www.jped.com.br
ORIGINAL
ARTICLE
The
association
of
sleep
and
late-night
cell
phone
use
among
adolescents
夽
Babak
Amra
a,
Ali
Shahsavari
b,
Ramin
Shayan-Moghadam
b,
Omid
Mirheli
a,
Bita
Moradi-Khaniabadi
b,
Mehdi
Bazukar
a,
Ashkan
Yadollahi-Farsani
a,
Roya
Kelishadi
b,∗aBamdadRespiratoryandSleepResearchCenter,IsfahanUniversityofMedicalSciences,Isfahan,Iran
bChildGrowthandDevelopmentResearchCenter,ResearchInstituteforPrimordialPreventionofNon-communicableDisease,
IsfahanUniversityofMedicalSciences,Isfahan,Iran
Received8August2016;accepted13December2016 Availableonline28February2017
KEYWORDS
Sleep; Cellphone; Adolescents
Abstract
Objective: Thisstudyaimstoassesstherelationshipoflate-nightcellphoneusewithsleep durationandqualityinasampleofIranianadolescents.
Methods: Thestudypopulationconsistedof2400adolescents,aged12---18years,livingin Isfa-han, Iran.Age, body massindex,sleep duration,cellphone useafter 9p.m.,andphysical activityweredocumented.Forsleepassessment,thePittsburghSleepQualityIndex question-nairewasused.
Results: Theparticipationratewas90.4%(n=2257adolescents).Themean(SD)ageof partici-pantswas15.44(1.55)years;1270participantsreportedtousecellphoneafter9p.m.Overall, 56.1%ofgirlsand38.9%ofboysreportedpoorqualitysleep,respectively.Wake-uptimewas 8:17a.m.(2.33),amonglate-nightcellphoneusersand8:03a.m.(2.11)amongnon-users.Most (52%)late-nightcellphoneusershadpoorsleepquality.Sedentaryparticipantshadhighersleep latencythantheirpeers.Adjustedbinaryandmultinomiallogisticregressionmodelsshowed thatlate-nightcelluserswere1.39timesmorelikelytohaveapoorsleepqualitythannon-users (p-value<0.001).
Conclusion: Late-nightcellphoneusebyadolescentswasassociatedwithpoorersleepquality. Participantswhowerephysicallyactivehadbettersleepqualityandquantity.Aspartofhealthy lifestyle recommendations,avoidance oflate-night cellphoneuse shouldbeencouragedin adolescents.
©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradePediatria.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/
by-nc-nd/4.0/).
夽
Pleasecitethisarticleas:AmraB,ShahsavariA,Shayan-MoghadamR,MirheliO,Moradi-KhaniabadiB,BazukarM,etal.Theassociation ofsleepandlate-nightcellphoneuseamongadolescents.JPediatr(RioJ).2017;93:560---7.
∗Correspondingauthor.
E-mail:[email protected](R.Kelishadi).
http://dx.doi.org/10.1016/j.jped.2016.12.004
0021-7557/©2017PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradePediatria.Thisisanopenaccessarticleunder
PALAVRAS-CHAVE
Sono; Celular; Adolescentes
Associac¸ãoentreosonoeousonoturnodecelularentreadolescentes
Resumo
Objetivo: Este estudovisaavaliararelac¸ão entreousodecelularànoite eadurac¸ão ea qualidadedosonoemumaamostradeadolescentesiranianos.
Métodos: Apopulac¸ãoestudadaconsistiuem2400adolescentes,comidadesentre12e18anos, residindo emIsfahan, Irã.Foramdocumentadosaidade,índice demassa corporal,durac¸ão dosono, usodecelular apósas21h00eprática deatividadefísica.Paraavaliac¸ãodosono, utilizamosoquestionáriodeÍndicedeQualidadedoSonodePittsburgh(PSQI).
Resultados: Ataxadeparticipac¸ãofoide90,4%(n=2257adolescentes).Aidade média(DP) dosparticipantesfoide15,44±(1,55)anos;1270participantesrelataramousodocelularapós as21h00.Emgeral,56,1%dasmeninase38,9%dosmeninosrelataramsonodemáqualidade, respectivamente.Osindivíduos queutilizaramcelularànoiteacordaramàs8h17min(2,33) e osquenão utilizaramacordaramàs8h03min(2,11).Amaiorparte(52%) dosusuáriosde celularànoiteapresentoumáqualidadedesono.Aquelessemnenhumtipodeatividadefísica apresentarammaiorlatênciadosonoqueseusoutrospares.Osmodelosajustadosderegressão logísticabináriaemultinomialmostraramqueosusuáriosdecelularànoiteforam1,39vezes maispropensosatermáqualidadedosonoqueseusoutrospares(valordep<0,001). Conclusão: Ousodecelularànoiteporadolescentesfoiassociadoapiorqualidadedosono.Os participantesfisicamenteativosapresentarammelhorqualidadeemaiortempodesono.Como partedasrecomendac¸õesdeestilodevidasaudável,osadolescentesdevemserincentivados aevitarousodecelularànoite.
