www.jped.com.br
ORIGINAL
ARTICLE
Blood
lead
levels
in
a
group
of
children:
the
potential
risk
factors
and
health
problems
夽
Mones
M.
AbuShady
a,∗,
Hanan
A.
Fathy
b,
Gihan
A.
Fathy
a,
Samer
abd
el
Fatah
b,
Alaa
Ali
a,
Mohamed
A.
Abbas
aaNationalResearchCentre,ChildHealthDepartment,Cairo,Egypt
bAtomicEnergyAuthority,NationalCenterforRadiationResearchandTechnology(NCRRT),HealthRadiationResearch
Department,Cairo,Egypt
Received15July2016;accepted22December2016 Availableonline31March2017
KEYWORDS
Bloodleadlevels; Children;
Leadexposure; Abnormalbehavior; Shortstature; Egypt
Abstract
Objective: ToinvestigatebloodleadlevelsinschoolchildrenintwoareasofEgypttounderstand
thecurrentleadpollutionexposureanditsriskfactors,aimingtoimprovepreventionpoliticies.
Subjectsandmethod: Thiswas across-sectionalstudy inchildren (n=400)aged 6---12years
recruited fromtwo areas inEgypt(industrial andurban).Bloodlead levelswere measured
usinganatomicabsorptionmethod.Detailedquestionnairesonsourcesofleadexposureand
historyofschoolperformanceandanybehavioralchangeswereobtained.
Results: ThemeanbloodleadlevelintheurbanareaofEgypt(Dokki)was5.45±3.90g/dL,
whilethatintheindustrialarea(Helwan)was10.37±7.94g/dL,withastatisticallysignificant
differencebetweenbothareas (p<0.05).InDokki,20%ofthestudiedgrouphadbloodlead
levels≥10g/dL,versus42%ofthoseinHelwan.Asignificantassociationwasfoundbetween
childrenwithabnormalbehaviorandthosewithpallorwithbloodleadlevel≥10g/dL,when
comparedwiththosewithbloodleadlevel<10g/dL(p<0.05).ThoselivinginHelwanarea,
thosewithbadhealthhabits,andthoselivinginhousingwithincreasedexposurewereata
statisticallysignificantlyhigherriskofhavingbloodleadlevel≥10g/dL.
Conclusion: LeadremainsapublichealthprobleminEgypt.Highbloodleadlevelswere
sig-nificantlyassociatedwithbadhealthhabitsandhousingwithincreasedexposure,aswellas
abnormalbehaviorandpallor.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽 Pleasecitethisarticleas:AbuShadyMM,FathyHA,FathyGA,FatahSa,AliA,AbbasMA.Bloodleadlevelsinagroupofchildren:the potentialriskfactorsandhealthproblems.JPediatr(RioJ).2017;93:619---24.
∗Correspondingauthor.
E-mail:[email protected](M.M.AbuShady).
http://dx.doi.org/10.1016/j.jped.2016.12.006
PALAVRAS-CHAVE
Níveisdechumbono sangue;
Crianc¸as; Exposic¸ãoao chumbo; Comportamento anormal; Baixaestatura; Egito
Níveisdechumbonosangueemumgrupodecrianc¸as:possíveisfatoresderisco
eproblemasdesaúde
Resumo
Objetivo: Investigarosníveisdechumbonosangue(NCSs)emcrianc¸asemidadeescolarem
duasáreasdoEgitoparaentenderaatualexposic¸ãoàpoluic¸ãoporchumboeseusfatoresde
risco,paramelhoraraspolíticasdeprevenc¸ão.
Indivíduosemétodo: Essefoiumestudotransversalemcrianc¸as(400)comidadesentre6---12
anos recrutadasde duas áreas no Egito(industrial e urbana).Os NCSs foram medidos por
ummétododeabsorc¸ãoatômica.Foramobtidosquestionáriosdetalhadossobreasfontesde
exposic¸ãoaochumboeohistóricodedesempenhoescolarequaisqueralterac¸ões
comporta-mentais.
