w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Postoperative
outcomes
and
functional
results
after
Deloyer’s
procedure
–
a
retrospective
cohort
study
Noel
Salgado-Nesme
a,∗,
Omar
Vergara-Fernández
a,
David
Mitre-Reyes
a,
Hugo
A.
Luna-Torres
a,
Juan
Francisco
Molina-López
a,
Adolfo
Navarro-Navarro
a,
Jorge
Guevara-Chipolini
baInstitutoNacionaldeCienciasMédicasyNutrición“SalvadorZubirán”,DepartamentodeCirugíaColorrectal,MexicoCity,Mexico bUniversidadLaSalle,FacultadMexicanadeMedicina,MexicoCity,Mexico
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9November2016 Accepted15February2017 Availableonline7March2017
Keywords:
Procedure
Extendedlefthemicolectomy Isoperistaltictransposition Lowcolorectalanastomosis Hartmann’sprocedure
a
b
s
t
r
a
c
t
Introduction:TheobjectiveofourstudywastodescribesurgicaloutcomesofDeloyers proce-dureinourreferralcenter,andtocomparetheresultsofpatientswithandwithoutprotective ileostomy.
Methods:PatientsundergoingaDeloyersprocedurefrom2013to2016wereprospectively included.Generalcharacteristics,intraoperativevariables,postoperativecourse,and func-tionaloutcomeswereanalyzed.Patientswerecomparedintotwogroups:group(1)patients undergoingDeloyersprocedurewithoutileostomy,andgroup(2)Deloyersprocedurewith protectiveileostomy.
Results:Sixteenpatientsundergoingisoperistaltictranspositionoftherightcolonremnant wereincluded,ofwhich9(63%)weremaleswithamedianageof47(range22–76)years. Themainsurgicalindicationwastherestorationofboweltransit(62.5%).Therewashigher majormorbidityrateintheDeloyersprocedurewithprotectiveileostomygroup,butwithout statisticalsignificance(20%vs.9%,p=0.92).Noleaksordeathswerereported.Thelength ofhospitalstaywas7days.Themeannumberofbowelmovementsperdaywas4at18 monthsoffollowup.Onlyfour(25%)patientsusedirregularlyloperamide.
Conclusions:TheDeloyersprocedurehassatisfactoryresultsandisreproduciblewithlow morbidity.Themajorandminormorbidityratesweresimilarbetweengroups,suggesting thatthecostsandrisksofasecondprocedurecanbeavoidedbyprovidingasafeprimary anastomosis.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](N.Salgado-Nesme). http://dx.doi.org/10.1016/j.jcol.2017.02.002
Desfechos
pós-operatórios
e
resultados
funcionais
após
o
procedimento
de
Deloyer
–
um
estudo
de
coorte
retrospectivo
Palavras-chave:
Procedimento
Hemicolectomiaextensaà esquerda
Transposic¸ãoisoperistáltica Anastomosecolorretalbaixa ProcedimentodeHartmann
r
e
s
u
m
o
Introduc¸ão:Oobjetivodenossoestudofoidescreverosresultadoscirúrgicosdoprocedimento deDeloyeremnossocentrodereferênciaecompararosresultadosdepacientescomesem ileostomiadeprotec¸ão.
Métodos: PacientessubmetidosaoprocedimentodeDeloyerde2013a2016foramincluídos prospectivamente.Foramanalisadasascaracterísticasgerais,asvariáveisintraoperatórias, ocursopós-operatórioeosdesfechosfuncionais.Ospacientesforamcomparadosemdois grupos:Grupo1)pacientessubmetidosaoprocedimentodeDeloyer(PD)semileostomia,e grupo2)procedimentodeDeloyercomileostomiadeprotec¸ão(IP).
Resultados: Foramincluídos 16 pacientessubmetidos à transposic¸ão isoperistáltica da porc¸ãoremanescentedocólondireito,dosquais9(63%)eramdosexomasculinocomidade médiade47anos(variac¸ãode22-76)anos.Aprincipalindicac¸ãocirúrgicafoiarestaurac¸ão dotrânsitointestinal(62,5%).HouvemaiormorbidademaiornogrupoIP,massem sig-nificânciaestatística(20%vs.9%,p=0,92). Nenhumvazamentoouóbitofoirelatado. A durac¸ão dahospitalizac¸ãofoi de7 dias.Onúmero médiodeevacuac¸ões por diafoi 4, aos18mesesdeseguimento.Apenasquatro(25%)pacientesutilizaramirregularmentea loperamida.
