REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Minimum
effective
concentration
of
bupivacaine
for
axillary
brachial
plexus
block
guided
by
ultrasound
夽
Alexandre
Takeda,
Leonardo
Henrique
Cunha
Ferraro
∗,
André
Hosoi
Rezende,
Eduardo
Jun
Sadatsune,
Luiz
Fernando
dos
Reis
Falcão,
Maria
Angela
Tardelli
DepartmentofAnesthesiology,PainandIntensiveCare,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo (UNIFESP),SãoPaulo,SP,Brazil
Received21September2013;accepted26November2013 Availableonline16February2015
KEYWORDS
Regionalanesthesia; Brachialplexusblock; Bupivacaine;
Ultrasound; Axillaryblock; Minimumeffective concentration
Abstract
Introduction:The useofultrasoundinregionalanesthesiaallowsreducingthedoseoflocal
anestheticusedforperipheralnerveblock.Thepresentstudywasperformedtodeterminethe
minimumeffectiveconcentration(MEC90)ofbupivacaineforaxillarybrachialplexusblock.
Methods:Patientsundergoinghandsurgerywererecruited.ToestimatetheMEC90,a
sequen-tialup-downbiasedcoinmethodofallocation wasused.Thebupivacainedosewas5mLfor
eachnerve(radial,ulnar,median,andmusculocutaneous).Theinitialconcentrationwas0.35%.
Thisconcentrationwaschangedby0.05%dependingonthepreviousblock;ablockadefailure
resultedinincreasedconcentrationforthenextpatient;incaseofsuccess,thenextpatient
couldreceiveorreduction(0.1probability)orthesameconcentration(0.9probability).
Sur-gical anesthesiawas defined as drivingforce≤2according tothe modified Bromage scale,
lackofthermalsensitivityandresponsetopinprick.Postoperativeanalgesiawasassessedin
therecoveryroomwithnumericpainscaleandtheamountofdrugsusedwithin4hafterthe
blockade.
Results:MEC90 was 0.241% [R2: 0.978, confidence interval: 0.20---0.34%]. No patient, with
successfulblock,reportedpainafter4h.
Conclusion: Thisstudydemonstratedthatultrasoundguidedaxillarybrachialplexusblockcan
be performedwith theuse oflowconcentration oflocal anesthetics,increasing the safety
of theprocedure. Further studies shouldbe conducted to assess blockade duration atlow
concentrations.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights
reserved.
夽 EthicalInstitutionComitteeRegister:0482/11.
ClinicalTrials.govRegister:NCT01838928.
∗Correspondingauthor.
E-mail:[email protected](L.H.C.Ferraro).
http://dx.doi.org/10.1016/j.bjane.2013.11.007
PALAVRAS-CHAVE
Anestesiaregional; Bloqueiodoplexo braquial;
Bupivacaina; Ultrassom; Bloqueioaxilar; Concentrac¸ãomínima efetiva
Concentrac¸ãomínimaefetivadebupivacaínaparaobloqueiodoplexobraquialvia axilarguiadoporultrassom
Resumo
Introduc¸ão:Ousodoultrassomnaanestesiaregionalpermiteareduc¸ãodadosedeanestésico
localutilizadaparaobloqueiodenervosperiféricos.Opresenteestudofoiconduzidocomo
objetivodedeterminaraconcentrac¸ãomínimaefetiva(CME90)debupivacaínaparaobloqueio
doplexobraquialviaaxilar(BPVA).
