ORI GI N AL ARTI CLE
Eva lu a t ion of t h e u se of pr oph yla x is for de e p ve n ou s t h r om bosis in a
t e a ch in g h ospit a l
Gu ilh e r m e Be n j a m im Br a n dã o Pit t aI; Ticia n a Le a l e Le it eI I; M a r ia do D e st e r r o Cost a e SilvaI I I; Ca m illa Fe lix Le ã o de M e loI V; Gise lli de Alm e ida Ca lh e ir osI V
IPhysician. Associat e pr ofessor , Depar t m ent of sur ger y, Univer sidade Est adual de Ciências da Saúde de Alagoas ( UNCI SAL) , Maceió, AL, Br azil. Vascular surgeon, Unidade de Em er gência Arm ando Lages, Maceió, AL, Hospit al Escola José Car neir o, Maceió, AL, Br azil.
I IPhysical Therapy St udent , UNCI SAL, Maceió, AL, Br azil. Scholarship holder, Scient ific I nit iat ion Program .
I I IAssociat e professor, Depart m ent of Physical Ther apy, UNCI SAL, Maceió, AL, Br azil. I VPhysical Therapy St udent , UNCI SAL, Maceió, AL, Br azil.
Correspondence
J Vasc Bras. 2007; 6( 4) : 344- 51.
RESUM O
Con t e x t o: A t rom bose venosa pr ofunda ( TVP) é um a doença freqüent e e gr ave. A pr ofilaxia é o m elhor m eio para reduzir a sua incidência, dim inuindo a m or bim or t alidade gerada por suas
com plicações. Na relação cust o x efet ividade, é m elhor m ant er um a rot ina profilát ica do que t rat ar a doença j á inst alada.
Obj e t ivo: Verificar se a pr ofilaxia da TVP est á sendo ut ilizada de m aneir a adequada e r ot ineir a no Hospit al Escola Dout or José Carneiro ( HEJC) , de Maceió ( AL) .
M é t odos:Foi r ealizado um est udo t ransversal descrit ivo no HEJC durant e o per íodo de 6 m eses. A am ost ra foi de 298 pacient es, de diferent es especialidades. Os dados foram colet ados nos
Con clu sã o: Apesar da eficácia da profilaxia para a TVP j á t er sido com pr ovada e difundida, em nosso m eio ainda não at inge os níveis desej ados de ut ilização.
Pa la vr a s- ch a ve : Prevenção e cont r ole, t r om bose venosa, avaliação.
ABSTRACT
Ba ck gr ou n d: Deep venous t hr om bosis ( DVT) is a frequent and severe disease. Pr ophylaxis is t he best m eans t o r educe it s incidence, low er ing m or bidit y and m or t alit y rat es caused by it s
com plicat ions. I n a cost - effect iveness rat io, it is bet t er t o m aint ain a prophylact ic r out ine t han t o t reat an est ablished disease.
Obj e ct ive : To verify w het her DVT pr ophylaxis is being properly and rout inely used at Hospit al Escola Dout or José Carneiro ( HEJC) , in Maceió, Br azil.
M e t h ods: A descr ipt ive, cr oss- sect ional st udy at HEJC w as carried out for a 6- m ont h per iod. The sam ple w as com posed of 298 pat ient s w it hin different specialt ies. Dat a w er e collect ed from m edical records, and divided int o clinical ( 68.5% ) and sur gical ( 31.5% ) . How DVT pr ophylaxis w as
perform ed w as analyzed for each pat ient . Clinical, phar m acological and sur gical fact ors w er e invest igat ed for all pat ient s. Based on t hese dat a, risk st rat ificat ion w as per for m ed in accor dance w it h t he classificat ion r ecom m ended by Sociedade Brasileira de Angiologia e Cir ur gia Vascular. St at ist ical analysis w as perform ed using soft w are SPSS and t he qui- square and bivariat e correct ion t est s, consider ing p value < 0.05.
