REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Effect
of
nitrous
oxide
on
fentanyl
consumption
in
burned
patients
undergoing
dressing
change
Arthur
Halley
Barbosa
do
Vale
∗,
Rogério
Luiz
da
Rocha
Videira,
David
Souza
Gomez,
Maria
José
Carvalho
Carmona,
Sara
Yume
Tsuchie,
Cláudia
Flório,
Matheus
Fachini
Vane,
Irimar
de
Paula
Posso
DisciplineofAnesthesiology,FaculdadedeMedicina,UniversidadedeSãoPaulo,InstitutoCentraldoHCFMUSP,SãoPaulo,SP, Brazil
Received28May2014;accepted3July2014 Availableonline2December2015
KEYWORDS
Pain;
Nitrousoxide; Burns; Debridement
Abstract
Backgroundandobjectives: Thermal injuries and injured areas management are important causesofpaininburnedpatients,requiringthatthesepatientsareconstantlyundergoing gen-eralanesthesiafordressingchange.Nitrousoxide(N2O)hasanalgesicandsedativeproperties; itiseasytouseandwidelyavailable.Thus,theaimofthisstudywastoevaluatetheanalgesic effectofN2Ocombinedwithfentanylinburnedpatientsduringdressingchange.
Method: AfterapprovalbytheinstitutionalEthicsCommittee,15adultburnedpatients requir-ing daily dressing change were evaluated. Patient analgesia was controlled with fentanyl 0.0005%administeredbyintravenouspumpinfusionon-demand.Randomly,inoneofthedaysa mixtureof65%N2Oinoxygen(O2)wasassociatedviamask,withaflowof10L/min(N2Ogroup) andontheotherdayonlyO2underthesameflow(controlgroup).
Results:No significant pain reduction was seen in N2O group compared to control group. VASscorebeforedressingchangewas4.07and3.4,respectively,inN2Oandcontrolgroups. Regarding pain attheend ofthedressing, patients inN2Ogroup reportedpain severity of 2.8;while thecontrolgroup reported2.87. Therewas nosignificant differenceinfentanyl consumptioninbothgroups.
Conclusions: TheassociationofN2Owasnoteffectiveinreducingopioidconsumptionduring dressingchanges.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](A.H.B.doVale). http://dx.doi.org/10.1016/j.bjane.2014.07.016
PALAVRAS-CHAVE
Dor;
Óxidonitroso;
Burns;
Desbridamento
Efeitodoóxidonitrososobreoconsumodefentanilempacientesqueimados submetidosàtrocadecurativo
Resumo
Justificativaeobjetivos: Osferimentostérmicoseamanipulac¸ãodasáreaslesadassãocausas importantesdedorem pacientesvítimasdequeimaduras,necessitandoqueestespacientes sejamconstantementesubmetidosaanestesiasgeraisparaatrocadocurativo.Oóxidonitroso (N2O)tem propriedadesanalgésicas esedativas,sendocapazdefácilutilizac¸ãoedeampla disponibilidade.Comisto, objetivou-seavaliaroefeitoanalgésicodaadministrac¸ão deN2O associadoaofentanilempacientesqueimados,duranteatrocadecurativo.
Método: Apósaprovac¸ãopela comissãodeéticainstitucional, foramavaliados15pacientes adultos,vítimasdequeimadurascomnecessidadedetrocadiáriadecurativo.Aanalgesiado pacientefoicontroladapelousodefentanil0,0005%administradoporbombadeinfusãosob demanda,intravenosa.Demaneiraaleatória,emumdosdiasfoiassociadamisturadeN2Oa 65%emoxigênio(O2)sobmáscaracomfluxode10 L/min(grupoN2O)enooutrodiaapenasO2 sobomesmofluxo(grupocontrole).
Resultados: Nãoseobservoudiminuic¸ãosignificativadadornogrupoN2Oemrelac¸ãoaogrupo controle.AdornaEAVantesdatrocadocurativofoide4,07e3,4;respectivamentenosgrupos N2Oecontrole. Quantoà dorao términoda trocadecurativo, os pacientesdogrupo N2O referiramdorintensidade2,8;enquantonogrupocontrolefoide2,87.Nãohouvediferenc¸a significativadeconsumodefentanilemambososgrupos.