©2017PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradePediatria.Este ´
eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/
by-nc-nd/4.0/).
Introduction
Itiswell-documentedthatsleepingisamaincomponentfor solidcognitiveandphysicalfunctions.1,2Sleephasacrucial roleindifferentaspectsoflife3;propersleepisespecially important for children and adolescents.4 It is suggested thatsleepdisturbancesmight increasetheriskofphysical andmentalproblems,especiallyduringadolescence.5Sleep deprivationamongadolescentsisnota newphenomenon; however, in recent years, itsadverse health effects have drawnmoreclinicalandacademicattention.6
The technologicalrevolutionhasmadecellphonesvery attractive and popular.7,8 They have become a part of daily life,9 being increasingly used among children and adolescents,10 andhavebecome oneofthemost common means ofcommunication.5 Somechildren andadolescents aresodependentontheircellphonesthattheytakethem to bed, to ensure that they do not miss any incoming message.11
Duetothewidespreaduseofcellphones,itisimportant tostudypossibleadversehealtheffectsoftheexposure.12 Cell phone use has been reported to be associated with healthproblems.5Anumberofstudieshaveindicatedthat the use of cell phones as a part of electronic media is associatedwithsleepdisorders.Onestudyshoweda signif-icant correlation between cell phone use after lights out and sleep disturbances such asshort sleep duration, low sleepquality,andexcessivedaytimesleepiness,aswellas symptomsof insomniaamongJapanese adolescents.5King etal.demonstratedadecreaseinobjectivesleepefficiency, total sleep time, and rapid eye movement sleep, along withan increased subjective sleeponsetlatency (SOL)in
adolescents.13AccordingtoTroxeletal.,nighttimetexting wasassociatedwithinsufficientsleep.14
The variousfindings of studies in differentpopulations may be due to cultural differences. The use of mobile devicesiswidespreadindifferentcountries,butmost pre-viousstudieshavebeenconductedinWesterncountries.To thebestoftheauthors’knowledge,nopreviousstudyhas beenconductedinthisfieldinMiddleEasternchildrenand adolescents.Theexperienceinthisregardinthepediatric populationislimited.Studyingdifferentpopulationswould helpcomparingthefindingsindifferentcommunities.This studyaimedtoassess,forthefirsttime,therelationshipof late-nightcellphoneusewithsleepqualityanddurationin asampleofIranianadolescents.
Methods
impaired theacademic performancewere notincluded in thisstudy. Datawere analyzed using IBM SPSS (IBMCorp. 2011. IBM SPSS Statistics for Windows, version 20.0. NY, EUA).Cramer’sVandGammatestswereruntodetermine theassociation betweencategorical variables.In orderto comparethequantitativedata, thet-test wasapplied,as wellastheMann---Whitneytestfordatathatdidnotfollow normal distribution. Kruskal---Wallis tests were performed to determine the mean differences between more than twogroupswithnon-normaldistribution.Properbinaryand multinomialregressionanalyseswereperformedinorderto omittheimpactofconfoundingdata.p-values<0.05were consideredtobesignificant.
Background
and
clinical
variables
Clinicalvariablesconsistedofage,sex,cellphoneuseafter 9p.m.,sleepduration,totalsleephour,sleeplatency,length ofactualsleep,bedtime,wake-uptime,healthstatus,and physicalactivity.