Métodos: Pacientessubmetidosacirurgiasdamãoforamrecrutados.Foiusadoummétodode
alocac¸ão‘‘biasedcoin’’seqüencial‘‘up-down’’paraestimaraCME90.Adosedebupivacaína
foide5mLparacadanervo(radial,ulnar,medianoemusculocutâneo).Aconcentrac¸ãoinicial
deera0,35%.Essaconcentrac¸ãoeraalteradaem0,05%dependendodobloqueioanterior:a
falhadobloqueioresultavaemaumentodaconcentrac¸ãoparaopróximopaciente;nocaso
desucesso,opróximopacientepoderiareceberoureduc¸ão(probabilidadede0,1)oumesma
concentrac¸ão(probabilidade0,9). Aanestesia cirúrgicafoidefinidacomo forc¸amotora ≤2
segundoaescaladeBromagemodificada,ausênciadesensibilidadetérmicaederespostaao
pinprick.Aanalgesiapós-operatóriafoiverificadanasaladerecuperac¸ãoanestésicacomescala
numéricadedoreaquantidadedeanalgésicosutilizadosaté4horasapósobloqueio.
Resultados: A CME90foide 0,241%[R2: 0,978,Intervalo deConfianc¸a:0,20%---0,34%]. Além
disso,nenhumpacientecomsucessodobloqueioapresentoudorapós4horas.
Conclusão:Este estudo demonstrou que pode-se realizar o BPVA guiado por ultrassom
utilizando-sebaixasconcentrac¸ões deanestésicolocal,aumentandoaseguranc¸ado
proced-imento.Novosestudosdevemserrealizadosparaavaliaradurac¸ãodebloqueioscombaixas
concentrac¸ões.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos
direitosreservados.
Introduction
A successful peripheral nerve block depends on the cor-rectidentification ofnervousstructures andtheinjection ofasuitabledoseoflocalanestheticarounditinorderto obtainacompleteimpregnationofallthenervesinvolvedin thesurgery.Foraxillarybrachialplexusblockade(ABPB),in whichthefailuresaretypicallyattributedtoimproper nee-dleplacement or septation of the brachial plexus sheath inaxillary region,1,2 volumes upto 80mL have been used
to increase the success rate.3 However, the use of large
amounts of local anesthetic increases the chance of
sys-temictoxicity,whichisthemajorcomplicationofregional
anesthesia. Although the incidenceof systemic toxicityis
less than 0.2%, this complication is difficult to treat and
potentiallyfatal.4,5
The introduction ofultrasound intoclinical practiceof
regionalanesthesiamadeitpossibletovisualizethenerve
structures, allowing greater accuracy in the
administra-tion of local anesthetics. The minimum effective volume
oflocalanestheticforblockingsomeperipheralnerveshad
been investigated, andstudies have shown that effective
blockades may be achieved with small volumes of
anes-thetic,whichreducesthelikelihoodofsystemictoxicity.6---11
However,theclinical applicabilityof lowvolumesandthe
limitationofidentifyingintraneuralinjectionsbyultrasound
havebeenquestioned.12
Reducing the local anesthetic concentration may limit
thetotal dose administered without changing the volume
injected. However, the minimum concentration of local
anesthetictoobtainasafeABPBwithoutcompromisingthe
blockadequalityandeffectivenesshasnotbeenestablished
yet.
The aim of this study was to calculate the
mini-mumeffectiveconcentrationof20mLbupivacainewithout
epinephrine, which reached surgical anesthesia dose for
axillarybrachialplexusblockguidedbyultrasoundforhand
surgeryin90%ofpatients(MEC90).
Material
and
methods
Thepresentstudyusedastep-up/step-downmodelto
deter-minetheMEC90ofbupivacaineinultrasoundguidedABPB.