Conclusões: OprocedimentodeDeloyertemresultadossatisfatórioseéreprodutívelcom baixamorbidade.Astaxasdemorbidadesmaioresemenoresforamsemelhantesentreos grupos,sugerindoqueoscustoseriscosdeumsegundoprocedimentopodemserevitados proporcionando-seumaanastomoseprimáriasegura.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
The vast majority of patients suffering from complicated diverticulardiseaseinLatinAmericaaresubjectedtoa Hart-mann’sprocedure (sigmoid colonremovalwithdescending coloncolostomyandrectalstump).Sometimes, reconstruc-tionofboweltransitbecomesadifficultprocedurebecause awideresectionorownextensionofthemiddlecolicartery preventsatension-freeanastomosis.
Deloyersprocedure,described bytheauthor in1964,1 is thefirstreferenceoftheartandhassincebeenmentioned infrequentlyinthemanagementofchronicorHirschsprung constipation.2,3Somearticleshighlightingtheimportanceof thisprocedureasasafealternativeforthereconstructionof boweltransitafteranextendedlefthemicolectomyhavebeen publishedinthelastdecade.
Theobjective ofourstudy wastoanalyzepostoperative andfunctionaloutcomes inaseriesofpatientsundergoing aDeloyersprocedure,andtocomparetheresultsofpatients withandwithoutprotectiveileostomy.
Patients
and
methods
PatientsundergoingaDeloyersprocedurewereprospectively includedfromFebruary2013toMarch2016inareferral cen-ter. Monitoring, demographic, and intraoperative variables werecomparedaccordingtotwogroups:patientsundergoing
Deloyers procedure (DP) without protective ileostomy vs. Deloyersprocedurewithprotectiveileostomy(PPI).
Operative mortality was defined as those that occurs within30daysoftheprocedure.Postoperativemorbiditywas includedintheClavien-Dindoclassificationsystem.4 Compli-cationswereclassifiedasminor(Clavien-DindoGrade<III)or major(≥Clavien-DindoGradeIII,IVandV).Thepresenceof anastomoticleakwassuspectedbyclinicalsystemic
inflam-matory response and confirmed with contrast-enhanced
computedtomography.
Adescriptiveandcomparativeanalysiswasperformed.For continuousvariables,themean,standarddeviation,median, ranges, and the rate in percentage points of other vari-ablesobtainedineachgroupweredetermined.Comparison betweengroupswereestimatedwiththechi-square,Fisher’s exactprobabilitytestortheStudent’st-testforcategoricaland continuous variables,respectively. Ap-valueof0.05 or less wasconsideredstatisticallysignificant.Allstatisticalanalyses werecarriedoutusingIBMSPSSStatistics(version23.0).
Surgicaltechnique
All procedures were performed using an open approach.
Fig.1–AnticlockwiserotationinDeloyersprocedure.
wellasthecolonicflexureandtheportionoftransversecolon onthegastrocolicligament;fullyrespectingthemesocolon. Oncethecolonhasbeenreleased,therightbranchofthe mid-dlecolicarteryisidentifiedandsectionedatitsroot,aswellas therightcolicartery(incaseofbeingpresentandbydecision ofthesurgeon).Thecolon,isresectedintheportionwherea visibleandpalpablepulseoftheileocecalvesselsisidentified. Theperitonealfoldisreleasedattheleveloftheileocecalvalve withreleaseoftheterminalportionoftheileumandcecum. Itproceedstoreleasethemesocolonfromtheloweredgeof theduodenumtothebaseoftheileocecalvessels.Ifthececal appendixispreserved,appendectomyismadeusinga cut-tinglinearstapler.Theoriginofthesuperiormesentericartery shouldbeidentified,andafterthecompletemobilizationof mesocolon,itrotatescounterclockwiseensuringthatthereis notwistingofileocaecalvessels(Fig.1).Theanvilofthe circu-larstaplerisplacedintheterminalportionoftheascending colon; staplerisintroduced transanallyand end-end anas-tomosisismadeusingadouble-stapletechnique(Fig.2).A hydropneumatictestisperformed,anddrainclosedtotherear faceoftheanastomosisisplaced.Forpatientswithprotective ileostomy,anilealhandleisexternalizedto30cmfromthe ileocecalvalveontherighttotheumbilicus.Theileostomy closurewasscheduledat8weeksorattheendofadjuvant chemotherapyifnecessary.