Resultados: ONCSnaáreaurbanadoEgito(Dokki)foi5,45±3,90g/dL,aopassoquenaárea
industrial(Helwan)foi10,37±7,94g/dL,comumadiferenc¸asignificativaentreambasasáreas
(p<0,05).NaáreadeDokki,20%dogrupoestudadoapresentaramNCSs≥10g/dL,aopasso
quenaáreadeHelwanfoi42%.Foiencontradaumaassociac¸ãosignificativaentreascrianc¸as
com comportamento anormal e aquelas compalidez com NCS≥10g/dL, em comparac¸ão
àquelas comNCS<10g/dL(p<0,05).Aquelas quemoramnaárea deHelwan aquelascom
hábitos de saúderuins eaquelas que moramem moradias commaiorexposic¸ão estiveram
significativamenteemaltoriscodeapresentarNCS≥10g/dL.
Conclusão: OchumboaindaéumproblemadesaúdepúblicanoEgito.AltosNCSsforam
signi-ficativamenteassociadosahábitosdesaúderuinsemoradiacommaiorexposic¸ão,bemcomo,
comportamentoanormalepalidez.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo
OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Bloodleadlevel(BLL)isamajorhealthhazard,especially inchildren,whichwarrantsitsfrequentmonitoringinorder toavoidleadexposureasmuchaspossible.1Leadhasbeen usedinmanyproductssuchaspaint,pipes,andceramics, andremainsapublichazard.Themainsourcesofleadand itspollutionareminingoperations,batteryrecyclingplants, andsmelting,2,3aswellasoldlead-basedpeeledorchipped paint,especiallyduringrenovationsofoldhouses,4,5contact withcontaminateddustorsoil,6leadinplumbing, automo-bileexhaust,by-productsofbothminingandmetalworking, and various consumer products.7,8 E-scrap recycling is an emergingareaofconcernasasourceofoccupational expo-suresamongworkersandasourceoftake-homeexposures.9 Leadis not knownto serveany physiological function, butitexistsinalmostallbiologicalsystems.Itisabsorbed via different routes; however, ingestion of contaminated dietaryconstituentsaccountsforthemajority oflead tox-icityinchildren.10 Childrenaremorelikelytobeexposed thanadultsduetoahighrateofinhalationandmore intesti-nalabsorption.Intense,high-doseexposuretoleadcauses acutesymptomaticpoisoning, characterizedbycolic, ane-mia,anddepressionofthecentralnervoussystemthatmay resultin coma,convulsions,anddeath. LowBLLsarenow knowntoaffectmultipleorgansintheabsenceofapparent symptoms.Toxicitywithlow leadlevelsin uteroand dur-ingchildhoodconstitutesbrainandnervoussystemdamage. Exposureto low BLL (lessthan 10g/dL)affects alsothe immune,reproductiveand cardiovascularsystems.Recent researchindicatesthat,atbloodlevelsof5g/dLorlower,
neurobehaviouraldamageisliabletooccur.Itappearsthat braininjurycanhappenatanybloodlevelthreshold.11---13
The goals of the present study were to evaluate the extentofleadexposureinschoolchildren,whoseageranged from6to12years,inindustrialandurbanareasinEgyptand to investigate the possible influencing factors in orderto clarifythecurrentproblemofleadexposureandtoimprove methodsofpreventionandcontrol.