Re su lt s: Of t he 298 pat ient s analyzed, 204 belonged t o m edical clinic, in w hich 28.9% w er e low risk, 60.3% average risk and 10.8% high risk for DVT; and 94 pat ient s belonged t o sur gical clinic, in w hich 43.6% w er e low r isk, 52.1% aver age risk and 4.3% high r isk. Only 23% of pat ient s in t he clinical gr oup and 2.1% in t he sur gical gr oup w er e given adequat e pr ophylaxis.
Con clu sion : Despit e t he efficiency of pr ophylaxis for DVT having been confirm ed, it does not reach sat isfact ory levels in our count ry.
Ke yw or ds:Prevent ion and cont r ol, venous t hr om bosis, evaluat ion.
I n t r odu ct ion
Developm ent of venous t hr om boem bolism is dependent on alt erat ion in one or m or e fact ors of t he t riad described by Vir chow in 1856, w hich considers changes in venous st asis, hyper coagulable st at e, and vessel w all inj ur y as r esponsible for t he t hr om bot ic pr ocess.1 Aft er 150 years, t hat st at em ent rem ains t rue, but t he know ledge of t he r elat ive role of each of t hese fact ors incr eased t he under st anding of t he t hr om bot ic phenom enon, allow ing t he diagnosis and ident ificat ion of individuals w it h higher r isk of developing t hrom bosis, t hus aiding in t he m or e rat ional m anagem ent of such pat ient s.2
Deep venous t hr om bosis ( DVT) is a frequent disease, especially as a com plicat ion of ot her sur gical and clinical affect ions. How ever , t hey m ay also occur spont aneously in appar ent ly healt hy
individuals.3
it can be r esponsible for several cases of physical disabilit y and huge socioeconom ic expenses, w it h t he developm ent of severe chr onic venous insufficiency, r esult ing in t he so- called post - t hrom bot ic syndrom e.4 , 5 Venous t hr om boem bolism is also descr ibed as t he m ost com m on cause of
prevent able hospit al m or t alit y.6 , 7
DVT pr ophylaxis is essent ial, since t his disease is t he m ain cause of PE,8 w hich in t ur n can be t he
first m anifest at ion of DVT and is usually fat al in 0.2% of hospit alized pat ient s.9
DVT is t he t hird m ost frequent car diovascular disease in t he USA. Ander son et al. est im at ed ar ound 170,000 new cases of DVT or PE a year , and 9,000 r elapses over t he sam e period, result ing in at least 13,000 deat hs ever y year .1 0
I n our count ry, Maffei's st udy report s an est im at e of 0.6 cases per 1,000 inhabit ant s/ year , based on DVT cases confir m ed by phlebogr aphy or duplex scan.1 1 Fow kes et al., in a r eview st udy, using
a m et a- analysis in 2003, est im at ed t hat w orldw ide incidence of DVT is 0.5 cases per 1,000 inhabit ant s/ year.1 2
The European Consensus for pr event ion of t hr om boem bolic disease est im at es annual incidence of 160 DVT cases and 60 cases of fat al PE for each gr oup of 100,000 inhabit ant s in West er n
count ries.1 3
I n general sur ger y, global incidence of DVT assessed by iodine 125- labeled fibrinogen is 25% in pat ient s w it hout pr ophylaxis.1 4
Clinical suspicion of DVT confir m ed by com plem ent ar y phlebogr aphy exam inat ion w as 40% , report ed by Richar ds.1 5 Sandler et al.1 6 found 58% and Rollo et al.1 7 perform ed a phlebogr aphic
st udy in 424 pat ient s w it h suspicion of DVT and found 68.6% of pat ient s w it h confir m ed diagnosis of DVT.
