Arq Neuropsiquiat r 2001;59(4):839-842
DIFFUSION-WEIGHTED M R IM AGING OF
CYSTIC LESIONS OF NEUROCYSTICERCOSIS
A prelim inary st udy
Luciana S. Raf f in
1, Luiz A. Bacheschi
2, Luis R. M achado
3,
José P.S. Nóbrega
3, Christ ina Coelho
1, Claudia C. Leit e
4ABSTRACT - Neurocysticercosis is an endemic disease in some developing countries. It has pleomorfic clinical and imaging findings, w hich are variable from pat ient t o pat ient . In t his preliminary not e, w e st udied t he magnet ic resonance (M R) diffusion-w eight ed images (DWI) of sixt een pat ient s present ing w it h cyst ic lesions of this disease diagnosed by clinical and laboratorial findings. All the lesions had hypointense signal and the similar apparent diffusion coeficient (ADC) values as t he cerebrospinal fluid (CSF).
KEY WORDS: neurocyst icercosis, cyst ic lesion, M RI, diffusion images.
Imagens por difusão de ressonância magnética em lesões císticas da neurocisticercose: estudo preliminar
RESUM O - Neurocist icercose é doença endêm ica em alguns países em desenvolvim ent o. Ela apresent a asp ect os clínicos e de im agem que variam em cada pacient e. Nest a not a prelim inar expom os um est udo ut ilizando im agens ponderadas em dif usão em dezesseis pacient es que apresent avam lesões císt icas da neurocist icercose comprovada clínica e laborat orialment e. Todas as lesões examinadas apresent aram hipo-sinal com int ensidade de hipo-sinal e valores de coef icient e de dif usão aparent e (CDA) sim ilares ao do líquido cef alorraquiano.
PALAVRAS-CHAVE: neurocist icercose, cist os int racranianos, ressonância magnét ica, imagem por difusão.
From Neurology and Radiology Depart ment s, Universit y of São Paulo M edical School. Neurology Depart ment : 1Post -graduat e st udent ; 2Associat e Professor; 3Assist ant Professor, Radiology Depart ment ; 4Associat e Professor.
Received 12 July 2001. Accept ed 21 August 2001.
Dr. Luiz A. Bacheschi – Divisão de Neurologia, HC, FM USP – Av. Dr. Enéas de Carvalho Aguiar 255 - 05403-010 São Paulo SP - Brasil. E-mail: bacheschi@henet .usp.br
Neurocyst icercosis is t he m ost im port ant parasi-t ic disease parasi-t haparasi-t af f ecparasi-t s parasi-t he nervous sysparasi-t em , and iparasi-t is a public healt h problem in t he developing count ries, m ainly in Cent ral and Sout h Am erica, Af rica and Asia1. It is relat ed t o t he poor sanit ary condit ions of
t he populat ion1, 2. In Brazil, neurocyst icercosis is
en-dem ic in som e areas in t he sout h and t he sout heast regions2. There are different clinical manifest at ions,
depending upon t he pat hological f indings and t he phase of evolut ion of t he disease. The clinical signs or sym pt om s can t ake from 1 t o 35 years aft er t he inf est at ion t o show up3. The m ost f requent clinical
present at ions include: epilepsy, m eningit is, int rac-ranial hypert ension and cognit ive disabilit y2,4. An
asym pt om at ic f orm can be seen in som e pat ient s4.
The im aging f indings on com put ed t om ography (CT) and m agnet ic resonance (M R) as w ell as t he follow -up of this disease have been studied5,6.
Neuro-im aging exam s usually are able t o est ablish t he
di-agnosis w hen t here are def init ive signs of t he para-sit e, like t he scolex inside a cyst ic lesion. Because t hese lesions are usually of variable size, w it h or w it h-out edema or peripheral enhancement , and t he sco-lex som et im es is not det ect able, a list of dif f erent ial diagnosis including ot her cyst ic lesions due t o infec-t ions or infec-t um ors should be considered.
The biologic w at er has random t ranslat ional mo-t ion (Brow nian m omo-t ion) of imo-t s m olecules caused by t heir t herm al energy and t he viscosit y of t he m e-dium7. This kind of m ot ion is relat ed t o t he
appar-ent dif f usion coef f iciappar-ent (ADC) and M R using dif f u-sion w eight ed im ages (DWI) can evaluat e it . The im age acquisit ion is achieved by applying st rong m agnet ic f ield gradient pulses in a T2-w eight ed se-quence. The signal det ect ion is based in prot ons de-phased and rede-phased af t er t he applicat ion of t he m agnet ic gradient s8. Only st at ionary prot ons w ill
840 Arq Neuropsiquiat r 2001;59(4)
rest rict ion of t he diffusion or reduces t he t ranslat io-nal m ovem ent , t he decreased ADC in t he lesion w ill be represent ed by a bright area in DWI in com pari-son t o t he unaf f ect ed t issue9.