ThisprotocolwasapprovedbytheEthicsResearch
Com-mitteeofourinstitution(Ref0482/11)andregisteredinthe
Clinical-Trials.gov (protocol NCT01838928). Patients aged
between18and65years,withindicationforanesthesiaand
analgesiabrachialplexusblock,undergoingelectivesurgery
ofthehandwithlessthan2hduration,physicalstatusASA
I,IIorIIIaccordingtotheAmericanSocietyof
Anesthesiol-ogists,andbodymassindex(BMI)<35kgm−2wereincluded
inthestudy betweentheyears2011 and2012, after
sign-ingtheinformedconsentform.Patientswithdisordersthat
preventedtheassessmentofmotorsensitivefunction,
cog-nitiveimpairmentoractivepsychiatriccondition,infection
attheblockadepuncturesite,bleedingdisordersorhistory
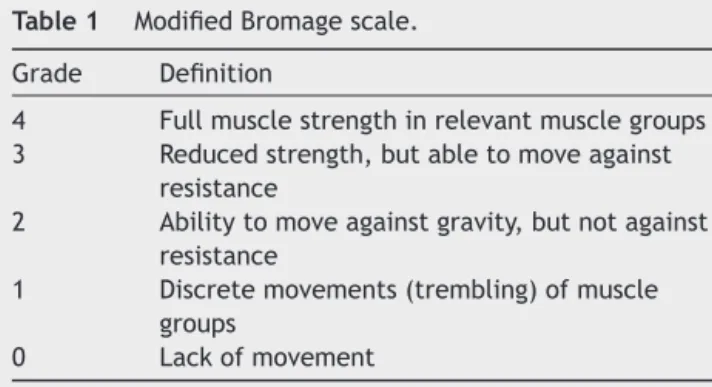
Table1 ModifiedBromagescale.
Grade Definition
4 Fullmusclestrengthinrelevantmusclegroups
3 Reducedstrength,butabletomoveagainst
resistance
2 Abilitytomoveagainstgravity,butnotagainst
resistance
1 Discretemovements(trembling)ofmuscle
groups
0 Lackofmovement
After inclusion in the study, demographic data of all patientswererecorded. Then,routinemonitoring for sur-gicalprocedurewasperformedwithECG,noninvasiveblood pressure,andpulseoximetry.Peripheralvenousaccesswas obtainedintheupperlimbcontralateraltothesurgeryfor infusionofcrystalloidsolutionandsedationwithmidazolam (0.03mgkg−1).
Axillary brachial plexus block wasperformed with the ultrasound M-Turbo® guidance and 13---6MHz linear
trans-ducer(SonoSite,Bothell,WA,USA)andaperipheralnerve stimulatorStimuplex®DIGRC(B.Braun,Melsung,Germany)
withthepatientinsupineposition.Skinantisepsiswas per-formedwithchlorhexidine;transducerwasprotectedwith sterile plastic; and puncture site was infiltrated with 1% lidocaine (2mL).After the brachialplexus nerves’ visual-ization by ultrasoundthe puncture wasperformed with a 22G needle for electrostimulation 50mm AEQ 2250 (BMD Group,Venice,Italy).Neurostimulatorwasusedtoconfirm theidentificationofthefournerves(median,ulnar,radial, musculocutaneous)separately.Adose of5mLbupivacaine withoutepinephrinewasslowlyinjectedaroundeachnerve visualizedwithultrasound,completingatotalof20mL.The 5mLdose wasdefinedbasedoncurrent regional anesthe-siaprotocolsofourinstitution.Iftherewasanyresistance tothesolutioninjection,thepatientcomplainedofsevere pain,or anincreaseinnervediameterwasvisualized,and theneedlewasrepositioned.Thelocalanestheticdispersion wascarefullymonitoredbytheimagesoitwentaroundthe nerveperimeter.
The end of the local anesthetic solutioninjection was consideredthetimezerotoassesstheblockade effective-ness.An anesthesiologist who wasnot present during the injectionandwasunawareoftheanestheticconcentration assessedthemotor,thermal,andsensoryblocks.This assess-mentoccurredevery5min,fromtimezerountiltheblock wasconsideredeffective,butlimitedto30min.Afterthat time,iftheblockwasnotappropriate,acomplementation wasperformed.
ModifiedBromage scale6,11 (Table1)wasusedtoassess
motorfunction.Thefollowingmuscleswereevaluated:
fin-gerflexors(mediannerve),fingerextensors(radialnerve),
fingeradductors(ulnarnerve)andelbowflexion
(musculo-cutaneousnerve).The scorewasobtainedfor eachof the
fournerves.