Over t he past 2 decades, DVT pr ophylaxis has been accept ed as a w ell est ablished and efficacious st rat egy. St udies by Am er ican and Eur opean groups defined det ailed r ecom m endat ions, w hich should be used in all classes of hospit alized pat ient s.9 , 1 8 Despit e DVT pr event ion pr ot ocols being available for all healt h professionals, m any do not use t hem rout inely.1 9 , 2 0
Our st udy aim s at ver ifying w het her DVT prophylaxis is being rout inely and adequat ely used at a t eaching hospit al, w orking w it h t he obser vat ional hypot hesis t hat it is not perform ed accor ding t o current guidelines.
M e t h ods
A cr oss- sect ional, prospect ive and descr ipt ive st udy was perform ed, w it h t he aim of evaluat ing DVT prophylaxis at HEJC fr om Januar y t o June 2006.
The sam ple, defined by convenience, included 298 pat ient s fr om differ ent m edical specialt ies hospit alized at HEJC. Dat a collect ion w as per for m ed t hrough analysis of m edical records of
hospit alized pat ient s, w ho w er e divided int o t w o gr oups: clinical and surgical. Sur gical pat ient w as considered t hat w ho had been subm it t ed t o any t ype of surgical pr ocedur e in cur r ent
relevant ) and out pat ient s.
Each pat ient w as assessed and st r at ified accor ding t o DVT r isk. Clinical, sur gical and
phar m acological fact ors w er e analyzed, follow ing a previously defined prot ocol. Table 1 has t he dat a t hat w er e part of t he st udy pr ot ocol, w hich w er e searched in hospit al records. Once t he prot ocol w as filled in, pat ient s w er e gr ouped in low , m oder at e and high r isk, accor ding t o t he Nor m s of Clinical Guidance of t he Sociedade Brasileira de Cir ur gia e Angiologia Vascular ( SBACV)2 1
Correct use of pr ophylaxis for DVT w as evaluat ed according t o SBACV r ecom m endat ions.2 1 For
low-risk pat ient s r ecom m endat ion is m ovem ent in bed and m ot or t herapy ( physical t herapy) ; for t hese pat ient s, phar m acological pr ophylaxis is not r ecom m ended. For pat ient s at m oderat e risk for DVT, use of unfract ionat ed hepar in ( UFH) subcut aneously ( SC) at a dose of 5,000 I U t w ice a day is indicat ed; anot her opt ion w ould be adm inist rat ion of low m olecular w eight heparin ( LMWH) , SC, at t he low est pr ophylact ic dose r ecom m ended by t he m anufact ur er , once a day. For pat ient s at high risk for DVT, use of UFH, SC at a dose of 5,000 I U, t hree t im es a day is suggest ed; an alt er nat ive w ould be LMWH, SC, at t he highest pr ophylact ic dose r ecom m ended by t he m anufact urer. For all groups adequat e m ot or t herapy should be com bined at each risk, and reassessm ent s should be perform ed daily as t o pr esence of venous t hr om bosis.2 1
Physical prophylact ic m et hods consist of kinesiot her apy for t he low er lim bs;2 2 gr aded com pr ession elast ic st ockings;2 3 int erm it t ent pneum at ic com pr ession;2 4 and w alking. Toget her , t hose
t echniques w or k t o r educe pr obabilit y of DVT incidence. Mot or physical t herapy is r ecom m ended for all DVT risks, w orking as adj uvant t o t he phar m acological t her apy or in cases of cont raindicat ion for use of ant icoagulat ing agent s.
The st at ist ical st udy w as perform ed using t he soft w ar e SPSS version 12.0, in w hich chi- square and bivariat e correct ion t est s w er e used, consider ing p value < 0.05.