Results
Duringthis study,sixteenpatientsunderwent isoperistaltic transpositionoftherightcolonremnantwithcolorectal anas-tomosis(CRA)orcoloanalanastomosis(CAA).Intotal,9(56%) maleswere included. Themedianage was47 years (range 22–76).ElevenpatientswereincludedintheDPgroup(68%). Nodifferenceswerefoundbetweenbothgroupsintermsof age,sex,scoreoftheAmericanSocietyofAnesthesiologists (ASA),body massindex, and the number of comorbidities (Table1).
Fig.2–Endtoendcolorectalanastomosis.
Comorbidity
Charlson index was slightly higher in the group without ileostomy(1.8vs.1.6;p=0.04).TwopatientswithLupus Ery-thematosus were included in primary anastomosis group. Bothpatientshadchronicsteroiduse(20mg/day).Duringthe surgical procedure,an adequate irrigationandfree-tension
Table1–Preoperativedata.
Variable Deloyers(n=11) PPI(n=5) p
Gender 0.36
Male 7(63%) 2(40%)
Age 41.7(±16.6) 59.8(±17.9) 0.74
ASAI–II 7(63%) 3(60%)
0.38 ASAII–IV 4(36%) 2(40%)
BMI(kg/m2) 25.9(±8.3) 26.7(±7.7) 0.93 Charlsonindex 1.8(±2.2) 1.6(±1.1) 0.04 Diverticulardisease 4(36%) 4(80%) 0.14
Coloncancerlocation:
Splenicflexure 2(18%) 0
Leftcolon 1(9%)
Transversecolon 1(9%)
Appendicitis
Incidentalinjury 1(9%) 0 0.45
GSW 1(9%) 0 0.45
Perforatedintestinal tuberculosis
0 1(20%) 0.54
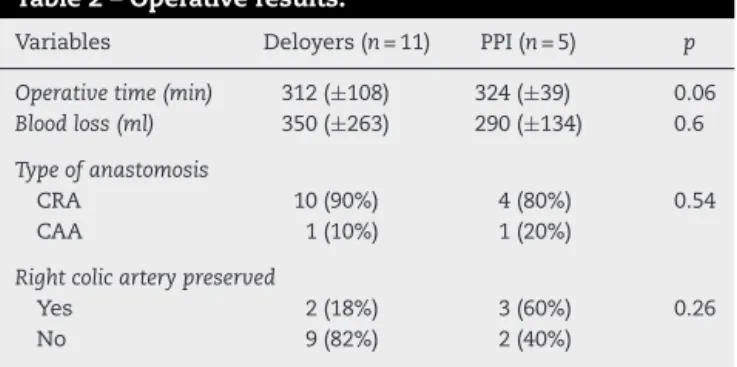
Table2–Operativeresults.
Variables Deloyers(n=11) PPI(n=5) p
Operativetime(min) 312(±108) 324(±39) 0.06 Bloodloss(ml) 350(±263) 290(±134) 0.6 Typeofanastomosis
CRA 10(90%) 4(80%) 0.54
CAA 1(10%) 1(20%)
Rightcolicarterypreserved
Yes 2(18%) 3(60%) 0.26
No 9(82%) 2(40%)
PPI, deloyers procedure+protective ileostomy; CRA, colorectal anastomosis;CAA,coloanalanastomosis.
anastomosis was performed. Both patients had no severe
postoperativecomplications.
Surgicalindications
Themainindicationfortheprocedurewastherestorationof boweltransitin10patients(62.5%).Hartmann’sprocedurewas initiallyperformedforcomplicateddiverticulardiseasein8 patients, forperforatedintestinal tuberculosisin1patient, andforincidentalcolonicinjuryin1patient(Table1).Four patients(25%)withcancerwereincluded:2(12.5%)patients withlocallyextendedtumorintheleftcolicflexure;1(6.2%) patientwithtransversecoloncancer;and1patientwitha his-toryofextendedleftcolectomyforcancer,whorequiredan iterativeresectionforrecurrenceofthetumor.Onepatient withcomplicatedappendicitisandinflammatoryphlegmon withinvolvementofsigmoid,andanotherpatientwitha his-toryoftraumabyfirearmthatrequiredresectionofmultiple intestinalsegmentswereincluded.
Intraoperativefeatures
ThetypesofanastomosisperformedinbothgroupswereCRA (n=14)andCAA(n=2).Theligationoftherightcolicarterywas performedin11patients(68.7%)accordingtothesurgeon’s preference.Theoperativetimebetweentwogroupswas sim-ilar(312vs324min),andintraoperativebleedingwasslightly higherintheDPgroup(350vs.290ml)(Table2).Three(18.75%) patientsweretransfusedduringsurgerywithoneredblood cellspackedperpatient.Thesuctiondrainagewasremoved on12day(6–30).