Thermal sensation was assessed with gauze and
alco-holandpainsensitivity withthepinpricktest witha23G
needle. Both assessments were performed separately for
eachnerveandsensation,andthefollowinglocationswere
used:hypothenareminence(ulnarnerve),thenareminence
(mediannerve),dorsumofhand(radialnerve),andlateral
aspectoftheforearm(musculocutaneousnerve).
Latencywasdefinedastheperiodbetweentimezeroand
thetimethatsurgicalanesthesiawasobtained.
Surgical anesthesia was considered effective if motor
scalewas lessthan or equal to2,ifthere wasnofeeling
ofpain andcold for all nerves,and iftherewas noneed
for supplementation (local or general anesthesia) during
surgery.Patientswhoexhibitedanydegreeofblockade
fail-urereceivedsupplementationwithnervelocalanesthesia,
distaltotheaxillaandguidedbyultrasound,orconversion
togeneralanesthesia.
Allpatientsreceivedsubcutaneousinjectionof2%
lido-cainewithepinephrine(3mL)tocomplementtheintercostal
nerveblock,duetotheuseofpneumatictourniquetinthe
middlethird ofthe arm. Duringsurgery, propofolinfusion
(25---40mcgkg−1min−1)wasusedforsedationuntilRamsay
score=3.
After surgery, patients were admitted to the
post-anesthesia care unit and remained monitored until they
reachedthe conditionsof discharge asoutpatients.While
remaininginthePACU,postoperativeanalgesiawasassessed
throughanumerical painscale (0=no painand10=worst
paineverexperienced bythe patient)andthe total
anal-gesicrequestedbythepatientupto4haftertheABPBwas
quantified.
Statisticalanalysis
Inthisstudy,theprimaryobjectivewastoestimatethe
min-imumeffectiveconcentrationofa5mLbupivacainesolution
pernerve(totalof20mL)foraxillarybrachialplexus
block-adeguided by ultrasound.For this,an allocationmethod
of biased coin up-down sequence was used to estimate
theMEC90.13 Thelocalanestheticinitialconcentrationwas
0.35%.This dose waschosen basedonthe clinical
experi-enceof our service and also on statistical simulations in
variousdoses. Each subsequent dose was basedon
previ-ousdose.ThesuccessorfailureoftheABPBdeterminedthe
decreaseorincrease oflocalanesthetic concentrationfor
thenextpatient,respectively.Afteraneffectiveblock,the
nextpatient wasrandomizedwith aprobability of 0.1 to
receivethenextlowerdose andrandomizedwitha
proba-bilityof0.9toreceive thesamedose.These probabilities
werecalculatedasfollows:
Probability for dose reduction (P1): P1=(desired
MEC−1)×(desiredMEC)−1
Probabilityfordosemaintenance(P2):P1=1−P1
Inthisstudy,wechosetoperformthecalculationto
esti-matetheminimumeffectiveconcentrationin90%ofcases,
thus:
--- P1=(1−0.9)/0.9=≈0.1
--- P2=1−P1=≈0.9
Thesequencewasexaminedusinglogisticregressionto
calculatethe minimumeffectiveconcentration for90% of
For sample size calculation, simulations were
per-formedassumingafixedbiasedcoinmodelandaminimum
number of positive responses. A significance level of 5%
(˛=0.05) was considered. A sample size of at least 46
patients was selected after testing with a variety of
settings,each withsimulationsof bothresponsesand
cor-responding doses selected by the sequential allocation
methoddescribed above,and starting withvarious initial
doses.
Nonparametric data are presented as medians and
quartiles (P25---P75). Categorical data are presented as
absolute and relativefrequencies. Calculations were
per-formed using Microsoft Excel for WindowsTM (Microsoft
Corp., Redmond, WA, USA), GraphPad PrismTM for
Win-dows (GraphPad Software Inc.,San Diego, CA, USA), and
IBMSPSS StatisticsTM 20.0 for Mac (SPSSInc.,Chicago, IL,
USA).