ThePittsburghSleepQualityIndex(PSQI)questionnaire, whichconsistsof19self-ratedquestionsandfivequestions ratedbythebed-partnerorroommate,wasused.Thelatter fivequestionsareusedforclinicalinformationonly---they arenottabulated inthescoringofthePSQI,andwerenot reportedoninthisstudy.The19self-ratedquestionsassess awidevarietyoffactorsrelatingtosleepquality,including estimatesofsleepdurationandlatency,aswellasfrequency andseverityofspecificsleep-relatedissues.These19items aregroupedinto sevencomponent scores, each weighted equallyonascalerangingfrom0to3.Thesevencomponent scoresarethen addedtoyield aglobal PSQIscore,which hasrangesfrom0to21;higherscoresindicateworsesleep quality.A global sumof 5 or greater indicates poor sleep quality,whilelessthan5indicatesgoodsleepquality.Inthis study,inadditiontothePSQI,anothervalidated question-nairewasusedtodetermine moreinformation containing demographicvariablessuchasage,sex,weight,height, par-ent’sjob,underlyingillness,physicalactivity,andhistoryof druguse,aswellashealthstatusandsomebehaviorfactors of the population. The Cronbach’s alpha of the PSQI was 0.83.
Results
Theparticipationratewas90.4%,and2257adolescents com-pletedthePSQI(1169malesand1086females).Themean age(±SD)was15.44±1.55years.Overall,1270of partici-pantshadapositivehistoryofusingcellphoneafter9p.m. and892ofthemdidnothavesuchhistory.Sleeplatencywas 24min (SD=21min)and 20min (SD=18min) in cell phone usersandnon-users,respectively.Thisfindingsuggeststhat cellphoneusershadsignificantlyhighersleeplatencythan non-users(p-value<0.001).Thosewhousedcellphoneafter 9p.m.hadameanwake-uptimeof8:17a.m.whereas non-usershadameanwake-timeof8:03a.m.(p-value<0.001). Nosignificantrelationshipregardingthedifferenceoftotal sleeptimeincellphoneusersandnon-userswasobserved (p-value=0.263).
Physical activity was also an important clinical vari-able for the participants; 1314 of them reported to be
physicallyactive,whereas851participantsdidnot. Seden-taryparticipantshadsignificantlylongersleeplatencythan those physically active (p-value<0.001). Totalsleep time wasalsosignificantlyhigherinthe physicallyactivegroup (p-value<0.001).Themeanwake-uptimeofsedentary par-ticipants 8:05a.m. (SD=131min), which was significantly earlier than the others, whose mean wake-up time was 8:12a.m.(SD=153min;p-value<0.001).
Anotherclinicalvariablethatwasmeasuredamong par-ticipants was the body mass index (BMI). The mean BMI was20.36±3.32kg/m2forgirls,and20.85±3.78kg/m2for
boys, and 20.59±3.55kg/m2 for the entire studied
pop-ulation. In total, 658 participants were underweight and had a total sleep time of 7.34h (SD=2.37h), 1346 were eutrophicandhadatotalsleeptimeof7.26h(SD=2.35h), and 241 were overweight and had a total sleep time of 7.08h (SD=2.23h). As presented in Table 1, participants withhigherBMIhadlowertotalsleeptime(p-value=0.023).
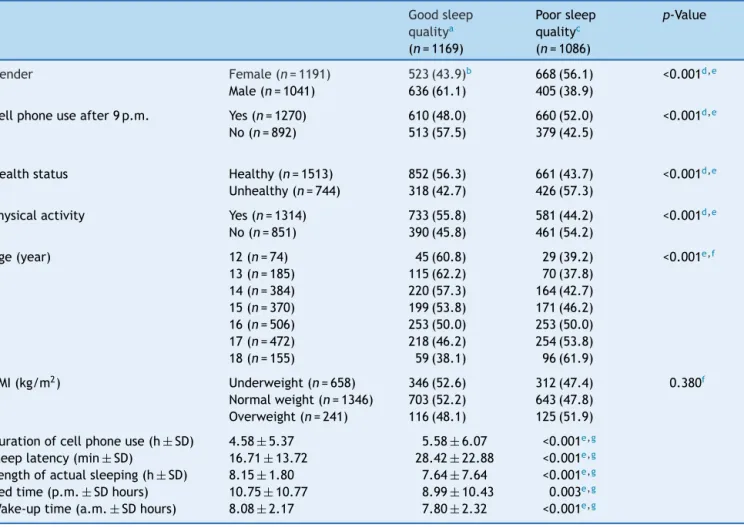
Table2presentstheassociationofsleepquality(based onPSQIscores)withtheclinicalvariablesstudied.Overall, 1270participantshadapositivehistoryofusingcellphones after9p.m.,610(48%)oneofthemhadgood-qualitysleep, whereas660(52%)ofthemhadpoorqualityofsleep. Con-versely,892participantsdidnotusecellphonesafter9p.m. In this group, 513 (57.5%) of participants had good sleep quality,whereas379 (42.5%)hadpoorsleepquality. Late-nightcellphoneusehadasignificantandnegativeimpacton thesleepqualityofparticipants(p-value<0.001).The dura-tionofcellphoneuseamongparticipantswasalsoassessed: those withgood quality of sleepused cell phones for 4h and58min(SD=5h); forthosewithpoorqualityofsleep, thisdurationwas5hand58min(SD=6h).Itwasobserved thatmoretimeofcellphoneusewasassociatedwithpoorer sleepquality(p-value<0.001).