The m ost im port ant clinical applicat ions of t he DWI is t he evaluat ion of acut e cerebral ischem ia9,
but new uses have been st udied like in t he dif f eren-t ial diagnosis beeren-t w een ineren-t racerebral necroeren-t ic eren-t umors and abscesses10,11, arachnoid cyst s and epiderm oid
t umors12 and t he evaluat ion of brain neoplasias13,14.
The DWI also seem s t o provide com plem ent ary in-f orm at ion in t raum at ic brain injury, dem yelinat ion disease and Creut zf eldt -Jakob disease15.
This is a prelim inary st udy in w hich w e obt ained M R axial unenhanced T1, T2, Flair and m ult iplanar enhanced T1-w eight ed im ages, and t he dif f usion-w eight images in cyst ic lesions of pat ient s usion-w it h neu-rocyst icercosis, in order t o det erm inat e a dif f usion-w eight ed pat t ern of t hese cyst ic lesions t hat aids in different ial diagnosis.
M ETHOD
We st udied prospect ively sixt een pat ient s w it h neuro-cyst icercosis conf irm ed by laborat orial f indings t hat w ere f ollow ed in t he Neurologic Clinic of Hospit al das Clínicas da Universidade de São Paulo (USP).
The ages of t he pat ient s ranged f rom 19 t o 60 years (m ean age 39,5 years). Tw elve subject s w ere m ale and four w ere female. Fift een of t hem present ed w it h epilepsy. One of t hese pat ient developed bilat eral f acial palsy and sw allow ing dif f icult ies, w hich w ere probably caused by a large cyst in t he IV vent ricle. One pat ient init ially present ed w it h headache and vom it s, being diagnosed int racranial hypert ension, and she w as submit t ed t o a vent ricular-peri-t oneal shunricular-peri-t . One paricular-peri-t ienricular-peri-t w iricular-peri-t h ricular-peri-t he largesricular-peri-t lesion (5.0 cm ) w as subm it t ed t o a st ereot at ic biopsy of t he cyst ic w all and drainage of it s cont ent s, aft er t he M R st udy.
All t he exam inat ions w ere perform ed in a 1.5 T w hole-body im ager (Signa Horizon LX: GE M edical Syst em ) ca-pable of echo planar im aging. DWI w as perf orm ed w it h a
m ult isect ion, single shot , echo planar spin-echo sequence w it h TR= 9999 m s, TE= 105 m s, NEX= 1, FOV= 24x19 cm , 96x128 m at rix, 5.0 m m slice t hickness w it h no gap and high-st rengt h dif f usion gradient (B = 1000 sec/m m2). The
dif f usion gradient w as applied along t hree direct ions (X, Y, and Z) and t he ADC m aps w ere calculat ed in all direct ions. ADC m easurem endirect w as done using a variable diam -et er ROI m anually placing in a select ed lesion (t he largest one). The cyst s had dif f erent sizes, so t he ROI dim ensions varied w it h t he lesion size.
ADC values of t he CSF inside t he lat eral vent ricles and in t he norm al parenchym al w ere m easured in all pat ient s t o com pare t o t he values of t hose obt ained in t he cyst ic lesions.
Co n ven t io n al u n en h an ced axial SE T1 (TR500m s/ TE14m s/NEX2), FSET2 (TR4500m s/ TE100m s/NEX2) and FLAIR(TR8402m s /TE142m s/TI2100m s/NEX2) w ere per-formed before DWI. Coronal, axial and sagit al T1-w eight ed w ere also obt ained af t er cont rast adm inist rat ion (Gado-linium :10 m M ol/Kg).
RESULTS
All pat ient s had cyst ic lesions w it h signal int ensi-t y similar ensi-t o ensi-t he CSF, w iensi-t h or w iensi-t houensi-t peripheral ede-m a and/or enhanceede-m ent . Tw elve pat ient s had only parenchymal lesions, tw o patients had cisternal cysts (racem ose f orm ) and t w o pat ient s had com bined f orm s, one w it h int ravent ricular and parenchym al cyst s and t he ot her w it h racem ose and parenchy-m al lesions. The lesions w ere solit ary in t hree pat ienpat s and m ulpat iples in pat hirpat een; pat he largespat diam -et er of t he lesions ranged f rom 0,5 t o 5.0 cm .