Results
Forty-six patients were enrolled and their demographic
and surgical characteristics are shown in Tables 2 and 3,
respectively.Nopatientwhomettheinclusioncriteriawas
excludedfromthestudy.
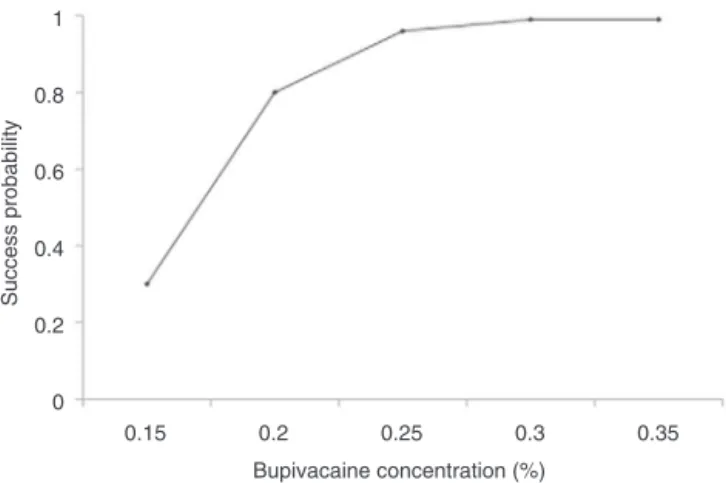
ThepresentstudyshowedthattheMEC90foratotalof
20mLsolutionofbupivacainewithoutepinephrinefor
axil-larybrachialplexusblockguidedbyultrasoundwas0.241%
[correlationcoefficient---R2:0.978;confidenceinterval(CI):
0.20---0.34%].
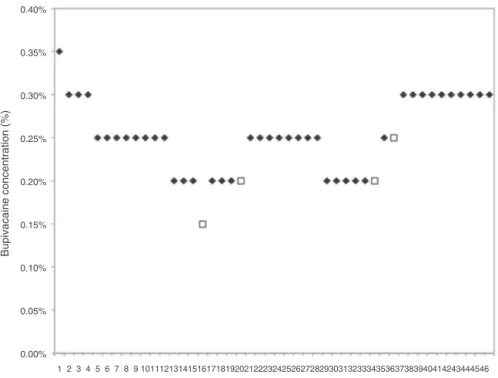
According to the results shown in Fig. 1, there is a
strong positive correlation between the success
proba-bility and observed concentrations. Fig. 2 illustrates the
Table2 Demographiccharacteristicsofpatients.
Age(years)a 35.5(28---44.5)
Sex(M/F) 32/14
ASA
I 31(67.4%)
II 15(22.6%)
BMI(kgm−2) 24.9(22.5---26.8)
BMI,bodymassindex.
a Datapresentedasmedian(quartiles).
Table3 Distributionofsurgicalprocedures(n=46).
Metacarpalfracture 17
Extensortendoninjury 6
Excisionofbonetumor 5
Flexortendoninjury 5
Phalanxpseudoarthrosis 3
Synovectomy 3
Dupuytren 3
Scaphoidfracture 3
Synthesismaterialremoval 1
Duration,min(P25---P75)a 55(40---78,75)
a Datapresentedasmedian(quartiles).
correlationbetweensuccessprobabilityandobserved
con-centrations.
Considering all study patients, the mean latency
time was 15 (10---20)min. Considering only patients who
Success
123456789 10111213141516171819202122232425262728293031323334353637383940414243444546
0.00% 0.05% 0.10% 0.15% 0.20% 0.25% 0.30% 0.35% 0.40%
Failure Sequence of patients
Bupivacaine concentration (%)
0.15 0 0.2 0.4 0.6 0.8 1
0.2
0.25
Bupivacaine concentration (%)
Success probability
0.3
0.35
Figure 2 Correlation between concentration and success probabilities.