Overall,1191ofparticipantsweregirlsand1041ofthem were boys.It was that 43.9% of girls had goodquality of sleepand56.1%ofthemhadpoorqualitysleep.Conversely, 61.1%ofboyshadgoodsleepqualityand38.9%ofthemhad poorsleepquality.Boyshadsignificantlybettersleep qual-itythangirls(p-value<0.001).Anotherclinicalvariablewas BMI.Overall,658participantswereunderweight,1346were normal-weight,and241participantswereoverweight. Nev-ertheless,nosignificantdifferenceswereobservedbetween sleep quality amonggroups with different BMI categories (p-value=0.38).
Anotherclinicalvariablestudiedwasphysicalactivity;of allparticipants,1314werephysicallyactiveand851were inactive. It was observed that 55.8% of those who were active had good sleep quality and 44.2% had poor sleep quality.Ontheotherhand,45.8%ofphysicallyinactive par-ticipantshadgoodsleepquality,whereas54.2%ofthemhad poorsleepquality.Physicalactivityhadasignificantand pos-itive relationship withsleepquality (p-value<0.001). Age wasalsooneoftheclinicalvariables.Thosewiththebest qualityofsleepweretheyoungest(12-year-olds),whereas the oldest (18-year-olds) had worst quality of sleep (p-value<0.001).
Table1 Characteristicsofstudyparticipants.
Bedtime mean±SDhour (p.m.)
Sleeplatency mean±SDminute
Wake-uptime mean±SDhour (a.m.)
Totalsleepd mean± SD hour
Cellphoneuse after9p.m.
Yes(n=1270) 8.29±10.21 23.90±20.72 8.17±2.33 7.86±2.09
No(n=892) 12.03±10.83 20.23±17.67 7.63±2.11 7.92±2.06
p-Valuea <0.001c <0.001c <0.001c 0.263
Healthstatus Healthy(n=1513) 10.10±10.66 21.65±19.07 7.95±2.22 7.94±2.05 Unhealthy(n=744) 9.49± 10.60 23.78± 20.55 7.94± 2.32 7.83± 2.14
p-Valuea 0.317 0.008c 0.607 0.218
Physicalactivity Yes(n=1314) 10.28± 10.70 21.38± 19.44 8.12± 2.33 8.07± 2.09 No(n=851) 9.27±10.54 23.92±19.69 7.65±2.11 7.60±2.04
p-Valuea 0.003c <0.001c <0.001c <0.001c
BMI(kg/m2) Underweight(n=658) 10.76± 10.73 21.58± 18.84 8.00± 2.29 8.04± 2.13
Normal(n=1346) 9.73±10.62 22.87±20.27 7.95±2.23 7.90±2.07 Overweight(n=241) 8.50± 10.38 21.60± 17.59 7.80± 2.26 7.57± 2.00
p-Valueb 0.039c 0.432 0.679 0.023c
BMI,bodymassindex.
a p-ValuebyMann---Whitney’sUtest. b p-ValuebyKruskalWallistest. c Significantatthelevelof<0.05.
d Totalsleep=(preferredwake-uptime+24)−(preferredbedtime).