Subjects
and
methods
Twohundredprimaryschoolchildrenwererandomlychosen in an industrial area in Egypt (Helwan); the same num-ber of primary school children was selected in an urban areainEgypt(Dokki).Thestudywasapprovedbythe Medi-calEthicalCommitteeofNationalResearchCentre,Dokki, Cairo,Egypt.Parentalconsentswereobtained.Parentswho opted tojoin the study answered detailedquestionnaires onsourcesofwatersupply,housing(oldhouseswith defec-tivepaints/useoflead-glazedceramics),livingwithadults whose jobinvolvebattery repair,recycling, orprocessing, dietaryhabits(e.g.,usingnewspaperstowrapthechildren’s food),exposuretoairpollution(locationofthehouseclose tomainroads), andoutdoorplayingindustareas.History ofschoolperformance,behavioralchanges(suchasanxiety andaggressiveness),andanyclinicalproblemswere investi-gated.Teachersandotherschoolstaffwereaskedtoassess eachchild’sperformanceandbehaviors.
wasalsoperformedthroughaninterviewwithaspecialist. CompletebloodcountandBLLwereassessed.
Bloodsampleswerecollectedaccording tothe instruc-tionsoftheCentersofDiseaseControlandPrevention(CDC). Allsamplecollectiontubesandmaterialswerepre-screened for lead contamination. Bloodsamples were analyzed for lead level with the atomic absorption method described byMilleretal.,14 usingheatinggraphiteatomization(HGA 600perkinElmer).BLLswereconsideredas‘‘elevated’’or ‘‘level of concern’’ ifequal to or greater than 10g/dL, inaccordancewiththeUSCentersforDiseaseControland Preventioncriteria.15
Statisticalanalysis
Statistical analysis was performed using SPSS version 16 for Windows(SPSSInc.,version16 for Windows,IL, USA). Continuousdata(BLLs)wereexpressedasmean±standard deviationandwerecomparedusingStudent’st-test. Cate-goricaldatawereexpressedasfrequenciesandpercentages, and were analyzed with the two-tailed chi-squared test. Multiple logistic regression analysis was used to analyze thepredictorsofBLL≥10g/dLandtomodifythe
associ-ationbetweentheclinicaldataandhighBLLbyaddingthe covariates.p-Values<0.05 were considered tobe statisti-callysignificant.
Results
Atotalof400childrenwereenrolledinthepresentstudy; their age ranged from 6 to 12 years, with a mean of 9.40±2.33.Fromthetotal,205childrenweremalesand195 werefemales.MeanBLLwas10.37±7.94g/dLinHelwan
and 5.45±3.90g/dL in Dokki, with a significant
differ-encebetweenbothareas(p<0.05).Nosignificantdifference was found between the genders in both areas regarding BLL (p>0.05). In Dokki, 20% of the studied group had BLLs≥10g/dL,while in Helwanthis valuewas42%. The
percentageofchildrenwithBLL≥5g/dLwas44%inDokki, versus64%inHelwan.
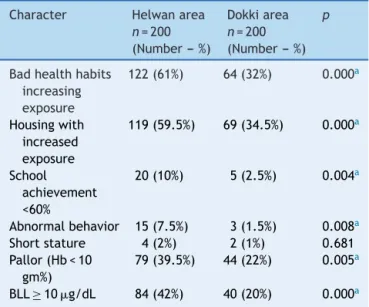
The socialandclinicaldataofthestudypopulationare presentedinTable1,showingthatchildreninHelwanhad significantly worse results in health habits, housing with increased exposure, school achievement <60%, abnormal behavior,andpallorthanchildreninDokki(p<0.05).
Theassociationbetweenclinicaldataofallchildrenand highBLLispresentedinTable2.Asignificantassociationwas observedbetweenBLL≥10g/dLandchildrenwithschool achievement <60%,children withabnormalbehavior, chil-dren with shortstature, andpallor, when compared with thosewithBLL<10g/dL(p<0.05).
Multiplelogisticregressionanalysiswasdonetostudythe predictorsofhighbloodleadlevel(≥10g/dL;Table3).It wasfoundthatthoselivinginHelwan,thosewithbadhealth habits,andthoselivinginhousingwithincreasedexposure wereatasignificantlyhigherriskofhavingBLL≥10g/dL (OR=2.16,95%CI1.35---3.47;OR=1.947,95%CI1.22---3.10; OR=1.72,95%CI1.09---1.09,respectively,p<0.05inall).