Table4 Latencyfordifferentconcentrations.
Dose Numberof
blocks/successful
Latency(min)a
(P25---P75)
0.15% 0/1
---0.20% 11/13 25(25---30) 0.25% 17/18 20(15---22.15) 0.30% 13/13 15(10---16.15)
0.35% 1/1 5
a Datapresentedasmedian(quartiles).
received blockades with 0.25% concentration (the
near-est MEC90 concentration), the mean latency time was
20 (15---22.15)min. Mean latency times for each assessed
concentrationaresummarizedinTable4.Blockadeduration
wasnotdeterminedinthisstudy.
There was100% blockadefailurewiththeuseof0.15%
bupivacaine. However, all blockades performed with a
concentrationequaltoorgreaterthan0.30weresuccessful
(Fig.1).
Nopatientincluded in theprotocolshowedabsenceof
specificresponsetoneurostimulatororintraoperativepain.
Allpatientsconsideredasfailuremaintainedmediannerve
motor function, and two patients also maintained radial
nervemotor function.The lack of thermal sensitivitywas
alsoobserved in thesepatients, although maintaining the
motorfunction.
Two surgical procedures exceeded the expected
dura-tion of surgery and lasted more than 120min, without
complicationsforthepatientorneedforsupplemental
anes-thesia.
Allsurgicalproceduresforwhichpatientsreceived
suc-cessful blocks were performed uneventfully, and there
was no need for local and systemic anesthetic
supple-mentation Moreover, all patients reported no pain 4h
after the ABPB (EAV=0). There were no complications,
such as vascular puncture or local anesthetic
intoxica-tion,duringthestudy.Allpatientsweredischargedonthe
same day of the surgery, without the need for hospital
readmission.
Discussion
Peripheral nerve block success is based on the accuracy
withwhichthenervesarelocatedandimpregnatedbythe
anesthetic.However,otherimportant factorsaffecting its
success rate and quality are the concentration and
vol-umeof anesthetic injected nearthe nerves.14 The use of
ultrasound has introduced a new perspective on regional
anesthesia. This technologyenables a real-time
visualiza-tionoftheentireprocedure,allowingtheanesthesiologist
to precisely position the needle around the structure to
beblockaded.Thus, ultrasoundenablesadecrease inthe
volume or concentration used during the blockade. This
study has proved it possible to achieve a successful
axil-lary brachial plexus block guided by ultrasound with low
concentrationsoflocalanesthetic.
Adverse events, such as systemic toxicity, may be
dose-dependent.Therefore, prevention of adverse events
is crucial to promote patient safety during regional
anesthesia.5Someguidelinesforregionalanesthesiainclude
localanestheticdoselimitationthroughtheuseofsmaller
volumes and concentrations during blockade. The use of
low doses of local anesthetic provides a safer blockade
with less risk of complications, particularly associated
with the systemic toxicity of these anesthetics. Despite
thedevelopmentof effectivetechniques fortreatingsuch
complications,suchastheuseoflipidsolutions,15,16theuse
oflowdosesoflocalanestheticspromotesablockadewith
ananestheticmassofawiderangeofsafetyrelativetothe
toxicdose.
One way to reduce the dose of local anesthetic is by
decreasing the volume used for the blockade. In a
pre-vious study conducted by ourgroup, the axillary brachial
plexusblockadewassuccessfulwithapproximately1.6mL
of0.5%bupivacainewithepinephrine1:200,000pernerve.11
O’Donnel and Iohom also showed similar results using 2%
lidocaine.6 However, the use of low volume technique is
probablydifficulttoreproduceinclinicalpractice.Onthe
otherhand,thepresentstudyusedavolumemorecloseto
thatusedinclinicalpractice,probablymakingthetechnique
easiertobeapplied.