associationbetweenoverallPSQIscore(goodvs.poor)and late-nightcellphoneuse(no,yes)wasperformedbyabinary logisticregressionmodel.TheresultsofModel2showedthat late-nightcellphoneuserswere1.39 timesmorelikelyto haveapoorsleepqualitythannon-users(p-value<0.001). Multinomiallogisticregressionanalysesweremadeto inves-tigatetherelationshipbetweeneachofthePSQIsubscales (subjectivesleepquality,sleeplatency,habitualsleep effi-ciency, sleep disturbance, use of sleep medication, and daytimedysfunction)andlate-nightcellphoneuse(no,yes). AspresentedinTable3,inthesleeplatencyPSQIsubscale, thosewho were notlate-night cell phone user were 1.22 times likelytobein the ‘‘no problemat all’’ group than in‘‘averybigproblem’’group(p-value<0.001).Moreover, theoddsratioofbeinginthe‘‘onlyaveryslightproblem’’ groupfornon-userswas1.59timesmorelikelythantobe inthe‘‘averybigproblem’’groupregardingsleeplatency (p-value=0.018).InthehabitualsleepefficiencyPSQI sub-scale,theoddsratiosofbeinginthe‘‘no problemat all’’ groupfornoncellphoneuserswas1.44timesgreaterthanto bein‘‘averybigproblem’’group.Furthermore,inthe day-timedysfunctionPSQIsubscale,noncellphoneuserswere 2.19timeslikelytobein‘‘noproblematall’’groupthanin ‘‘averybigproblem’’group(p-value<0.001).InthisPSQI subscale,theoddsratioofbeingin‘‘onlyaveryslight prob-lem’’groupfor non-userswere1.56timesgreaterthanto bein‘‘averybigproblem’’group(p-value=0.039).
Discussion
Themainobjectiveofthisstudywastoassessthe relation-shipof late-night cellphoneuse (after9p.m.) withsleep parameters such as its duration and quality. The present
findingsshowedthattheuseofcellphonesafter9p.m.was associatedwithpoorer sleepquality, later wake-up time, andhighersleeplatency,butitwasnotdirectlyassociated withsleepduration.
Between2003and2008,thereweremorethan900 mil-lionnewcellphonesubscribersworldwide.15Astudyimplied thattheworldwideproportionofsubscribingtocellphones hasincreased from 5% in 1995 tomore than 70% current usersin2010.10 Nowadays,cellphonesprovidetheirusers withvariousways of communication,suchascalling, tex-ting, sending e-mails; they also allow users to interact withothersonsocialnetworks,usingtheinternet,sharing videosandpictures,andusingdifferent software applica-tions.Considering the mobile natureof cell phones, they canbeusedanywhereandatanytime,unlikeconventional computers.16,17
Table2 Associationofsleepquality(basedonPSQIscores)anddemographicvariables.
Goodsleep qualitya (n=1169)
Poorsleep qualityc (n=1086)
p-Value
Gender Female(n=1191) 523(43.9)b 668(56.1) <0.001d,e
Male(n=1041) 636(61.1) 405(38.9)
Cellphoneuseafter9p.m. Yes(n=1270) 610(48.0) 660(52.0) <0.001d,e
No(n=892) 513(57.5) 379(42.5)
Healthstatus Healthy(n=1513) 852(56.3) 661(43.7) <0.001d,e
Unhealthy(n=744) 318(42.7) 426(57.3)
Physicalactivity Yes(n=1314) 733(55.8) 581(44.2) <0.001d,e
No(n=851) 390(45.8) 461(54.2)
Age(year) 12(n=74) 45(60.8) 29(39.2) <0.001e,f
13(n=185) 115(62.2) 70(37.8)
14(n=384) 220(57.3) 164(42.7)
15(n=370) 199(53.8) 171(46.2)
16(n=506) 253(50.0) 253(50.0)
17(n=472) 218(46.2) 254(53.8)
18(n=155) 59(38.1) 96(61.9)
BMI(kg/m2) Underweight(n=658) 346(52.6) 312(47.4) 0.380f
Normalweight(n=1346) 703(52.2) 643(47.8) Overweight(n=241) 116(48.1) 125(51.9)
Durationofcellphoneuse(h±SD) 4.58±5.37 5.58±6.07 <0.001e,g Sleeplatency(min± SD) 16.71± 13.72 28.42± 22.88 <0.001e,g Lengthofactualsleeping(h± SD) 8.15± 1.80 7.64± 7.64 <0.001e,g Bedtime(p.m.±SDhours) 10.75±10.77 8.99±10.43 0.003e,g Wake-uptime(a.m.± SDhours) 8.08± 2.17 7.80± 2.32 <0.001e,g
PSQI,PittsburghSleepQualityIndex;BMI,bodymassindex.
aGoodsleepquality:PSQIscore<5.0. b n(%).
c Poorsleepquality:PSQIscore≥5.0. d p-ValuebyCramer’sVtest. e Significantatlevelof<0.05.
f p-ValuebyGammatest.
gp-ValuebyMann---Whitney’sUtestonsleepqualitycategories(goodvs.poor).