Re su lt s
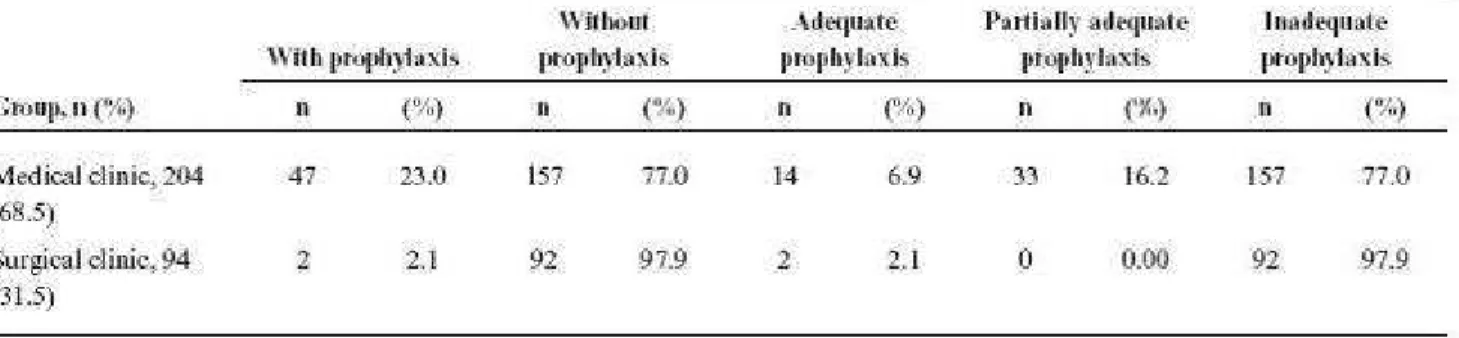
Most pat ient s w er e clinical ( 204- 68.5% ) ; of t hese, only 47 pat ient s ( 23% ) w er e given pr ophylaxis for DVT and, of t hese, only 14 pat ient s ( 29.7% ) w er e given adequat e pr ophylaxis. I t w as m or e frequent ly used in pat ient s at m oder at e r isk. I n pat ient s of t he sur gical group ( 94- 31.5% ) , only t w o ( 2.1% ) w er e given adequat e pr ophylaxis for DVT, one at m oder at e risk and anot her at high risk ( Table 5) .
Of 198 clinical and sur gical pat ient s w ho had indicat ion of phar m acological and physical
prophylaxis, cases of m oder at e and high risk, only 48 ( 24.2% ) w er e given com bined t her apy. Of t hese, 36 ( 18.1% ) w er e m oder at e risk and 12 ( 6% ) w er e high risk.
Correlat ion r isk and adequat e pr ophylaxis in t he clinical gr oup w as 57% ( r = 0.57; p < 0.01) ; how ever , in t he sur gical group t here w as no significant correlat ion, possibly due t o t he fact t hat t here w er e only t w o cases of adequat e pr ophylaxis.
D iscu ssion
DVT pr ophylaxis is needed and cr ucial t o pr event com plicat ions, such as pulm onar y
t hr om boem bolism , and sequelae, such as post t hr om bot ic syndrom e. Mainly due t o DVT silent nat ure, PE is oft en it s first m anifest at ion.2 5 - 2 7
I n t he 1960's, t he nat ur al hist or y of venous t hr om boem bolism w as w ell est ablished aft er t he cont ribut ions by Kakkar et al.2 8 Their st udies dem onst r at ed t hat clinical exam inat ion of DVT alone
has low reliabilit y, since t hey det ect ed t hat 50% or m or e of DVT cases had no clinical signs. Based on t hat discovery, prophylaxis for DVT and
PE gained a new perspect ive, allow ing cr eat ion of consensus and r ecom m endat ions for each risk group for t hat ent it y.2 9 How ever , venous t hr om boem bolism is st ill t he m ain cause of sudden deat h
in hospit al beds.1 8
Prophylaxis is descr ibed as beneficial and, since gr oups of pat ient s at low , m oder at e and high risk for t he developm ent of DVT can be ident ified, it is reasonable and desir able t o consider pr event ion form s, w hich is m uch bet t er t han t reat m ent .9 Alt hough accessible, pr ophylaxis for DVT is st ill
underused, ev en in developed count ries, as dem onst r at ed in t he st udy published by Goldhaber & Tapson, in w hich out of 2,726 pat ient s diagnosed w it h DVT during t heir hospit al st ay, only 1,147 ( 42% ) had been given pr ophylaxis over a 30- day per iod befor e diagnosis.3 0
This st udy show s an even w or se sit uat ion, since out of 198 pat ient s indicat ed t o receive
phar m acological and/ or physical pr ophylaxis, only 6% of high- risk pat ient s and 18% of m oder at e-risk pat ient s w er e given pr ophylaxis. Lack of pr ophylaxis prescript ion for pat ient s indicat ed t o receive it w as higher in t he gr oup of sur gical pat ient s, in w hich 97.9% of pat ient s w er e not given adequat e prophylaxis considering t heir risk. I n t he clinical gr oup, 77% of pat ient s w it h indicat ion w er e not given pr ophylaxis. Ot her st udies per for m ed in differ ent t ypes of hospit al in our count r y also show ed underuse of DVT pr ophylaxis: Gar cia et al.1 verified t hat only 24% of pat ient s w er e