It is known that the local anesthetic concentration is
animportantfactorinfluencingthelatencytimeof
periph-eralnerveblock.Thelocalanestheticpenetrationintothe
nerverootisaffectedbytheconcentrationofthesolution
used.17 Itis suggestedthatincreasingthelocalanesthetic
concentration around the nerve increases the
concentra-tiongradientandmayfacilitatethediffusionofanesthetic
moleculesintothenerve,andtherebyreducingthenerve
blocklatencytime.However,inthepresentstudy,wefound
amedianlatency closetothe medianlatency obtainedin
ourpreviousstudy,withlowvolumes.11Onepossible
expla-nation is that, despite the low concentration, the total
mass of bupivacaine used in this study was greater than
thatused in the study withlow volumes.Furthermore, a
study comparingdifferent concentrations but maintaining
theanestheticmassfixedinABPBrevealedthatthemotor
latency, but not the sensory latency, was smaller when
usinglargervolumeoflocalanesthetic.18 Thus,thisisnot
adefinedissue, requiring furtherstudies toelucidate the
Theuseoflowerconcentrationsoflocalanestheticmay
bring some benefits. Pippa et al. reported that the use
ofhighconcentrations oflocalanestheticfor interscalene
brachial plexus block is associated with a greater
num-berof complications, such asphrenic nerveparalysis and
hypotension.19 Furthermore, in vitro studies have shown
thattheuseoflocalanestheticsisassociatedwithcytotoxic
effects,includinginductionofapoptosisin Schwanncells,
mitochondrial injury, caspase activation, and increased
cytoplasmic calcium. However, all these effects were
relatedtothe timeof exposureand higherconcentration
ofthedrugused,whichtheoreticallysuggestsgreatersafety
whenusinglowerconcentrationsoflocalanesthetic.20
More-over, the use of lower concentrations may decrease the
postoperativemotorblocktime,whichmaybemore
com-fortableforsome patients.21 Finally, thedose required to
produceasuccessfulblockmaybeclinicallyrelevantin
pedi-atricpatientsorwhenthecombinationofdifferentblocksis
requiredforthesurgeryduetothepotentialriskofsystemic
toxicity.
This study has some limitations. Initially, we do not
measurethe duration of ABPBusing low doses of
bupiva-caine.The use oflow dosesof localanesthetic decreases
block duration, defined as the time between the end
of the blockade onset and recovery of motor and
sen-sory functions.22 As it was not known how the use of
lowconcentrations would influence the block duration,it
wasdecided to include procedures planned to last up to
2h.
Furthermore, this study was not designed to assess
the minimum effective concentration of local
anes-thetic for postoperative analgesia, and further studies
should be performed to evaluate this topic. However, no
patient with successfulblock reported pain 4h after the
blockade.
Wealsoknowthattheresultswerelimitedtoobtainthe
MEC90toa5mLsolutionofbupivacaineforeachABPBnerve,
anditmaynotrepresentthesameconcentrationforsmaller
volumes.Morestudiesshouldbeconductedtoevaluatethe
efficacyofdifferentvolumesforthisconcentration.Finally,
oneshouldnot extrapolatethis resulttoother peripheral
nerveblocks.
In summary, this study suggests that with the use
of ultrasound it is possible to obtain surgical
anes-thesia with concentrations close to 0.25% bupivacaine
when using 5mL volume of anesthetic for each brachial
plexus nerve (radial, median, ulnar, and
musculocuta-neous) by axillary route, decreasing the local anesthetic
doseusedandincreasingtheproceduresafety.More
stud-ies should be conducted to determine the effects that
low concentrations of bupivacaine may have onblockade
duration.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Thompson GE,Rorie DK.Functional anatomyof thebrachial plexussheaths.Anesthesiology.1983;59:117---22.
2.Klaastad O, Smedby O, Thompson GE, et al. Distribution of local anesthetic in axillary brachial plexus block: a clini-cal and magnetic resonance imaging study. Anesthesiology. 2002;96:315---24.