stressfulandsometimesirritatingcontentofmediais sug-gestedastheunderlyingfactorregardinghowcellphoneuse mayaffectsleep.21
Physical activity and BMI were also considered in the present as twoimportant variables, and their association withsleepparameterswasinvestigated.Theauthorsfound thatcellphoneuseafter9p.m.wassignificantlyassociated withanumberofsleep-related variables.Thosewhoused cellphones after9p.m.hadhigherlevelsofsleeplatency and delayed wake-up time than non-users. No significant relationship was observed between late-night cell phone useandsleepduration.This findingis inlinewithastudy amongTaiwaneseadolescents,whichreportednosignificant relationshipbetween cellphoneuseandsleepduration.22 Likewise, a study amongCanadian children found no sig-nificant relationship between using cell phones for either chatting or texting at night with sleep duration.23 How-ever,astudyinUnitedKingdomshowedthattheuseofcell phonesreducedtotalsleepdurationforaslongas21min.24 InanotherresearchintheUnitedKingdom,cellphoneuse
was associated with 45min decrease in sleep duration.25 Anotherstudyreportedthatsendingatleastonetext mes-sagelate nightwasextremely prevalentand couldaffect thesleepduration.14
association
of
sleep
and
late-night
cell
phone
use
among
adolescents
565
Table3 Associationoflatecellphoneuseandsleepdisturbancesinbinaryandmultinomiallogisticregressionmodels.
Dependentvariable Model1 Model2e
n OR(95%CI) p-Value n OR(95%CI) p-Value
GlobalPSQIa,b Classification 2031 1.44(1.21,1.73) <0.001d 2031 1.39(1.15,1.67) 0.001d
PSQIsubscale
Subjectivesleepqualityc Verygood 1454 1.23(0.77,1.98) 0.386 1365 1.22(0.74,2.00) 0.445
Fairygood 439 1.04(0.63,1.71) 0.885 410 1.09(0.64,1.84) 0.758
Fairlybad 134 1.18(0.66,2.09) 0.579 126 1.04(0.56,1.93) 0.981
Verybad 78 Reference --- 77 Reference
---Sleeplatencyc Noproblematall 588 2.35(1.62,3.41) <0.001d 546 2.11(1.42,3.15) <0.001d
Onlyaveryslightproblem 861 1.69(1.18,2.43) 0.004d 816 1.59(1.08,2.34) 0.018d
Somewhatofaproblem 546 1.54(1.06,2.24) 0.025d 513 1.42(0.95,2.13) 0.086
Averybigproblem 167 Reference --- 156 Reference
---Sleepdurationc Noproblematall 1371 1.27(0.91,1.77) 0.159 1287 1.25(0.87,1.79) 0.236
Onlyaveryslightproblem 384 1.08(0.74,1.57) 0.700 368 1.15(0.77,1.72) 0.654
Somewhatofaproblem 242 0.90(0.60,1.36) 0.613 222 0.93(0.60,1.46) 0.758
Averybigproblem 165 Reference --- 154 Reference
---Habitualsleepefficiencyc Noproblematall 1523 1.39(1.01,1.91) 0.044d 1430 1.44(1.02,2.05) 0.039d Onlyaveryslightproblem 273 1.32(0.90,1.95) 0.155 255 1.47(0.97,2.24) 0.071
Somewhatofaproblem 126 1.12(0.70,1.79) 0.650 120 1.15(0.69,1.91) 0.585
Averybigproblem 184 Reference --- 172 Reference
---Sleepdisturbancesc Noproblematall 145 1.69(0.42,6.82) 0.458 138 1.51(0.36,6.35) 0.575
Onlyaveryslightproblem 1643 1.69(0.44,6.65) 0.449 1540 1.48(0.37,6.00) 0.580
Somewhatofaproblem 334 1.34(0.34,5.29) 0.673 315 1.13(0.27,4.61) 0.870
Averybigproblem 10 Reference --- 10 Reference
---Useofsleepingmedicationc Noproblematall 1903 1.06(0.57,1.97) 0.848 1787 1.23(0.61,2.48) 0.566 Onlyaveryslightproblem 108 1.05(0.51,2.16) 0.892 103 1.26(0.56,2.81) 0.576
Somewhatofaproblem 51 0.91(0.39,2.09) 0.821 49 0.92(0.36,2.34) 0.850
Averybigproblem 43 Reference --- 39 Reference
---Daytimedysfunctionc Noproblematall 635 2.15(1.46,3.19) <0.001d 597 2.19(1.42,3.39) <0.001d Onlyaveryslightproblem 929 1.37(0.94,2.01) 0.104 876 1.56(1.02,2.37) 0.039d
Somewhatofaproblem 416 1.16(0.77,1.74) 0.491 390 1.22(0.78,1.91) 0.384
Averybigproblem 139 Reference --- 129 Reference
---OR,oddsratio;95%CI,95%confidenceinterval.