Conclusões:Aassociac¸ãodeN2Onãofoieficaznareduc¸ãonoconsumodeopióidesdurantea trocadecurativos.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Oneofthebiggestproblemsfacedincaringforburnpatients istheneedforfrequentdressings,astheburningisamajor cause of pain even without its manipulation. Therefore, thesepatientsundergogeneralanesthesiaeveryotherday, orevendaily,withlongpost-anesthetic recoveryand pro-longedfasting.1,2Theconsequencesofthisprocessmaybe
malnutritionanddelayed healing.Furthermore, thedrugs usedin general anesthesia often cause nausea and vomi-tinginsensitivepatients.Developmentofdependenceand tolerancetoanestheticdrugsmayalsooccur.3
Thus, thereis interest in studying analgesia and seda-tionmethodsfordressingchangesinburnpatients,allowing rapidinductionandrecoveryofthepatients,withlow inci-denceofsideeffects,atareducedcost,whichcouldbeeasy, efficient,andknownbymedicalprofessionals,enabling bet-terpaincontrolatthemostcriticalmoment.4
Nitrousoxide(N2O)hasanalgesicandsedativeproperties
known for over 150 years and it is still used in gen-eralanesthesia,potentiatingotherintravenousandinhaled anesthetic agents.5,6 Its use in small procedures outside
the operating room is also widespread in the medical and dentalpractice, and it is satisfactory in most cases, with mild and controllable side effects with the agent discontinuation.7---11
Theobjectiveofthisstudywastoevaluatetheanalgesic effectof65%nitrousoxideassociatedwithfentanylinburn patientsduringdressingchanges.
Materials
and
methods
AfterobtainingtheinstitutionalEthicsCommitteeapproval and written informedconsentof all participants, 15burn patients,agedbetween18and60years,ASAIandII, admit-tedtothespecializedunitforburntreatmentattheHospital dasClínicas daFaculdade deMedicinadaUniversidadede SãoPaulo(HCFMUSP),requiringdailydressingchangewere evaluated.
Exclusioncriteria were patients withburns in the air-ways, face or cervical region compromising the proper management and air mask coupling;history of significant side effects (e.g., significant agitation or prolonged nau-sea and vomiting)with N2O inhalation, thosewith severe
or uncontrollablesideeffects,confusedor poorly collabo-rative,withpsychiatricdisordersthatpreventparticipation inthestudy,SpO2<90%,andpregnant.
Patients underwent sedation with 0.0005% fentanyl solution administered intravenously by patient-controlled analgesia (PCA) in loading dose (1mcgkg−1) and, if with
moreseverepain,bolusof30mcgon-demandat5min inter-vals duringdressing change carriedout in thebed by the nursing staffontwooccasions.The use ofPCA pump was previouslyexplainedtothepatient,withthedemandbolus triggeredbythepatientorinvestigatorphysician.Inoneof thedays,amixtureof65%N2Oandoxygen(O2)undermask
withflowrateof10Lmin−1(N
2Ogroup)wasassociated,and
thenextdayonlyO2underthesameflow(controlgroup),
Thestudyparticipantsweremonitoredwithpulse oxime-try, non-invasive pressure, and cardioscope during the procedureandforatleast45subsequentminutes,following possibleadversereactionsandtheirseverity.Patientswere dischargedfromthepost-anestheticcareunitafterreaching anAldrette---Kroulikindex>8.
The following results were recorded for analysis: side effectsduringfollow-up; modalityofanalgesic drugsused for analgesic controlduringhospitalization;dose of intra-venousmorphineinthelast24handthetimesincethelast administration;severityofpainusingavisualanalogscale (VAS)from0to10before,during,andattheendofthe pro-cedure;intravenousfentanylrequired(numberofbolusand totaldose received)recorded in micrograms(mcg) during dressing;patientsatisfactionwiththetechniqueused:very satisfied(VS),satisfied(S),unsatisfied(U),veryunsatisfied (VU), indicating which of the modalities wasmore effec-tiveforpaincontrol:anesthesiausedinthefirstdayofthe study,anesthesiausedintheseconddayofthestudyorany techniqueusedin theprevious dressingchanges;duration oftheprocedure;timeof100%O2administrationafterthe
endoftheprocedure;andtheintervalbetweentheendof theprocedureandobtainingtherecoverycriteriadescribed above.