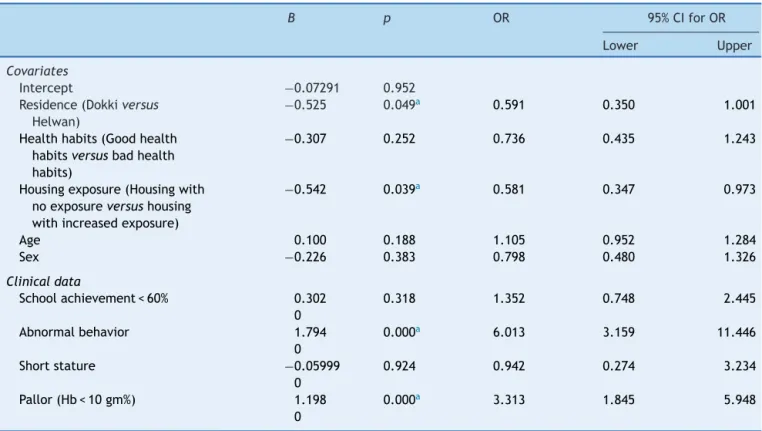
Table4showstheassociationbetweentheclinicaldata andhighBLLaftermodificationbythepredictorsofhighBLL ascovariates.Abnormalbehaviorandpallorwereassociated
Table1 Clinicalandsocial data ofthe studypopulation
(n=400).
Character Helwanarea
n=200
(Number--- %)
Dokkiarea
n=200
(Number--- %)
p
Badhealthhabits
increasing exposure
122(61%) 64(32%) 0.000a
Housingwith increased exposure
119(59.5%) 69(34.5%) 0.000a
School achievement <60%
20(10%) 5(2.5%) 0.004a
Abnormalbehavior 15(7.5%) 3(1.5%) 0.008a
Shortstature 4(2%) 2(1%) 0.681 Pallor(Hb<10
gm%)
79(39.5%) 44(22%) 0.005a
BLL≥10g/dL 84(42%) 40(20%) 0.000a
Hb,hemoglobin;BLL,bloodleadlevel.
a p-Values<0.05wereconsideredassignificant.
withhigh BLL≥10g/dL (p<0.05), while school
achieve-ment<60%andshortstaturewerenotassociatedwithhigh BLL(p>0.05)aftermodificationbythecovariates.
Discussion
Childhoodlead poisoning is a majorproblem that can be preventedworldwide.Inthecurrentstudy,meanBLLinan urban area of Egypt (Dokki) was5.45±3.90g/dL, while
thatinanindustrialarea(Helwan)was10.37±7.94g/dL.
In Dokki, 20% of the studied group had BLLs≥10g/dL, versus 42% in Helwan. The percentage of children with BLL≥5g/dLwas 44%in Dokki, versus64% in Helwan. In
Singapore,from1995to1997,themeanreportedBLLwas 6.6g/dLin269children.16Childrenaged12---19yearswere assessedin 1999in theUnited States,anda meanBLL of 1.1g/dLwas found17; from2007 to2010, thegeometric means at age 1---2 years and 3---5 years were found tobe 1.5g/dLand1.2g/dL,respectively.18
Across-sectionalsurveyforBLLsincluded3831children recruitedathospitals in France.Thegeometric meanBLL was1.49g/dL; 0.09% of the children hadBLL exceeding 10g/dL,andin1.5%,BLLexceeded5g/dL.19
In 2011, a study of blood lead concentrations of 226 schoolchildrenwasconductedinAlpuyeca,Morelos,Mexico. ThemeanBLLwas7.23g/dL;BPb>5g/dLand>10g/dL wereobservedin64%and18%ofthechildren,respectively. In almost 50% of the households, the use of lead-glazed ceramicswasreported.20
Table2 Associationofclinicaldataofchildrenandhighbloodleadlevels(≥10g/dL).
