RevBrasAnestesiol.2015;65(3):213---216
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiology www.sba.com.brSCIENTIFIC
ARTICLE
Evaluation
of
brachial
plexus
fascicles
involvement
on
infraclavicular
block:
unfixed
cadaver
study
Luiz
Carlos
Buarque
de
Gusmão
a,b,
Jacqueline
Silva
Brito
Lima
a,
Jeane
da
Rosa
Oiticica
Ramalho
a,
Amanda
Lira
dos
Santos
Leite
a,∗,
Alberson
Maylson
Ramos
da
Silva
aaUniversidadeFederaldeAlagoas(UFAL),Maceió,AL,Brazil
bColégioBrasileirodeCirurgiões,Maceió,AL,Brazil
Received24March2014;accepted2June2014 Availableonline17February2015
KEYWORDS
Regionalanesthesia; Brachialplexus; Blockinfraclavicular
Abstract
Backgroundandobjectives: Thisstudyshowshowthediffusionoftheanestheticintothesheath occursthroughtheaxillaryinfraclavicularspaceandhenceprovestheefficacyoftheanesthetic blockofthebrachialplexus,andmaytherebyallowaconsolidationofthispathway,withfewer complications,previouslyattachedtotheanesthesia.
Materialsandmethods: 33armpitsofadultcadaverswereanalyzedandunfixed.Weinjected a solutionofneoprene with latexdye intheinfraclavicularspace, basedonthe technique advocatedbyGusmãoetal.,andputthecorpsesinrefrigeratorsforthreeweeks.Subsequently, thespecimenswerethawedanddissected,exposingtheaxillarysheathalongitsentirelength.
Resultsanddiscussion:Wasdemonstratedinvolvementofallfasciculusoftheplexusin51.46%. Inpartialinvolvementwas30.30%,18.24%ofcasestheacrylicwaslocatedoutsidetheauxiliary sheathinvolvingnoissue.
Conclusions: Theresultsallowustoestablishtheinfraclavicularasaneffectiveandeasywayto accessplexusbrachial,becausethesolutioninvolvedthefasciclesin81.76%partiallyortotally, whenitwasinjectedinsidetheaxillarysheath.Webelievethatonlytheuseofthispathway accessinpracticeitmaydemonstratetheefficiency.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](A.L.d.S.Leite). http://dx.doi.org/10.1016/j.bjane.2014.06.010
214 L.C.B.deGusmãoetal.
PALAVRAS-CHAVE
Anestesiaregional; Plexobraquial; Bloqueio infraclavicular
Avaliac¸ãodoenvolvimentodosfascículosdoplexobraquialnobloqueioporvia
infraclavicular:estudoemcadáveresnãofixados
Resumo
Justificativaeobjetivos: Procuramosdemonstrarcomoocorreadifusãodoanestésicono inte-rior da bainha axilar,quando se utilizao bloqueio porvia infraclavicular,através da fossa infraclaviculare,consequentemente,provaraeficáciadessavia,podendo,comisso,permitir umaconsolidac¸ãodautilizac¸ãodesseacesso,comreduc¸ãodascomplicac¸ões.
Materiasemétodo:Foram utilizadas33 axilas de cadáveres adultos não fixados. Injetamos umasoluc¸ãodeneoprene látexcomcorantenafossainfraclavicular,baseando-senatécnica preconizada porGusmãoe col,e colocamosos cadáveresem geladeiraspor trêssemanas. Posteriormente,aspec¸asforamdescongeladasedissecadas,expondoabainhaaxilaremtoda suaextensão.
Resultadosediscussão: Foi demonstrado envolvimento de todos os fascículos do plexo em 51,46%.Em30,30%houveenvolvimentoparcial,eem18,24%doscasosoacrílicofoilocalizado foradabainhaaxilar,nãoenvolvendonenhumfascículo.
Conclusões:Osdadosobtidospermitemestabeleceraviainfraclavicularcomoumaviaeficaze defácilacessoaoplexobraquial,vistoqueasoluc¸ãoinjetadaenvolveuosfascículosem81,76% parcialmente outotalmente, quandoerainjetadadentrodabainhaaxilar.Acreditamosque apenasautilizac¸ãodestaviadeacessonapráticapoderádemonstraraeficiênciadamesma. ©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Overtheyears,brachialplexusblockadebysupraclavicular andaxillaryrouteshaspresentedanumberofcomplications and failures, bringing back the use of the infraclavicular route.1
The infraclavicular brachial plexus block was initially advocatedbyHirschel2in 1913.In1917, Bazy3 introduced
aneedlebelowtheclavicle,ina‘‘anestheticline’’drawn betweentheanteriortubercleofthesixthcervicalvertebra andthe coracoid process.In 1918, Babitsky4 injected the
anestheticbetweentheangleformedbythe2ndribandthe clavicle.