given phar m acological prophylaxis for DVT; Caiafa & Bast os4 found t hat 59% of pat ient s w er e
subm it t ed t o adequat e pr ophylaxis; Engelhorn et al.2 0 dem onst r at ed t hat in 12.7% of cases
adequat e prophylaxis; and Franco et al.,3 1 in an evaluat ion of a t eaching hospit al, obser ved t hat 26.4% of pat ient s w er e given pr ophylaxis.
A possible explanat ion for not using pr ophylaxis for DVT in sur gical pat ient s is concern by healt h professionals as t o risk of bleeding dur ing t he surgery t hat m ay be caused by use of ant icoagulant agent s.2 0 Anot her j ust ificat ion for not using pr ophylaxis is it s financial cost . How ever , Ber gqvist et
al.3 2 show ed t hat use of pr ophylaxis, w hen correct ly indicat ed, has a posit ive cost- benefit r at io.
Anot her possibilit y t o explain underuse of prophylaxis are doubt s regarding classificat ion of risk groups and adequat e indicat ion for each gr oup, since t her e are m any published classificat ions of risk, som e m or e suit able for clinical pat ent s and ot her s bet t er for sur gical pat ient s, such as t he score by Nicolaides et al.9
As t o pr ophylaxis adequacy, it can be seen t hat , even having m any t echnically adequat e
prophylact ic schem es available, bot h phar m acological and physiot her apeut ic, t hey are not alw ays follow ed.2 7
Educat ional pr ogr am s about adequat e prophylaxis of DVT for healt h professionals ar e ext r em ely im port ant . Anderson et al. r epor t ed an increase in use of pr ophylaxis from 29 t o 52% in
hospit alized pat ient s w it h m aj or r isk for developm ent of DVT, aft er int r oduct ion of educat ional st rat egies w it h t he aim of w ar ning professionals for t he im port ance of t hr om boem bolism prevalence. Pr ophylaxis w as higher in hospit als in w hich healt h professionals oft en at t ended educat ional program s. Know ledge of st at ist ical dat a about t hrom boem bolic disease in t he hospit al t hey w or ked w as an im por t ant fact or t hat m ot ivat ed t hem t o use prophylaxis.3 3
Con clu sion
Based on dat a analysis, it can be concluded t hat pr ophylaxis for DVT is being underused, bot h in clinical and sur gical pat ient s, despit e it s efficacy having been confir m ed in several st udies.
I n our st udy, prophylaxis for DVT w as not used in m ost pat ient s, clinical or surgical, and in t hose in w hich it w as used, m ost w as not perform ed adequat ely. This brief st udy dem onst r at ed t he need of cont inuous educat ion for healt h professionals and inst it ut ional educat ive cam paigns for fur t her change in t his sit uat ion, gener at ing unquest ionable benefit s for pat ient s and hospit als.