Dataanalysiswasperformed usingtheStudent’spaired
t-test for comparing total fentanyl consumption between thecontrolandN2Ogroups.VAScomparisonbetween
pro-cedures and time points was performed with analysis of variance for repeated measures and post-test with Bon-ferroni multiple comparisons, considering a p-value<0.05 significant.
Results
Datawere collected betweenJune 2010and March2012. Weevaluated15patients,12menand3women.The aver-ageageandweightwere36.27yearsand66.57kg. Ofthe analyzed patients, 13 wereASA I andtwo wereASA II by systemicarterialhypertension(SAH)andepilepsy,andSAH andChagasdisease.
Regarding burn characteristics, themean body surface area burned (BSAB) was 15.1%, with 20% of participants alsopresentingwiththird-degreeburns.The timeelapsed betweentheburnandthefirsttreatmentusedinthestudy rangedfromthreeto61days,averaging15days.Regarding thetypesofburns,therewerealcohol,petrolorgasburnings (40%);contactwithfireor abrasion(20%);electrical (27%) andscald(13%)(Table1).
Table1 Demographicdata.
Characteristics Mean
Age(years) 36.27
Weight(kg) 66.57
ASAI:II 13:02
BSAB(%) 15.10%
BurnTime(days) 15
ASA,physicalstatusaccordingtotheAmericanSocietyof Anes-thesiologistsclassification;BSAB,bodysurfaceareaburned.
Table2 Morphineconsumptionthedaybeforethedressing
change.
Technique Morphineuse(patients) Meandose(mg)
N2O 9 4.55
Control 7 3.42
0 1 2 3 4 5 6 7 8
Preferred technique
O2
N2O with O2
No distinction between O2 and N2O with O2 Morphine Pacinte
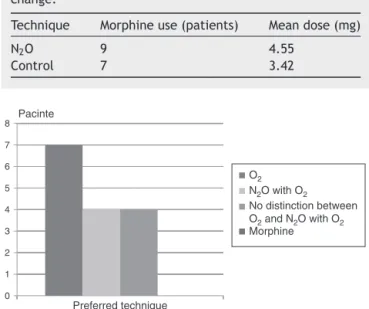
Figure1 Preferenceofpatientsforthetwotechniques
used.
The mean durationof dressing change was 38.8min in N2Ogroupand43.33minincontrolgroup.Fourpatientsin
N2Ogrouphadside effects(3:dizziness; 1:nausea). Only
onecase wasreported in control group (dizziness). None ofthepatientsrequiredadditionalmeasurestocontrolthe symptoms,withspontaneousresolution.
The standard treatment of pain used in the burn wardconsistedofintravenousbolusadministrationof mor-phine,minutesbeforemanipulationofpatientsandincase of severe pain. Seven patients (46.7%) in control group receivedmorphine(meandose of3.42mg)theday before thedressingchange;whileninepatients(60%)inN2Ogroup
receivedameandoseof4.55mgperperson(Table2). Therewasnosignificant decreaseinpainin N2Ogroup
comparedtocontrolgroup.VASpainscorebeforedressing change was 4.07 (p=0.808) and 3.4 (p=0.838), respec-tively.Themostseverepainduringtheprocedurewas6.33 (p=0.532)and6.73(p=0.547).Regardingpainattheendof dressingchange,patientsinN2Ogroupreportedpain
sever-ityof 2.8(p=0.663) andcontrol group of2.87 (p=0.786) (Table3).
Fentanyl consumption in N2O group was 147.43mcg,
whileincontrolgroupitwas157.77mcg.Therewasno sig-nificantdifferenceinconsumption(p=0.46)(Table4).
Regardingtheassessmentoftechniquesusedandpatient satisfaction,seven patients preferredtheuse ofO2 alone
(46.6%), four patients preferred the mixture of N2O and
O2(26.7%),andfourpatientspreferredthetwotechniques
withoutdistinction(26.7%).Noneofthepatientschosethe previoususeofmorphineasafavorite.Amongpatientswho preferredone ofthe techniques, only one chose thefirst daytechnique, while 10chose asfavoritethesecond day technique(Fig.1).
Theanalysisofpatientsatisfactionwiththetechniques usedinthe study showedthat inN2O group fourpatients
Table3 Dressingchangeandpainvariation.