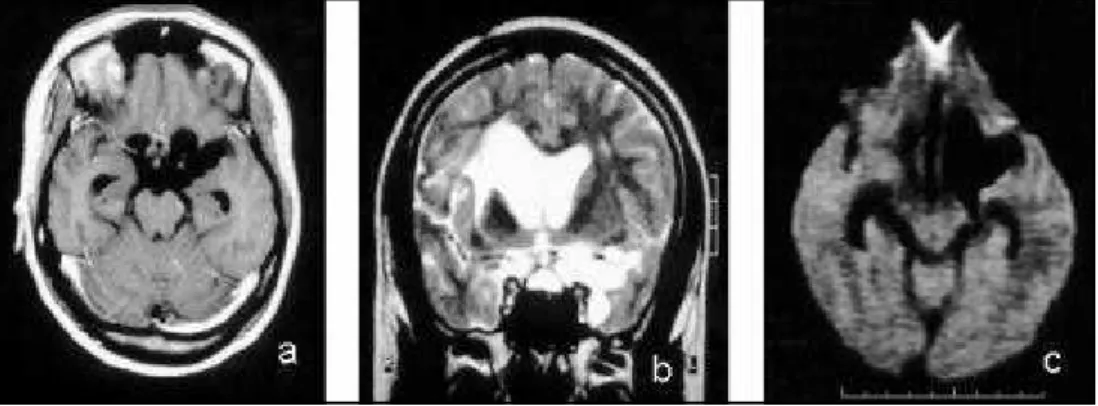
The cyst ic lesions present ed sim ilar signal int en-sit y as t he CSF on T1, T2 and FLAIR im ages. On DWI t he lesions w ere hypoint ense, comparable t o or slig-ht ly hyperint ense t han t he CSF signal int ensit y. There w as no signif icant dif f erence of t he signal int ensit y in t he lesions t hat exhibit ed peripheral enhancement or edem a f rom t hose t hat did not have t hese f ind-ings or among t he parenchymal, int ravent ricular and
Arq Neuropsiquiat r 2001;59(4) 841
racemose forms (Fig 1), except t he largest lesion (5.0 cm) and a case of racemose cysts w ith thick enhance-m ent , w hich had an het erogeneous cont ent w it h slight ly higher signal int ensit y t han t he CSF on DWI. In t he ADC maps, t he cyst s w ere as bright as t he CSF (Fig 2).
The calculat ed ADC values of t he cyst ic lesions ranged from 1.28 t o 3.10 x 10-3mm2/sec, t he CSF
ADC values ranged from 1.12 t o 3.50 x 10-3mm2 /sec
and t he brain parenchym a ADC values ranged f rom 0.70 t o 0.88 x 10–3mm2/sec (Table 1). There w as no
significant difference bet w een t he cyst ic lesions and
CSF calculated ADC values according to the non-para-m et ric st at ist ic analysis (Friednon-para-m an´ s t est ).
Eleven pat ient s had an eccent ric nodule adhered t o t he cyst ic w all corresponding t o t he scolex. In seven of t hese pat ient s t here w as a hyperint ense nodule on DWI on the same topography of the scolex (Fig 3). This nodule present ed t he same signal int en-sit y of t he parenchym a on t he ADC m ap. In a pa-t ienpa-t w ho had m ulpa-t iple cyspa-t s w ipa-t h scolex, DWI al-low ed ident if icat ion of a sm all hyperint ense nodule in t w o cyst s and in anot her pat ient it could be iden-t if ied a sm all hyperiniden-t ense nodule in only one cysiden-t . In t he rem aining four pat ient s, t he scolex w as easily dist inguished on t he T2-w eight ed images, alt hough it w as not seen in t he DWI. The scolex w as t oo sm all t o allow an appropriat ed ADC m easurem ent w it h-out cont am inat ion w it h t he f luid around it .
DISCUSSION
Neurocyst icercosis represent s an import ant pub-lic healt h problem , being endem ic in developm ent count ries1. The inf est at ion by t he parasit e w as
re-lat ed t o poor sanit ary condit ions. During it s
evolu-Table 1. Calculat ed ADC values according t o t he t ype of t issue st udied in 16 pat ient s w it h neurocyst icercosis.