a GlobalPittsburghSleepQualityIndex(goodsleepquality:PSQIscore<5.0andpoorsleepquality:PSQIscore≥5.0). b Usingbinarylogisticregressionanalysis.
c Usingmultinomiallogisticregressionanalysis. d Significantatlevelof5%.
ofusingcellphonesduringnormalsleepinghoursmay con-tributeto daytimesleepiness, which is in turn related to poorsleepquality.20
The present findings showed that physical activity was positively associated with both sleep quality and quality. Participants who were physically active had lower sleep latency than their sedentary peers. Moreover, total sleep durationandsleepqualitywerehigherinphysicallyactive participants.AstudyamongSwedishadolescentsreported thathigherlevelsofbothsubjectiveandobjectivephysical activityresultedinmorefavorablesubjectiveandobjective sleep.27 Inastudy amongSpanishadolescents,thosewith higherlevelofmorningtiredness,anindicatorofpoorsleep quality,werelesslikelytotakepartinanykindofphysical activity.28Astudyontherelationshipofphysicalactivityand sleepparametersinAmericanadolescentsshowedthat phys-icalactivitywasassociatedwithrememberingwhentired.29
Study
strengths
and
limitations
Themainlimitationofthepresentstudyisitscross-sectional design. Some potential confounding factors were consid-ered,butothervariablesnotconsideredinthepresentstudy may be associated withboth sleeping and late-night cell phoneuse ineither a positive or negativeway. Moreover, thecut-offforsufficientsleeptimewas8h;giventhatthe useofanothercut-offtostratifythesleepintopoorand suf-ficientwouldleadtodifferentresults,theauthorsconsider thisfactasalimitationofthepresent study.Assessingthe correlationbetweensleepandacademicperformancewas onlypossible inthe adolescentage range;therefore,it is reasonabletothinkthatthepresentfindingsmaynotbe sig-nificantinotheragegroups.Themainstrengthofthisstudy isitslarge samplesizeandthefactthatparticipantswith varioussocio-demographic characteristics were recruited. Furthermore,tothebestoftheauthors’knowledge,thisis thefirstlargepopulationbasedstudyofitskindinIran.
In this study, late-night cell phone use wasassociated withpoorersleepqualityinadolescents.Itwasassociated withsleeplatency andwake-up time,howeveritwasnot directly associated with sleep duration. Adolescents who werephysicallyactive hadbetter sleepqualityand quan-tity.Publicawarenessshouldbeincreasedabouttheadverse healtheffectsoflate-nightcellphoneusebyadolescents.
Funding
ThisstudywasfundedbyagrantoftheResearchInstitutefor PrimordialPrevention of Non-CommunicableDisease, Isfa-hanUniversityofMedicalSciences,Isfahan,Iran.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.DewaldJF,MeijerAM,OortFJ,KerkhofGA,BögelsSM.The influ-enceofsleepquality,sleepdurationandsleepinessonschool
performance in children and adolescents: a meta-analytic review.SleepMedRev.2010;14:179---89.
2.NeinsteinLS.Adolescenthealthcare:apracticalguide.5thed. Philadelphia:LippincottWilliams&Wilkins;2008.
3.CurcioG,FerraraM,DeGennaroL.Sleeploss,learningcapacity andacademicperformance.SleepMedRev.2006;10:323---37.
4.AhrbergK,DreslerM,NiedermaierS,SteigerA,GenzelL.The interactionbetweensleepqualityandacademicperformance. JPsychiatrRes.2012;46:1618---22.
5.MunezawaT, KaneitaY,OsakiY, KandaH,Minowa M,Suzuki K,etal.Theassociationbetweenuseofmobilephonesafter lights out and sleep disturbances among Japanese adoles-cents: a nationwide cross-sectional survey. Sleep. 2011;34: 1013---20.
6.AdamsSK,DalyJF,WillifordDN.Adolescentsleepandcellular phoneuse:recenttrendsandimplicationsforresearch.Health ServInsights.2013;6:99---103.
7.AhmedI,QaziTF,PerjiKA.Mobilephonetoyoungsters: neces-sityoraddiction.AfrJBusManag.2011;5:12512---9.