Character HighBLL≥10g/dL
n=124
(Number---%)
BLL<10g/dL
n=276
(Number---%)
p
Schoolachievement<60% 18(14.5%) 7(2.5%) <0.000a
Abnormalbehavior 10(8%) 8(2.9%) 0.041a
Shortstature 5(4%) 1(0.4%) 0.019a
Pallor(Hb<10gm%) 67(54%) 57(20.7%) 0.000a
Hb,hemoglobin;BLL,bloodleadlevel.
ap-Values<0.05wereconsideredassignificant.
Table3 Predictorsofhighbloodleadlevel(≥10g/dL;multiplelogisticregressionanalysis).
B p OR 95%CIforOR
Lower Upper
Residence(Dokkiversus
Helwan)
0.763 0.002a 2.145 1.335 3.447
Healthhabits(Good healthhabitsversus
badhealthhabits)
0.664 0.005a 1.943 1.220 3.095
Housingexposure (Housingwithno exposureversus
housingwithincreased exposure)
0.565 0.017a 1.760 1.108 2.796
Age −0.077 0.243 0.926 0.815 1.053
Sex 0.200 0.392 1.222 0.772 1.932
Constant −3.410 0.000 0.033
OR,oddsratio;CI,confidenceinterval.
ap-Values<0.05wereconsideredassignificant.
Children in six communities near to the now-closed KabweminesandsmeltersinZambiawerestudiedforBLL; the mean was4.83g/dL. The lowest BLL measured was
1.36g/dL.ThehighestBLLdetectedusingthetesting
sys-temwas6.5g/dL.23
BLL was also assessed in the Bagega community in Nigeria;themedianwas71g/dL(range:8---332g/dL). Ele-vatedBLL (≥10g/dL) wasfound in99.5% of the studied group.24InWuhan,China,childrenlessthan18yearswere investigatedthroughouttheentireyearof2012.Forall sub-jects,thegeometric meanwas4.48g/dL. Elevated BLLs (≥10g/dL and ≥5g/dL) were found in 2% and in 44%, respectively.25 In SouthAfrica,across-sectionalanalytical studiesincluding160youngschoolchildrenwasperformed. The mean BLL was 7.4g/dL (range: 2.2---22.4g/dL). BLLs≥5g/dLwereobservedin74%ofthechildren,while 16%hadBLL≥10g/dl.26
BLLswereassessedinchildrenlivinginRiyadh,Saudi Ara-bia. The mean(±SD)BLL was5.2±1.7, ranging from1.7 to10.6g/dL;in 17.8% ofchildren, BLL wasgreater than 10g/dL.27
AstudyconductedinthreeschoolsinNablus,Palestine, assessedBLLin178children(140boys,38girls,agerange 6---8years).The meanBLLwas3.2±2.4g/dL,and levels above10g/dLwereobservedin4.5%ofchildren.28
In the present study, high BLLs were found in Helwan area,whichisanoldindustrialareawithmanylead-related industriesandfactories.OtherpredictorsofhighBLLwere badhealthhabits(usingnewspaperstowrapchildren’sfood; no hand washing before meals and after playing outside; contactwithcontaminateddust,soilandtoys;ingestionof preservedeggs;andconsumptionoffriedfood)andhousing withincreasedexposure(oldlead-basedpeeledorchipped paint,renovations,leadinplumbing,anduseofleadglazed ceramics).
Nosignificant differencesweredetectedinthecurrent studybetweenmalesandfemalesinbothDokkiandHelwan regardingBLLs,whichcanbeexplainedbythesimilar behav-iorandoutdooractivitiesofboth genders.Thisresultisin agreementwiththosebyAllenCounteretal.21Caoetal.29 foundthatthemeanBLLsinboys(23.57mg/L)werehigher thanthatingirls (21.2mg/L),which wasexplainedbythe greaterdistinctbehaviorandoutdooractivitiesfoundwith growing boys,leadingtocontactwithenvironmental lead pollution.