Re fe r e n ce s
1. Gar cia ACF, Sousa BV, Volpat o DE, Deboni LM, Souza MV, Mar t inelli R, Gechele S. Realidade do uso da profilaxia para t rom bose venosa profunda: da t eoria à pr át ica. J Vasc Bras. 2005; 4: 35- 41. 2. Lour enço DM. Alt erações da hem ost asia que propiciam o t r om boem bolism o venoso. Cir Vasc Angiol. 1998; 14: 9- 15.
3. Maffei FHA. Tr om bose venosa profunda dos m em br os infer ior es: incidência, pat ologia, fisiopat ologia e diagnóst ico. I n Maffei HA, Last oria S, Yoshide WB, Rollo HA Doenças vasculares periféricas. 2ª ed. Rio de Janeir o: Médici; 1995. p. 842.
Marcílio Dias: um m odelo de educação cont inuada. J Vasc Bras. 2002; 1: 103- 12.
5. Caiafa JS. Tr om bose venosa e em bolia pulm onar [ m onogr afia] . Por t o Alegr e: SBACV; 1991. 6. Alper t JS, Dalen JE. Epidem iology and nat ur al hist or y of venous t hr om boem bolism. Prog Cardiovasc Dis. 1994; 36: 417- 22.
7. Rubinst ein I , Murray D, Hoffst ein V. Fat al pulm onary em boli in hospit alized pat ient s: na aut opsy st udy. Ar ch I nt er n Med. 1988; 148: 1425- 6.
8. Bar uzzi ACA, Nussvacher A, Lagudis S, Souza JAM. Tr om bose venosa pr ofunda: profilaxia. Ar q Bras Cardiol. 1996; 67: 215- 8.
9. Nicolaides AN, Br eddin HK, Fareed J, et al. Prevent ion of venous t hr om boem bolism :
I nt ernat ional Consensus St at em ent . Guidelines com piled in accor dance w it h t he scient ific evidence. J Vasc Bras. 2002; 1: 133- 70.
10. Ander son FA Jr., Wheeler HB, Goldber g RJ, et al. A populat ion based perspect ive of t he hospit al incidence and case- fat alit y r at es of deep vein t hr om bosis and pulm onar y em bolism. The
Worchest er DVT st udy. Ar ch I nt er n Med. 1991; 151: 933- 8.
11. Maffei FHA. Tr om bose venosa pr ofunda dos m em br os infer ior es: incidência, pat ologia,
fisiopat ologia e diagnóst ico. I n: Maffei FHA, Last or ia S, Yoshida WB, Rollo HA. Doenças vascular es periféricas. 3ª ed. São Paulo: Medsi; 2002. p. 1363.
12. Fow kes FJ, Pr ice JF, Fow k es FG. I ncidence of diagnosed deep vein t hr om bosis in t he gener al populat ion: syst em at ic review. Eur J Vasc Endovasc Sur g. 2003; 25: 1- 5.
13. Prevent ion of venous t hr om boem bolism : int ernat ional consensus st at em ant ( guidelines according t o scient ific evidence). I nt Angiol. 1997; 16: 3- 38.
14. Heit JA. Risk fact ors for venous t hr om boem bolism . Clin Chest Med. 2003; 24: 1- 12. 15. Richar ds KL, Ar m st r ong JD, Tikoff G, Her shgold EJ, Boot h JL, Ram pt on JB. Noninvasive diagnosis of deep vein t hr om bosis. Ar ch I nt er n Med. 1976; 136: 1091- 6.
16. Sandler DA, Mart in JF, Duncan JS, et al. Diagnosis of deep- vein t hr om bosis: com par ison of clinical evaluat ion,ult r asound, plet hysm ogr aphy, and venoscan w it h X- ray venogr am. Lancet 1984; 2: 716- 9.
17. Rollo HA, Maffei FHA, Last ór ia S, Yoshida WB, Cast iglia V. Uso rot ineiro da flebografia no diagnóst ico da t r om bose venosa pr ofunda dos m em br os infer ior es. Cir Vasc Angiol. 1986; 2: 7- 12. 18. Claget t GP, Ander son FA Jr ., Geer t s W, et al. Prevent ion of venous t hr om boem bolism. Chest 1998; 114 Suppl 5: 531- 60.