Postoperativefollow-up
Postoperativeoutcomes
Thelengthofhospitalstaywas7days(5–57).The postopera-tivemortalitywasnull.Halfofthepatientshadcomplications. Major morbidity (Clavien-Dindo≥3) was more frequent in the ileostomy group (20% vs. 9%, p=0.92). There was one patientwithapresacralfluidcollectionineachgroup.Both patientsweretreatedwithpercutaneousdrainageand antibi-otics.Minormorbidity(Clavien-Dindo<3)wassimilarinboth groups(40%vs.36%,p=0.92)and itwas relatedto superfi-cialsurgicalsiteinfections(Table3).Nopatientunderwenta surgicalreoperation.
Table3–Morbidity.
Morbidity Deloyers(n=11) PPI(n=5) p
Clavien-Dindo≤II 4
(36%)
2 (40%)
0.92 Surgicalsiteinfections
Clavien-Dindo≥III 1 (9%)
1 (20%) Presacralfluidcollections
PPI,Deloyersprocedure+protectiveileostomy.
Latemorbidity
Onepatient(6.2%)withCAAandprotectiveileostomy
devel-oped stenosis. This was treated with Hegar dilators. No
complicationswerefoundafterileostomyclosure.
Morbidityatstomaclosure
Ileostomyclosure wasperformedinall patients(n=5).The meantimeperiodforileostomyclosurewas4months(range,
1–6).Abariumenemawasbeforeclosure.Twopatientshad
minor morbidity(1 surgical site infection,and 1 incisional hernia).Andtherewerenotmajorcomplications.
Functional
result
Thefollow-upperiodwas18months(4–38).Themeannumber ofbowelmovementsperdaywas4(range,2–10).Onepatient withCAAhadfecalurgency.Noincontinencewasreported.
Four(25%)patientsweretaking2mgofloperamideperday,
withameannumberofbowelmovementsof4perday.
Discussion
TherepresentativeworksofthisprocedurebyDeloyersand Manceau1,5 in1964and2012respectively,haveshown that theDeloyersprocedureprovidesalowmorbidityandadequate long-termfunctionaloutcome.
Table4–ComparisonofanastomoticleakinDeloyers procedure.
Variable No.ofpatients Anastomotic
leakrate(%)
Sarlietal.12
DP 26 0
PPI 0 0
Manceauetal.5
DP 17 0
PPI 31 0
Dumontetal.15
DP 20 0
PPI 9 11
Kontovounisiosetal.16
DP 5 0
PPI 9 0
Salgadoetal.
DP 11 0
PPI 5 0
DP, Deloyers procedure; PPI, Deloyers procedure+protective ileostomy.
ofappendicitisinthesepatients.Nosecondarycomplications resultingfromthisprocedurewerefoundinourseries.
Thereiscurrentlynorecommendationontheuseof pro-tectiveileostomyduringtheDeloyersprocedure.Inourseries, protectiveileostomywasperformedin5patients(32%),lower numberthanthoseusuallyreportedinotherseries(upto64%). Thedecisiontoperformaprotectiveileostomyinthe minor-ityofpatientswasbasedontheproperreleaseandrotation oftheproximalcolon.Inouropinion,thisprocedureworks verysimilartoanileotransverseanastomosisadequate due toadequatemobilityoftheproximalportionthereofandwith aproperdilationofthesphinctercomplex.5,12,15,16
Inthe increasedmorbidity,theformation ofapresacral collectionwasreportedineachoftheDPvs.PPIgroups.No leakageoftheanastomosissitewasfound.Itissimilartothat recordedinpreviousstudieswithDeloyerswhereanincidence of0–11%5,12,15,16ismentioned(Table4),whichisclearlyhigher thanthatreportedinseriesofileorectalanastomosis men-tionedrangingfrom 3to17%.8,15,17 Itisnoteworthythatin theDPgrouphasalowermajormorbidityrate,andthe mor-bidityassociatedwithstomaclosure wasof40%.Although bothpatientshadaminorcomplication,apatientwithwound infectionandonewithapost-incisionalhernia.Themorbidity resultingfromclosureofderivativeproceduresiswellknown andhasnotnegligiblenumbersofmorbidityratefrom0to 38%andmortalityratefrom0to6.9%.18Nore-surgeriesand mortalitywerereportedinourcompleteseries.