Table4 Associationofclinicaldataandhighbloodleadlevel(≥10g/dL)aftermodificationbycovariates(multiplelogistic
regressionanalysis).
B p OR 95%CIforOR
Lower Upper
Covariates
Intercept −0.07291 0.952
Residence(Dokkiversus
Helwan)
−0.525 0.049a 0.591 0.350 1.001
Healthhabits(Goodhealth habitsversusbadhealth habits)
−0.307 0.252 0.736 0.435 1.243
Housingexposure(Housingwith noexposureversushousing withincreasedexposure)
−0.542 0.039a 0.581 0.347 0.973
Age 0.100 0.188 1.105 0.952 1.284
Sex −0.226 0.383 0.798 0.480 1.326
Clinicaldata
Schoolachievement<60% 0.302 0.318 1.352 0.748 2.445 0
Abnormalbehavior 1.794 0.000a 6.013 3.159 11.446
0
Shortstature −0.05999 0.924 0.942 0.274 3.234
0
Pallor(Hb<10gm%) 1.198 0.000a 3.313 1.845 5.948
0
OR,oddsratio;CI,confidenceinterval;Hb,hemoglobin.
a p-Values<0.05wereconsideredassignificant.
associatedwithamodestincreaseinchildren’sBLLs,which areinagreementwiththepresentstudy.
In the present study, school achievement <60%, short stature,andpallor(Hb<10g/dL)wereassociatedwithhigh BLLs (≥10g/dL). Liu et al.30 conducted a prospective cohort study that assessed children in four elementary schools. They detected a significant association between BLL and increased scores for teacher-reportedbehavioral problems (emotional reactivity, anxiety/depression, and pervasivedevelopmentalproblems),whichisinagreement withthe present results. Boys experiencethe deleterious cognitiveeffectsofleadmorethangirlsdo.31
Across-sectionalassessmentinchildrenandadolescents aged 0---17 years from six communities in the Corrientes river basin wasconducted.Childrenand adolescentswith BLLs>5g/dLhadtwicetheriskofstuntingwhencompared withthosewithlowerBLLs.32Fleischetal.33concludedthat, inperipubertalboys,higherBLLswereassociatedwithlower serum IGF-1, which is attributed to the inhibition of the hypothalamic---pituitary-growthaxisbyleadexposure, lead-ingtogrowthdelay.Theresultsoftheprevioustwostudies areinagreementwiththepresentresults,whichindicated asignificantassociationbetweenhighBLLsandstunting.
Thepresentstudyhadsomelimitations,whichincluded itssmallsamplesize;itscross-sectionaldesign,whichmay notallowthefollow-upoftheassociationbetweenclinical dataandBLLs;andthequestionnaireusedtocollect infor-mationonriskfactors,whichmayhavecausedrecallbias.
ThemeasurementofBLLthroughthegoldstandardmethod (graphiteatomicabsorptionmethod)addedstrengthtothe presentstudy.
Inconclusion,BLLwasmeasuredandassociatedto expo-sureriskfactorsintwoareas(oneurbanandoneindustrial) inEgypt.BLLsweresignificantlyhigherintheindustrialarea thanin theurban area.HighBLLswere significantly asso-ciatedwithbad health habitsand housing withincreased exposure,aswellaswithschoolachievement <60%, short stature,andpallor(Hb<10g/dL).
InEgypt,definitiveplansandregulationsshouldbe car-riedouttoimprovethepreventionandcontrolofchildhood lead poisoning. Regulatory policies areneeded to reduce leadrelease from different industries. BLL screening and testing shouldbe improved. In industrialareas, screening programsforBLLshouldbeimplemented.Finally,the pre-ventionandtreatment of childhoodleadpoisoning should beimprovedinEgypt.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.NeedlemanH.Lowlevelleadexposure:historyanddiscovery. AnnEpidemiol.2009;19:235---8.