Procedure Time Mean SD Median Minimum Maximum p
Control Before 3.40 3.25 2 0 10 0.838
During 6.73 2.12 7 3 10 0.547
End 2.87 3.04 2 0 10 0.786
N2O Before 4.07 3.13 4 0 10 0.808
During 6.33 2.06 6 3 10 0.532
End 2.80 2.57 2 0 8 0.663
Table4 Fentanylconsumptionduringprocedure.
Variable Group Mean SD Median Minimum Maximum p
Totalfentanil(mcg) Control 157.77 74.25 152 60 335 0.460a
N2O 147.43 49.93 145 55 230
aResultofpairedStudentt-test.
Table5 Patient’ssatisfactionaccordingtogroup.
Technique VS S U VU
N2O 4 11 0 0
Control 6 9 0 0
VS,verysatisfied;S,satisfied;U,unsatisfied;VU,very unsatis-fied.
wassix(VS)andnine(S).Therewasnoreportof dissatisfac-tion(Table5).
Discussion
ThemainfindingofthisstudywasthattheN2Oassociation
wasnoteffectiveinreducingtheopioidconsumptionduring dressingchanges.
The primary effects of N2O are exertedin the central
nervoussystem,withanalgesicactiononsupraspinalGABA inhibition and spinal GABA activation. N2O promotes the
release of endogenous opioids with subsequent release of norepinephrine in the spinal cord and inhibits pain transmission.12 TheuseofN
2Oforpainreliefinprocedures
outside the operating room in the burned pediatric pop-ulation is an issue widely discussed in the literature,8,9,13
incontrasttothepaucityofdataontheadultpopulation. In a survey of more than 7000 cases, Zier et al.14 noted
thathigherconcentrationsofN2O,upto70%,weresafein
severalsmallproceduresperformedinchildren,withhigher incidenceofsideeffectswhenusedformorethan30min. Asystematicreviewinvolving26articlesalsoreportedthe efficacyofusingnitrousoxideforproceduresinchildren.13
In contrast, in this study, the use of N2O 65% offered
no additional benefit in pain control, with no statistical differencewhencomparedwiththecontrolgroup.Apoint tobeconsideredisthatmanyofthestudiesintheliterature useN2Oasatechniqueforpainreliefofprocedureswhose
painstimulusisreduced,suchasperipheralvenousaccess, lumbar puncture, and intramuscular injections.13 When
painstimulusismoresevere, asinthe presentstudy,N2O
showednostatisticaldifferenceofwhenitisnotused. However, the study patients preferred the techniques used (PCA with or without N2O), with 100% satisfaction,
rather than the use of morphine beforedressing change, aswastheserviceroutine.TheuseofPCAinfusionpumpis easy,allowingtheproperuseafterasimplifiedexplanation. It allows the patient to self-administer a predetermined doseoffentanyltotheinfusionlimitssetbythephysician.15
When thereis a request, fentanyl reaches equilibriumat the effector site with an average of 6.4min.14 The
pref-erence forthetechnique usedonthesecond dayby most patients,independentoftheuseoftheN2OandO2mixture
(N2Ogroup)or O2alone(controlgroup),canbeexplained
bythebetteruseofPCA,duetotheexperiencegainedfrom useonthepreviousday.
Ourresults show thatPCA withtarget controlled infu-sion pump with fentanyl may be used as an alternative in sedation ofpatients undergoingburn dressing changes. Theloadingdoseoffentanyl(1mcgkg−1)usedinthestudy
withbolus of30mcgwasinsufficienttoalleviate thepain satisfactorily during dressing change, compared to stud-iesinvolving theuseof otheropioids.16---18 Prakashetal.16
compared four different administration schemes of bolus fentanylon-demand(10,20,30,40mcg)afterloadingdose of1mcgkg−1andreportedbetterpaincontrolinthegroups
receiving30or40mcgoffentanyl(4.7±0.83and3.9±0.63) inVAS,comparedtoreceiving10and20mcg(7.73±1.33and 7.20±1.21).Despitethesimilaritybetweenthedosesused, theworstpaincontrolinthepresentstudymaybeexplained bythedressingchangeintrinsiccharacteristicssuchastime andtechniqueusedbythepractitioners,inadditiontopain intensityfluctuationsthroughoutthedayanditssubjective interpretationbyburnpatients.
subjective.The interactionwithpatients,eitherwith ver-balor tactilestimulation, performedby doctorsornurses duringtheprocedureistheconductadvocatedbymost stud-ies to assess the level of consciousness.19 The technique
safetywasobserved witha sedation inwhich the patient remainedconscious,collaborative,usingthePCAonhisown, andremainedwithhisvitalsignsstable.
