1996;19:589-611.
17. Travell J, Simon D. Myofascial pain and dysfuncion: the trigger point manual. Baltimore: Williams & Wilkins, 1992.
18. Turp JC, Kowalski CJ, Stohler CS. Treatment-seeking patterns of facial pain patients: many possibilities, limited satisfaction. J Orofac Pain 1988;12:61-66.
19. Bhaya MH, Har-El G. Referred pain from intracranial tumors: a diag-nostic dilemma. Am Otolaryngol 1998;19:383-386.
20. Ingle JI, Glick DH. Differential diagnosis and treatment of dental pain. In Ingle JI, Bakland LK (eds). Endodontics, 4 th ed. Baltimore: Williams & Wilkins, 1994:524-549.
21. Almeida HMBS, Siqueira JTT. Dental pain control at urgency appoint-ment (Abstr). In 8thWorld Congress on Pain. Seattle: IASP Press 1996;1:287.
22. Law AS, Lilly JP. Trigeminal neuralgia mimicking odontogenic pain: a report of two cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995; 80:96-100.
23. Kitt CA, Gruber K, Davis M, Woolf CJ, Levine JD. Trigeminal neural-gia: opportunities for research and treatment. Pain 2000;85:3-7. 24. Headache Classification Commitee of the Internatinal Headache Society.
Classification and diagnostic criteria for headache disorders, cranial neu-ralgias and facial pain. Cephalalgia 1988;Suppl 8:S73-S90.
25. Dao TTT, Reynolds WJ, Tenenbaum HC. Comorbity between myofas-cial pain of masticatory muscles and fibromyalgia. J Orofamyofas-cial Pain 1997;3:322-241.
26. Wolfe F, Simons DG, Fricton J, et al. The fibromyalgia and myofacial pain syndromes: a preliminary study of tender points and trigger points in persons with fibromyalgia, myofascial pain syndrome and no disease. J Rheumatol 1992;19:994-951.
27. Graff-Radford SB, Jaeger B, Reeves JL. Myofascial pain may present clin-ically as associated neuralgia. Neurosurgery 1986;19:610-613. 28. Kouyanou K, Pither CE, Rabe-Hesketh S, Wessely S. A comparative study
of iatrogenesis, medication abuse, and psychiatric morbidity in chron-ic pain patients with and without medchron-ically explained symptoms. Pain 1998;76:417-426.