Tissue Diffusion coefficient No. of (x10-3 mm2 /sec) m easurem ent s
M ean ± SD
cyst ic lesion 2.25 ± 0.57 16
CSF 2.34 ± 0.63 16
w hit e mat t er 0.79 ± 0.05 16
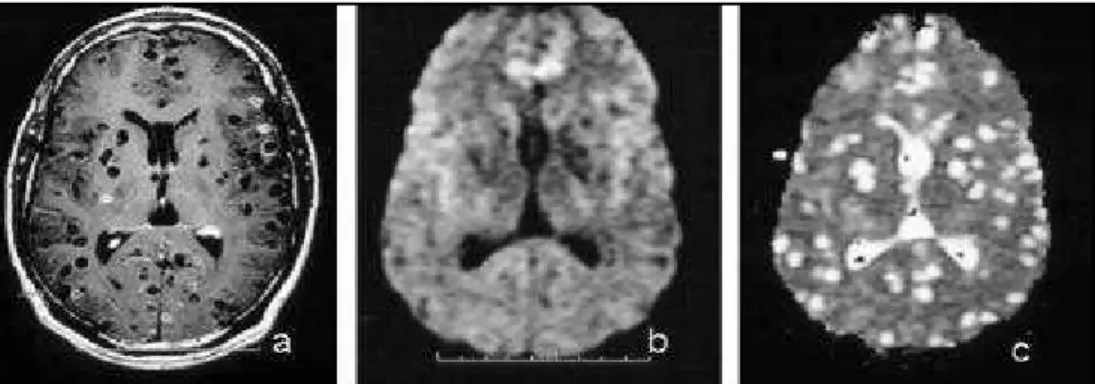
Fig 2. Dif f use parenchymal f orm, mult iple cyst ic lesions in dif f erent evolut ive st ages: a) Cont rast en-hanced axial T1 Wl; b) Axial diffusion Wl; c) Axial diffusion map.
842 Arq Neuropsiquiat r 2001;59(4)
t ion, t he disease can change it s present at ion in neu-roim aging exam s f rom a cyst t o a calcif ied nodule. The init ial phase is an egg-shaped cyst ic lesion w it h-out enhancem ent or edem a, and if t he scolex w as ident if ied t he diagnosis can be done w it h reason-able conf idence. But w hen it seem s like a cyst w it h peripheral enhancem ent and edem a w it hout scolex t he diagnosis is not so easy because t he ring-en-hancem ent m ass is a nonspecif ic im aging f inding and it can be seen in neoplast ic diseases and ot her infect ions10.
Diffusion-w eighted images is helpfull in the evalu-at ion of t raum evalu-at ic brain injury, dem yelinevalu-at ion dis-ease, Creut zf eldt -Jakob disease and t he dif f erent ial diagnosis betw een necrotic tumors and abscess10,11,15.
The necrot ic or cyst ic t um or present s signal int en-sit y similar t o t he CSF and t he calculat ed ADC values ranged from 0.3 t o 2.7 (1.69± 0.9) x 10–9 m2/s and
from 1.7 t o 3.8 (2.2± 0.9) x 10–3 mm2/s14.
The f indings seen in abscess w ere dif f erent . The abscess present s hyperint ensit y on DWI and low er ADC value ( 0.21 t o 0.34 x 10-3 mm2/s)10. The cyst ic
or necrot ic t um ors are also dif f erent f rom acut e is-chemic lesion, w hich present s hyperint ensit y on DWI (like t he abscess) and ADC values ranged f rom 0.29 t o 0.33 x 10-3 mm2/s, f or ischem ic lesions st udied
less t han 8 hours10 t o 0.48 ± 0,05 x 10-3 mm2/s9 lat er
on t he evolut ion of t he lesion.
In t his st udy, all t he neurocyst icercot ic cyst s had a signal int ensit y sim ilar or slight ly higher t han CSF in all sequences, including DWI. We did not find any hyperint ense lesion, even in t he colloidal st age, as w as relat ed in t he lit erat ure16, alt hough our ADC
va-lues ranged in a sim ilar f orm of t hose report ed. The calculat ed ADC values w ere not signif icant ly dif f er-ent bet w een t he CSF and t he neurocyst ycercosis cys-t ic lesions (Fig 1).
The small lesions w ere uneasy to see on DWI prob-ably because of t he low spat ial resolut ion, charac-t erischarac-t ic of charac-t his sequence. How ever, charac-t hey w ere easily recognized in t he ADC m ap independent ly of t he lesion size, because t he ADC m ap gives a m ore con-spicuous dif f erence bet w een t he signal of t he pa-renchym a and t he lesions t hat are hyperint ense on DWI (Fig 2).