3.Vester-AndersenT,ChristiansenC,SorensenM,etal. Perivas-cularaxillary blockII:influence of injectedvolume oflocal anaesthetic on neural blockade. Acta Anaesthesiol Scand. 1983;27:95---8.
4.GrobanL. Central nervous system and cardiac effects from long-actingamidelocalanesthetictoxicityintheintactanimal model.RegAnesthPainMed.2003;8:3.
5.Maher LE, Copeland SE, Ladd LA. Acute toxicity of local anesthetics:underlyingpharmacokineticandpharmacodynamic concepts.RegAnesthPainMed.2005;30:553---66.
6.O’DonnellBD,IohomG.Anestimationoftheminimumeffective anestheticvolumeof2%lidocaineinultrasound-guidedaxillary brachialplexusblock.Anesthesiology.2009;111:25---9.
7.MarhoferP,SchrogendorferK,WallnerT,etal.Ultrasonographic guidance reduces the amount of local anesthetic for 3-in-1 blocks.RegAnesthPainMed.1998;23:584---8.
8.Casati A, Baciarello M, Di Cianni S, et al. Effects of ultrasound guidance on the minimum effective anaesthetic volume requiredto blockthe femoral nerve. Br J Anaesth. 2007;98:823---7.
9.WillschkeH,BosenbergA,MarhoferP,etal. Ultrasonographic-guided ilioinguinal/iliohypogastric nerve block in pediatric anesthesia: what is the optimal volume? Anesth Analg. 2006;102:680---4.
10.Falcão LF, Perez MV, de Castro I, et al. Minimum effective volumeof 0.5% bupivacaine withepinephrine in ultrasound-guided interscalene brachial plexus block. Br J Anaesth. 2013;110:450---5.
11.FerraroLHC,TakedaA,RezendeAH,etal.Determinationofthe minimumeffectivevolumeofbupivacaine0.5%for ultrasound-guided axillary brachial plexus block. Rev Bras Anestesiol. 2014;64:49---53.
12.HadzicA,DewaeleS,GandhiK,etal.Volumeanddoseoflocal anestheticnecessarytoblocktheaxillarybrachialplexususing ultrasoundguidance.Anesthesiology.2009;111:8---9.
13.Pace NL, Stylianou MP. Advances in and limitations of up-and-downmethodology: aprécisofclinicalus,studydesign, and dose estimation in anesthesia research. Anesthesiology. 2007;107:144---52.
14.CappelleriG, AldegheriG, Ruggieri F,etal. Minimum effec-tiveanestheticconcentration(MEAC)forsciaticnerveblock: subgluteusandpoplitealapproaches.CanJAnaesth.2007;54: 283---9.
15.Lesklw U, Weinberg GL. Lipid resuscitation for local anes-thetictoxicity:isitreally lifesaving?CurrOpinAnaesthesiol. 2009;22:667---71.
16.BemS,AkpaBS,KuoI,etal.Lipidresuscitation:alife-saving antidoteforlocalanesthetictoxicity. CurrPharm Biotechnol. 2011;12:313---9.
17.CasatiA,FanelliG,BorghiB,etal.Ropivacaineor2% mepiva-cainefor lowerlimbperipheralnerveblocks.Anesthesiology. 1999;90:1047---52.
18.KrennH, DeuschE,BaloghB,et al.Increasing theinjection volumebydilutionimprovestheonsetofmotorblockade,but notsensoryblockadeofropivacaineforbrachialplexusblock. EurJAnaesthesiol.2003;20:21---5.
19.Pippa P, Cuomo P, Panchetti A, et al. High volume and low concentration of anaesthetic solution in the perivas-cular interscalene sheath determines quality of block and incidence of complications. Eur J Anaesthesiol. 2006;23: 855---60.
21.FredricksonMJ,SmithKR,WongAC.Importanceofvolumeand concentrationforropivacaineinterescaleneblockinpreventing recoveryroompainandminimizingmotorblockaftershoulder surgery.Anesthesiology.2010;112:1374---81.