19. Keane MG, I ngenit o EPO, Goldhaber SZ. Ut ilizat ion of venous t hr om boem bolism prophilaxis in m edical int ensive car e unit. Chest 1994; 106: 13- 4.
Trombose Venosa Profunda da SBACV. Diretrizes para preven€•o, diagn‚stico e tratamento da trombose venosa profunda. Belo Horizonte: SBACV; 2001. Disponƒvel em: http://www.sbacv-nac.org.br/diretrizes.
22. Kisner RC; Colby LA. Exercƒcios terap„uticos. S•o Paulo: Manole, 1989. p. 435-7.
23. Belen BV, Zorn WGW, Braga PE, Oliveira RSM, Caetano JR O. M…todos n•o-invasivos no estudo das doen€as venosas. In Maffei FHA, Lastoria S, Yoshida WB, Rollo HA. Doen€as vasculares
perif…ricas. 2† ed Rio de Janeiro: MEDSI. p. 785-94.
24. Ilgenfritz FM, Meier JR. Venous velocity increase with a pneumatic foot compression garment. Angiology. 1994:45:949-52.
25. Caiafa JS. Medidas profil‡ticas da doen€a tromboemb‚lica. In: Thomas JB. Sƒndromes venosas: diagn‚stico e tratamento. Rio de Janeiro: Reveinter; 2001. p. 195-208.
26. Baker WF Jr. Diagnosis of deep venous thrombosis and pulmonary embolism. Med Clin North Am. 1998;82:459-76.
27. Marchi C, Schlup IB, Lima CA, Schlup HA. Avaliaۥo da profilaxia da trombose venosa profunda em um hospital geral. J Vasc Bras. 2005;4:171-5.
28. Kakkar VV, Flanc C, Howe CT, Clarke MB. Natural history of postoperative deep vein thrombosis. Lancet. 1969;2:230-2.
29. Silva MC. Tromboembolismo venoso: epidemiologia e fatores de risco. In: Brito CJ, Duque A, Merlo I, Murilo R, Fonseca VL, editores. Cirurgia vascular. Rio de Janeiro: Revinter; 2002. p. 1123-34.
30. Goldhaber SZ, Tapson VF, DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound confirmed deep vein thrombosis. Am J Cardiol. 2004;93:259-62.
31. Franco RM, Simezo VB, Bortoleti RR, et al. Profilaxia para tromboembolismo em um hospital de ensino. J Vasc Bras. 2006;5:131-8.
32. Bergqvist D, Lindgren B, Matzsch T. Comparison of the cost of preventing postoperative deep vein thrombosis with either unfractionated or low molecular weight heparin. Br J Surg.
1996;83:1548-52.
33. Anderson FA Jr., Wheeler HB, Goldberg RJ, et al. Prospective study of the impact of continuing medical education and quality assurance programs on use of prophylaxis for venous
thromboembolism. Arch Intern Med. 1994;154:669-77.
Cor r e spon de n ce :
Ticiana Leal e Leite
Rua Louren€o Moreira da Silva, 267/701, Ponta Verde CEP 57035-360 – Macei‚, AL, Brazil
This st udy was present ed as a post er at t he 58ª Reunião Anual da Sociedade Brasileira par a o Progresso da Ciência ( SBPC) , held in 2006.
Support m odalit y: Scholarship Pr ogr am for Scient ific I nit iat ion ( PROBI C) , gr ant ed by Fundação de Am par o à Pesquisa do Est ado de Alagoas ( FAPEAL) .
This st udy was appr oved by t he research et hics com m it t ee at Univer sidade Est adual de Ciências da Saúde de Alagoas ( UNCI SAL) , pr ocess no. 511/ 2005, w it h per m ission by t he HEJC m anagem ent , and was conduct ed accor ding t o r esolut ion 196/ 96 of Conselho Nacional de Saúde.