In 1922, Labat5, after injecting the anesthetic at the
samepoint recommendedbyBazy,flexed thearm toward thechestandperformedanotherinjectionofthesame solu-tion.
In1924,Balog6modifiedBazy’stechnique,buttheneedle
wasintroducedtowardtheribcage,untilittouchesthe sec-ondrib,andheretreatedtheneedlealittleanddeposited theanesthetic.
In1973,Rajetal.7introducedtheneedleatamidpoint
oftheclavicle,turningittothesidetopreventpuncturing thechestwall.
Sims8,1977,modifiedthetechniquebyRajetal.usinga
standard3.8cmneedlewhichdirecteddownward,outward, andbackwardreachedthebrachialplexus2---3cmafter hav-ingpassed theskin.Heemphasizesthatitisarapid,easy andconsistentaccessrouteforblockadeperformance.
Whiffler9,1981,drewalinebetweenthesubclavianand
axillaryarteries,andthe puncturewasmadeat thepoint that this line crossed the coracoid process and reported successin92.5%ofcasesandarterialpuncturein50%.
In1995, Kilkaetal.10 reportedthat theinfraclavicular
brachialplexusblockhavelowerriskofpneumothoraxand lowincidenceofphrenicnerveblock.
In2001, Imbelloni etal.1 determine thatthe injection
shouldbeatapoint1.5cmbelowthesiteofunionbetween thelateralthirdandthemedialtwo-thirdsoftheclavicle, succeedingin94%ofcases.
Althoughtherewerefewercomplications,casesof vascu-larandchestwallpunctureswithconsequentpneumothorax werestillreported.11
In2002,Gusmãoetal.11usedonehundredfixedcadavers
and performed infraclavicularfossa dissection,which was present in 96% of cases, determiningthat brachialplexus block by thisroute should beperformed after findingthe angleformedbythejunctionoftheanteriormarginofthe deltoidmuscleandthe clavicle,drawabisectorfromthe angle to the fossa center, measuring about 2.21cm, and entertheneedleperpendiculartotheskinatthissitewitha depthof3.0---3.5cm,piercingtheaxillarysheathand reach-ing the brachial plexus, which are located at this level, laterallytotheaxillaryvessels.
Verifyingthat brachialplexus in mostcases lieswithin theinfraclavicularfossaandthattheblockadebythisaccess routereachesthebrachialplexusfasciculiwithfewfailures andwithoutthecomplicationsdescribedintheinterscalene, supraclavicular,andaxillarytechniques, itremainedtobe demonstrate how the anesthetic spread behavesby using theabovedescribedroute.
Materials
and
methods
Complying with what determines the Federal Law N◦
Evaluationofbrachialplexusfasciculiinvolvementininfraclavicularblock 215
approval, 33 axillary regions of unfixed adult cadaversof bothsexesdonatedbytheInstitutoMédicoLegalEstáciode Limatothe MedicalScholloftheUniversidadeFederal de Alagoaswereusedinthisstudy.
The infraclavicular route wasused, through the infra-clavicular fossa, as stated by Gusmão et al.11 Instead of
theanesthetic,weusedadilutesolutionofneoprenelatex withdye (30Ml). After injection, the bodies were placed intotherefrigerator,wheretheyremainedforaboutthree weeks.After theneoprenelatex solidification period,the bodieswerethawed.Subsequently,alargeincisionfromthe necktothearmpitwasperformed,exposingthefullextent of theaxillary sheath,aswell asitscontent. Suchaccess hasallowedustoobserveandanalyzetheinjectedsolution diffusionalong theaxillary sheath,aswellasthebrachial plexusfasciculiinvolved.
Results
Thefindingsinthe33injectedaxillaewereasfollows:
--- In51.46%ofcases(17axillae)therewas100%involvement ofbrachialplexusfasciculi(Figs.1and2).
--- In30.30% of cases(10 axillae),the anestheticpartially involvedthebrachialplexusfasciculiasfollows:inthree axillae there was diffusion only of the posterior and medialfasciculi; inthree axillae,the solutiononly cir-cledthelateralfasciculus;intwoaxillae,onlythelateral andposteriorfasciculiwereinvolved;intwoaxillae,only theposteriorfasciculuswasbathedinsolution.
Figure1 Totalinvolvementofthebrachialplexus(yellow). V,axillaryvein;fl,lateralfasciculus;fm,medialfasciculus.