8.KhanMM.Adverseeffectsofexcessivemobilephoneuse.IntJ OccupMedEnvironHealth.2008;21:289---93.
9.Sahin S,Ozdemir K, UnsalA, Temiz N.Evaluation ofmobile phoneaddictionlevelandsleepqualityinuniversitystudents. PakJMedSci.2013;29:913---8.
10.Divan HA, Kheifets L, Obel C, Olsen J. Cell phoneuse and behaviouralproblemsinyoungchildren.JEpidemiolCommunity Health.2012;66:524---9.
11.VandenBulckJ.Textmessagingasacauseofsleepinterruption inadolescents,evidencefromacross-sectionalstudy.JSleep Res.2003;12:263.
12.ThoméeS, HärenstamA, Hagberg M. Mobile phone useand stress,sleepdisturbances,andsymptomsofdepressionamong youngadults---aprospectivecohortstudy.BMCPublicHealth. 2011;11:66.
13.KingDL,GradisarM,DrummondA,LovatoN,WesselJ,MicicG, etal.Theimpactofprolongedviolentvideo-gamingon adoles-centsleep:anexperimentalstudy.JSleepRes.2013;22:137---43.
14.TroxelWM, Hunter G, ScharfD. Say ‘‘GDNT’’:frequency of adolescenttextingatnight.SleepHealth.2015;1:300---3.
15.DivanHA,KheifetsL,ObelC,OlsenJ.Prenatalandpostnatal exposuretocellphoneuseandbehavioralproblemsinchildren. Epidemiology.2008;19:523---9.
16.LeppA, BarkleyJE, Karpinski AC.The relationship between cell phone use, academic performance, anxiety, and satis-faction with life in college students. Comput Hum Behav. 2014;31:343---50.
17.AroraT,BrogliaE,ThomasGN,TaheriS.Associationsbetween specifictechnologiesandadolescentsleepquantity,sleep qual-ity,andparasomnias.SleepMed.2014;15:240---7.
18.FobianAD,AvisK,SchwebelDC.Impactofmediauseon ado-lescentsleepefficiency.JDevBehavPediatr.2016;37:9---14.
19.LemolaS, Perkinson-GloorN, BrandS, Dewald-Kaufmann JF, GrobA.Adolescents’electronicmediauseatnight,sleep dis-turbance,anddepressivesymptomsinthesmartphoneage.J YouthAdolesc.2015;44:405---18.
20.Polos PG, Bhat S, Gupta D, O’Malley RJ, DeBari VA, Upad-hyayH,etal. TheimpactofSleepTime-RelatedInformation and Communication Technology (STRICT) on sleep patterns anddaytime functioninginAmericanadolescents. JAdolesc. 2015;44:232---44.
21.ExelmansL,VandenBulckJ.Bedtimemobilephoneuseand sleepinadults.SocSciMed.2016;148:93---101.
22.YenCF,KoCH, YenJY, ChengCP.The multidimensional cor-relates associated with short nocturnal sleep duration and subjective insomnia among Taiwanese adolescents. Sleep. 2008;31:1515---25.
devicesare associatedwithshort sleepdurationand obesity amongCanadianchildren.PediatrObes.2013;8:42---51.
24.AroraT,HussainS,HubertLamKB,LilyYaoG,NeilThomasG, TaheriS.Exploringthecomplexpathwaysamongspecifictypes oftechnology,self-reportedsleepdurationandbodymassindex inUKadolescents.IntJObes(Lond).2013;37:1254---60.
25.CalamaroCJ,MasonTB,RatcliffeSJ.Adolescentslivingthe24/7 lifestyle:effectsofcaffeineandtechnologyonsleepduration anddaytimefunctioning.Pediatrics.2009;123:e1005---10.
26.NathanN,ZeitzerJ.Asurveystudyoftheassociationbetween mobilephone useand daytime sleepiness inCalifornia high-schoolstudents.BMCPublicHealth.2013;13:840.
27.Lang C, Brand S, Feldmeth AK, Holsboer-Trachsler E, Pühse U,GerberM.Increasedself-reportedandobjectivelyassessed physicalactivitypredictsleepqualityamongadolescents. Phys-iolBehav.2013;120:46---53.
28.Ortega FB,Chillón P,RuizJR, DelgadoM,Albers U, Alvarez-Granda JL, et al. Sleep patterns in Spanish adolescents: associationswithTVwatchingandleisure-timephysicalactivity. EurJApplPhysiol.2010;110:563---73.