The mostimportant limitations in our study are those inherentbyitsretrospectivenatureandthoseregardingthe selectionofpatients.Thedecisiontodeterminetheneedfor protectiveileostomywasadecision madebythe responsi-ble surgeon. Thesurgical judgment – which considers the patient’sgeneralcondition,associatedcomorbiditiesandeven the typeofanastomosis usedamongother factors – influ-encestheintraoperativedecisionsthatmaybiastheformation ofthegroupsanalyzed.Inourfavor,demographics,Charlson
index,ASAclassification,andsurgicaltime>3hinbothgroups showednodifference,whichtranslatessimilarityof circum-stances.Itisnoteworthythattheexperienceobservedinour series using this techniquebegan with the first patient in February2013withoutrecordofsimilarproceduresperformed atourinstitutionpreviously.
Conclusion
The resultsof the Deloyersprocedure are satisfactory and reproducible. The major and minor morbidity rates were similar betweengroups, suggestingthat themorbidity and costsassociatedwiththeileostomyclosurecanbeavoided inpatientswhoarecandidatesforthisprocedure.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.DeloyersL.Suspensionoftherightcolonpermitswithout exceptionpreservationoftheanalsphincterafterextensive colectomyofthetransverseandleftcolon(includingrectum). Technic–indications–immediateandlateresults.LyonChir. 1964;60:404–13.
2.FasthS,HedlundH,SvaningerG,OreslandT,HultenI. Functionalresultsaftersubtotalcolectomyandcaecorectal anastomosis.ActaChirScand.1983;149:623–7.
3.SarliL,CostiR,SarliD,RoncoroniL.Pilotstudyofsubtotal colectomywithantiperistalticcecoproctostomyforthe treatmentofchronicslow-transitconstipation.DisColon Rectum.2001;44:1514–20.
4.DindoD,DemartinesN,ClavienPA.Classificationofsurgical complications:anewproposalwithevaluationinacohortof 6336patientsandresultsofasurvey.AnnSurg.
2004;240:205–13.
5.ManceauG,KarouiM,BretonS,BlanchetAS,RousseauG, SavierE,etal.Rightcolontorectalanastomosis(Deloyers procedure)asasalvagetechniqueforlowcolorectalor coloanalanastomosis:postoperativeandlongterm outcomes.DisColonRectum.2012;55:363–8.
6.YouYN,ChuaHK,NelsonH,HassanI,BarnesSA,Harrington J.Segmentalvs.extendedcolectomy:measurabledifferences inmorbidity,function,andqualityoflife.DisColonRectum. 2008;51:1036–43.
7.MarianiA,MoszkowiczD,TrésalletC,KoskasF,ChicheL, LupinacciR,etal.Restorationofintestinalcontinuityafter colectomyfornon-oclusiveischemiccolitis.TechColoproctol. 2014;18:623–7.
8.ChristosK,BaloyiannisY,KinrossJ,TanE,RasheedS,Tekkis P.Modifiedrightcoloninversiontechniqueasasalvage procedureforcolorectalorcoloanalanastomosis.Colorectal Dis.2014;16:971–5.
9.UmarUS,KullarN,DorudiS.Rightcolonictransposition technique:whentheleftcolonisunavailableforachievinga pelvicanastomosis.DisColonRectum.2011;54:360–2. 10.ToddIP,Constipation:.Resultsofsurgicaltreatment.BrJSurg.
1985;72Suppl.:S12–3.
colectomyreducingrisksofdigestivesequelae.AnnChir. 1997;51:248–55.
12.SarliL,CostiR,IuscoD,RoncoroniL.Long-termresultsof subtotalcolectomywithantiperistalticcecoproctostomy.Surg Today.2003;33:823–7.
13.DouglasW,DimitrovaM,NandakumarG.Colonicsalvage withantiperistalticcecorectalanastomosis.DisColon Rectum.2015;58:270–4.
14.SaundersBP,PhillipsRK,WilliamsCB.Intraoperative measurementofcolonicanatomyandattachmentswith relevancetocolonoscopy.BrJSurg.1995;82:1491–3. 15.DumontF,DaReC,GoéréD,HonoréC,EliasD.Optionsand
outcomeforreconstructionafterextendedleft hemicolectomy.ColorectalDis.2013;15:747–54.
16.KontovounisiosC,BaloyiannisY,KinrossJ,TanE,RasheedS, TekkisP.Modifiedrightcoloninversiontechniqueasa salvageprocedureforcolorectalorcoloanalanastomosis. ColorectalDis.2014;16:971–5.
17.TangST,YangY,WangGB,TongQS,MaoYZ,WangY,etal. Laparoscopicextensivecolectomywithtransanalsoave pull-throughforintestinalneuronaldysplasiain17children. WorldJPediatr.2010;6:50–4.