2.Mackay AK, Taylor MP, Munksgaard NC, Hudson-Edwards KA, Burn-NunesL.Identificationofenvironmentalleadsourcesand pathwaysinaminingandsmeltingtown:MountIsa,Australia. EnvironPollut.2013;180:304---11.
3.Were FH, Kamau GN, Shiundu PM, Wafula GA, Moturi CM. Air and bloodlead levelsin lead acid battery recycling and manufacturingplantsinKenya.JOccupEnvironHyg.2012;9: 340---4.
4.JacobsDE, ClicknerRP,Zhou JY,Viet SM,MarkerDA,Rogers JW,etal.Theprevalenceoflead-basedpainthazardsinU.S. housing.EnvironHealthPerspect.2002;110:A599---606. 5.SpanierAJ,WilsonS,HoM,HornungR,LanphearBP.The
contri-butionofhousingrenovationtochildren’sbloodleadlevels:a cohortstudy.EnvironHealth.2013;12:72.
6.Dixon SL, Gaitens JM, Jacobs DE, Strauss W, Nagaraja J, Pivetz T, etal. Exposureof U.S.childrento residentialdust lead, 1999---2004: II. The contribution of lead-contaminated dusttochildren’sbloodleadlevels.EnvironHealthPerspect. 2009;117:468---74.
7.OyanaTJ,MargaiFM.Spatialpatternsandhealthdisparitiesin pediatricleadexposureinChicago:characteristicsandprofiles ofhigh-riskneighborhoods.ProfGeogr.2010;62:46---65. 8.EdwardsM.Leadpoisoning:apublichealthissue.PrimHealth
Care.2008;18:18.
9.NewmanN,JonesC,PageE,CeballosD,OzaA.Investigation ofchildhoodleadpoisoningfromparentaltake-homeexposure fromanelectronicscraprecyclingfacility----Ohio,2012.MMWR MorbMortalWklyRep.2015;64:743---5.
10.SilbergeldEK.Preventingleadpoisoninginchildren.AnnuRev PublicHealth.1997;18:187---210.
11.World Health Organization (WHO). Childhood lead poi-soning; 2010. Available from: http://www.who.int/ceh/ publications/childhoodpoisoning/en/[cited19.09.15]. 12.GumpBB,MackenzieJA,BendinskasK,MorganR,DumasAK,
PalmerCD,etal.Low-levelPbandcardiovascularresponsesto acutestressinchildren:theroleofcardiacautonomic regula-tion.NeurotoxicolTeratol.2011;33:212---9.
13.LiuJ,GaoD,ChenY,JingJ,HuQ,ChenY.Leadexposureat eachstageofpregnancyandneurobehavioraldevelopmentof neonates.Neurotoxicology.2014;44:1---7.
14.Miller DT, Paschal DC, Gunter EW, Stroud PE, D’Angelo J. Determinationofleadinbloodusingelectrothermal atomisa-tionatomicabsorptionspectrometrywithaL’vovplatformand matrixmodifier.Analyst.1987;112:1701---4.
15.CentersforDiseaseControlandPrevention(CDC)Advisory Com-mittee onChildhood LeadPoisoning Prevention.Interpreting andmanagingbloodleadlevels<10g/dLinchildrenand redu-cingchildhoodexposuresto lead:recommendationsofCDC’s AdvisoryCommitteeonChildhoodLeadPoisoningPrevention. MMWRRecommRep.2007;56:1---16.
16.Sallmén M,LindbohmML,NurminenM. Paternalexposureto leadandinfertility.Epidemiology.2000;11:148---52.