Thestudyresultsshowthatpatient-controlledanalgesia at bedsideassociated withtheuseof N2Oduring dressing
change in burn patients does not benefit pain control or decreases fentanyl consumption, although this technique is safe, affordable, resource-sparing,and associated with greaterpatientsatisfaction,regardingtheuseofmorphine alone.However,morestudiesareneededtoassessthemost appropriatedoseofmedicationsusedinalargerpopulation simpletoassessthevalidityandthestatisticalsignificance ofthefindings.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Berge TI.Acceptance and side effects ofnitrous oxide oxy-gensedationfororalsurgicalprocedures.ActaOdontolScand. 1999;57:201---6.
2.Prakash S, Tazeen F, Mridula P. Patient-controlled analge-sia with fentanyl for burn dressing changes. Anesth Analg. 2004;99:552---5.
3.CasteraL,NegreI,SamiiK,etal.Patient-administerednitrous oxide/oxygeninhalationprovidessafeandeffectiveanalgesia forpercutaneousliverbiopsy:arandomizedplacebo-controlled trial.AmJGastroenterol.2001;96:1553---7.
4.BadenJM,RiceSA.Metabolismandtoxicity.In:MillerRD,editor. Anesthesia,4thed.NewYork:ChurchillLivingstone;1994. p. 157---83.
5.VideiraRLR,AulerJOCJr.TratadodeAnestesiologia.SAESP,7th ed.SãoPaulo:Atheneu;2011.p.2157---66.
6.GirtlerR,GustorffB.Painmanagementinburninjuries. Anaes-thesist.2011;60:243---50.
7.Fink DA.Nitrous oxideanalgesia. In: EgerEI,editor. Nitrous oxide/N2ONewYork:Elsevier;1985.p.41---55.
8.Hurford WE, Bailin MT, Davison JK, et al. Clinical anesthe-siaproceduresoftheMassachusettsGeneralHospital,5thed. Philadelphia:Lippincott-Raven;1997.p.174---5.
9.LuhmannJD,KennedyRM,PorterFL,etal.Arandomized clin-icaltrialofcontinuous-flownitrousoxideandmidazolam for sedationofyoungchildrenduringlacerationrepair.AnnEmerg Med.2001;37:20---7.
10.AnnequinD,CarbajalR,ChauvinP,etal.Fixed50%nitrousoxide mixture for painful procedures:a French survey. Pediatrics. 2000;105:47---57.
11.KeidanI, ZaslanskyR, YusimY, etal. Continuous flow 50:50 nitrous oxide:oxygen is effective for relief of procedural pain in the pediatric emergency department. Accute Pain. 2003;5:25---30.
12.SimKM,HwangNC,ChanYW,SeahCS.Useofpatient-controlled analgesia with alfentanil for burns dressing procedures: a preliminary report of five patients. Burns. 1996;22: 238---41.
13.CorboyJM.Nitrousoxideanalgesiaforoutpatientsurgery.JAm IntraoculImplantSoc.1984;10:232---4.
14.Gallagher G, Rae CP,Kenny GN, etal. The useof a target-controlled infusion of alfentanil to provide analgesia for burn dressing changes: a dose finding study. Anaesthesia. 2000;55:1159---63.
15.Coimbra C, Choinière M,Hemmerling TM. Patient-controlled sedationusingpropofolfordressingchangesinburnpatients:a dose-findingstudy.AnesthAnalg.2003;97:839---42.
16.Sanders RD,Weimann J, MazeM. Biologiceffects of nitrous oxide: a mechanistic and toxicologic review. Anesthesiology. 2008;109:707---22.
17.PedersenRS,BayatA,SteenNP,etal.Nitrousoxideprovides safeandeffectiveanalgesiaforminorpaediatricprocedures,a systematicreview.DanMedJ.2013;60:A4627.
18.ZierJL, LiuM.Safetyofhigh-concentrationnitrousoxide by nasalmaskforpediatricproceduralsedation:experiencewith 7802cases.PediatrEmergCare.2011;27:1107---12.