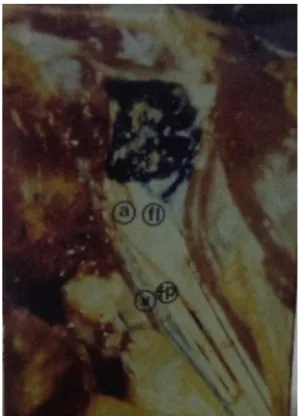
Figure2 Totalinvolvementofbrachialplexusfasciculi(blue). V,axillaryvein;a,axillaryartery;fl,lateralfasciculus;fp, pos-teriorfasciculus.
In18.24%ofcases(sixaxillae),almostallofthesolidified solutionwaslocatedoutsidetheaxillarysheath,andwhen theacrylicwasintothesheath,nofasciculuswasinvolved.
Discussion
Sincethe 70s, studies have demonstrated the superiority ofthe infraclavicular brachialplexus block. Raj7 has
suc-cessfulinblockingallbrachialplexusinmostcases(95%), arguingthatthisapproachisquitesafefor brachialplexus block,allowingtheadequateanestheticblockoftheupper limb.
The infraclavicular anesthetic blockade techniques reportedintheliteratureuseseveralpointsbelowthe clavi-cle,whichsometimesareoverthepectoralismajormuscle, sometimes beside the coracoid process, or over the infr-aclavicularfossa.11 Inseveralrecommendedaccessroutes
theanestheticinjectionsitewasnotalwayswithinthe infr-aclavicularfossaandthereisnoinformationaboutthefossa sitethroughwhichthebrachialplexusandaxillary vessels pass.TheaccessrouteproposedbyGusmãoetal.11 shows
that,inmostcases,thebrachialplexusfasciculiarelocated inthisfossaand,forsecurityintheimplementationofthe blockadebytheanesthesiologist,itwasgiventhe informa-tionnotonlyofthedepthwheretheplexusislocated,but alsoitslocationwithintheinfraclavicular fossa,fromthe angleformedbythedeltoidmuscleandtheclavicle.
216 L.C.B.deGusmãoetal.
Thepartialinvolvementoffasciculi,andcasesinwhich thesolutionwaslocatedoutsidethesheath,wasinpartdue tothe fact that puncture was not performed by a single investigator,andfailuremayhaveoccurredinthedepthof needleinsertion.
Wearguethat thesolutionlocatedoutside theaxillary sheathmayhave resultedfromleakagebecause,although some authors believe that this sheath forms a enclosed space,12 dissections in laboratory showed that the
solu-tion injected into it could be leaked through the holes drilled by vascular and nervous structures transfixing the sheath.
Basedontheresultsandusingtheaccessrouteproposed byGusmãoetal.,11 weobservedthatitallowseasyaccess
to brachial plexus, as the injected solution involved the fasciculiin 81.76% of cases, with51.46% totallyenvolved and30.30%partiallyenvolvedwhenitwasinjectedintothe axillarysheath.
Webelievethattheuseofthisroute,performedby anes-thesiologists,yieldsthesameresultsreportedbyImbelloni etal.1
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ImbelloniLE,BeatoL,GouveiaMA.BloqueiodoPlexoBraquial porviainfraclavicular:Abordagem Ântero-Posterior.RevBras Anestesiol.2001;51:235---43.
2.Hisrchel G. Handbook of local anesthesia. Wiesbaden: JF Bergman;1913.
3.BazyYL.L‘anesthesiaregionale.Paris:GDoin;1917.
4.BabitszkyP.Anewwayofanesthesiathebrachialplexus. Zen-tralblFChir.1918;45:215---7.
5.LabatG.Regionalanesthesia.Philadelphia:WBSaunders;1922. 6.BalogA.Conductionanesthesiaoftheinfraclavicularportionof
thebrachialplexus.ZentralblChir.1924;51:1563---4.
7.RajPP,MontgomerySJ,NettlesD,etal.Infraclavicularbrachial plexusblock---anewapproach.AnesthAnalg.1973;52:897---904. 8.SimsJK.Modificationoflandmarksforinfraclavicularapproach
tobrachialplexusblock.AnesthAnalg.1977;56:554---5. 9.WhifflerK.Coracoidblock:asafeandeasytechnique.Anesth
Analg.1981;53:845---8.
10.Kilka HG, Geiger P, Mehrkens HH. Infraclavicular vertical brachialplexusblockade.Anewmethodforanesthesiaofthe upperextremity.Ananatomicalandclinicalstudy.Anaesthesist. 1995;44:339---44.
11.GusmãoLCB,LimaJSB,PratesJC.Basesanatômicasparao blo-queioanestésicodoplexobraquialporviainfraclavicular.Rev BrasAnestesiol.2002;52:348---53.