In seven pat ient s w it h cyst ic lesions w it h scolex, at least one scolex w as det ect able as a very hyper-int ense nodule w it hin t he vesicle on DWI (Fig 3). The scolex represent s t he solid com ponent ; indeed it is t he larval body t hat probably causes enough w at er rest rict ion t o slow t his signal behavior on DWI. In
f our pat ient s none of t he det ect able scolex show ed t his hyperint ense signal. This f act should be a m at -t er of f ur-t her s-t udies, in order -t o explain w hy and how t he scolex present s hyperint ense signal on DWI.
CONCLUSIONS
In t his preliminary st udy, w e demonst rat e t hat t he cyst ic lesions of sixt een pat ient s w it h neurocyst i-cercosis present ed sim ilar signal int ensit y or slight ly higher t han t he CSF signal int ensit y. We show ed t hat DWI can be usef ul t o aid in t he est ablishm ent of t he different ial diagnosis bet w een abscesses and neurocyst icercot ic neurocyst s, since t hey can share sim ilar im -age findings in t he convent ional M RI, alt hough t hey have opposit e behavior in DWI and ADC m aps. In-creasing t he sam ple w ould give us a m ore reliable conclusion.
REFERENCES
1. Singh G. Neurocysticercosis in South-Central America and the Indian subcontinent: a comparative evaluation. A rq Neuropsiquiatr 1997; 55:349-356.
2. Teive HAG, Minguetti G, Sasaki MGM, Lopes CE, Carvalho MTM, Szpeiter N. Neurocisticercose: artigo de revisão. Rev Bras Neurol 1997; 33:147-153.
3. Mihai C, Mattson DH. Specific neurologic diseases manifesting as myelitis and myelo p athy. In: Clinical N euro lo gy o n CD-ROM, Lippincott-Raven Publishers, 1998, record 53077.
4. Zenteno-Alanis GH. A classification of human cysticercosis. In Flisser A, Wilms K, Laclette JP, Larralde C (eds). Cysticercosis: present state of knowledge and perspectives. New York: Academic Press, 1982:107-127. 5. Machado LR, Nobrega JPS, Barros NG, Livramento JA, Bacheschi LA, Spina-França A. Computed tomography in neurocysticercosis: a 10-year long evolution analysis of 100 patients with an apraisal of a new classification. Arq Neuropsiquiatr 1990; 48:414-418.
6. Dumas JL, Visy JM, Beli C, Gaston A, Goldlust D, Dumas M. Paren-chymal neurocysticercosis: follow-up and staging by MRI. Neuroradio-logy 1997;39:12-18.
7. Edelman RR, Weiskoff RM. Basic principles of MRI. In Edelman RR, Hesselink JR, Zlatin MB (eds). Clinical magnetic resonance imaging. 2.Ed. Philadelphia: Saunders 1996:22.
8. LeBihan D. Molecular diffusion nuclear magnetic resonance imaging. Mag Reson Q 1991; 7:1-28.
9. Beauchamp NJ Jr, Ulug AM, Passe TJ, van Zijl PCM. MR diffusion im-aging in stroke: review and controversies. RadioGraphics 1998; 18:1269-1283.
10. Desprechins B, Stadnik T, Koerts G, Shabana W, Breucq C, Osteaux M. Use of diffusion-weighted MR imaging in differential diagnosis be-tw een intracerebral necrotic tumors and cerebral abscesses. A m J Neuroradiol 1999; 20:1252-1257.
11. Ebisu T, Tanaka C, Umeda M, et al. Discrimination of brain abscess from necrotic or cystic tumors by diffusion-weighted echo planar im-aging. Magnetic Resonance Imaging 1996;14:1113-1116.
12. Tsuruda JS, Chew M, Mosely DN. Diffusion-weighted MR imaging of the brain: value of differentiating between extra axial cysts and epider-moid tumors. Am J Neuroradiol 1990;11:925-931.
13. Krabbe K, Gideon P, Wagn P, Hansen U, Thomsen C, Madsen F. MR diffusion imaging of human intracranial tumors. Neuroradiology 1997;39:483-489.
14. Tien RD, Felsberg GJ, Friedman H, Brown M, MacFall J. MR imaging of high-grade cerebral gliomas: value of diffusion-weighted echoplanar pulse sequences. AJR 1994;162:671-677.
15. Schaefer PW, Grant PE, Gonzalez RG. Diffusion-weighted MR Imag-ing of the Brain. Radiology 2000;217:331-345.