17.FadrowskiJJ,Navas-AcienA,Tellez-PlazaM,GuallarE,Weaver VM, Furth SL. Blood lead level and kidney function in US
adolescents:The ThirdNationalHealth and Nutrition Exami-nationSurvey.ArchInternMed.2010;170:75---82.
18.CentersforDiseaseControlandPrevention(CDC).Bloodlead levelsinchildrenaged1---5years---UnitedStates,1999---2010. MMWRMorbMortalWklyRep.2013;62:245---8.
19.EtcheversA,BretinP,LecoffreC,BidondoML,LeStratY, Gloren-necP,etal.Bloodleadlevelsandriskfactorsinyoungchildren in France, 2008---2009. Int J Hyg Environ Health. 2014;217: 528---37.
20.Farías P, Álamo-Hernández U, Mancilla-Sánchez L, Texcalac-Sangrador JL, Carrizales-Yá˜nez L, Riojas-Rodríguez H. Lead in school children from Morelos, Mexico: levels, sources and feasible interventions. Int J Environ Res Public Health. 2014;11:12668---82.
21.AllenCounterS,Buchanan LH,OrtegaF.Bloodleadlevelsin AndeaninfantsandyoungchildreninEcuador:aninternational comparison.JToxicolEnvironHealthA.2015;78:778---87. 22.Ilmiawati C,Yoshida T, Itoh T, NakagiY, Saijo Y, Sugioka Y,
etal.Biomonitoringofmercury,cadmium,andleadexposurein Japanesechildren:across-sectionalstudy.EnvironHealthPrev Med.2015;20:18---27.
23.CaravanosJ,FullerR,RobinsonS.CentersforDiseaseControl and Prevention (CDC).Notes from thefield: severe environ-mentalcontaminationand elevatedbloodleadlevels among children --- Zambia, 2014. MMWR Morb Mortal Wkly Rep. 2014;63:1013.
24.Ajumobi OO, Tsofo A, Yango M, Aworh MK, Anagbogu IN, MohammedA,et al.Highconcentrationofbloodleadlevels amongyoungchildreninBagegacommunity,Zamfara---Nigeria andthepotentialriskfactor.PanAfrMedJ.2014;18:14. 25.Li Y, Wu S, Xiang Y, Liang X. An investigation of
outpa-tientchildren’sbloodlead levelinWuhanChina.PLOSONE. 2014;9:e95284.
26.Mathee A, Khan T, Naicker N, Kootbodien T, Naidoo S, Becker P. Lead exposure in young school children in South Africansubsistencefishingcommunities.EnvironRes.2013;126: 179---83.
27.El-DesokyGE,Aboul-SoudMA,Al-OthmanZA,HabilaM,Giesy JP.Seasonalconcentrationsofleadinoutdoorandindoordust andbloodofchildreninRiyadh,SaudiArabia.EnvironGeochem Health.2014;36:583---93.
28.Sawalha AF, Wright RO, Bellinger DC, Amarasiriwardean C, Abu-Taha AS, Sweileh WM. Blood lead level among Pales-tinian schoolchildren:a pilot study.East MediterrHealth J. 2013;19:151---5.
29.CaoJ,LiM,WangY,YuG,YanC.Environmentalleadexposure amongpreschoolchildreninShanghai,China:bloodleadlevels andriskfactors.PLOSONE.2014;9:e113297.
30.Liu J, Liu X, Wang W, McCauley L, Pinto-Martin J, Wang Y, et al. Blood lead concentrations and children’s behav-ioral andemotional problems:a cohortstudy.JAMA Pediatr. 2014;168:737---45.
31.KhannaMM.Boys,notgirls,arenegativelyaffectedon cogni-tivetasksbyleadexposure:a pilotstudy.JEnvironHealth. 2015;77:72---7.
32.AnticonaC,SanSebastianM.Anemiaandmalnutritionin indige-nous children and adolescents of the Peruvian Amazon in a contextofleadexposure:across-sectionalstudy.GlobHealth Action.2014;7:22888.