w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Pathological
findings
of
colorectal
polyps
analyzed
in
Curitiba
–
Brazil
Renato
Nisihara
a,∗,
Francine
Fudalli
a,
Mariana
Luísa
Mafra
Turra
a,
Rhuanna
Margareth
Malanche
a,
Soraia
Heloise
Benassi
a,
Ana
Paula
Piai
Pimenta
b,
Danielle
Giacometti
Sakamoto
baUniversidadePositivo,DepartamentodeMedicina,Curitiba,PR,Brazil bLaboratóriodePatologiaByori,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15December2016 Accepted11February2017 Availableonline1March2017
Keywords:
Colonoscopy Polyp
Colorectalcancer
a
b
s
t
r
a
c
t
Context:Colorectalcanceristhethirdleadingcauseofdeathfrommalignancyintheworld andthefourthleadingcauseinBrazil’sranks.Adenomatouspolypsareconsidered prema-lignantlesions,anditsresectionreducesbothmorbidityandmortalityrates.
Objectives: Investigatetheprevalenceofpremalignantlesionsandcorrelateitwithageand gender,aswellaswiththelesionfoundprofile:location,morphology,histologyandgrade dysplasia.
Methods:Thiswasaretrospective,observationalanddescriptivestudy.Weanalyzedand tabulatedresultsofpolypsreportssenttoPathologyLaboratoryintheperiodrangingfrom January1toDecember31,2013,inCuritiba,Paraná,Brazil.
Results:Weanalyzed4640reportsofcolorectalpolypectomy,comingfrom3089patients,of whom97.6%wereexaminedbycolonoscopy.Concerninggender,56.5%werefemaleand 43.5%weremale.Themeanagewas57.6years(rangingfrom15to92years).The predom-inantremovalareasofpolypswererectumin26.2%andsigmoidin24.2%cases.About histologicalaspects,themostcommontype–adenoma–waspresentin75.1%polyps,of which74.2%weretubularand21.7%wereserrated.Amongthenon-adenomatouspolyps, hyperplasticprevailedwith88.7%cases.Malignancywasobservedin100cases(2.15%).
Conclusion: Thisstudyshowedhigherincidenceofcolorectalpolypsinwomen,although adenocarcinomas are equallydistributed inbothsexes. Inaddition,the averageageof patientsundergoingcolonoscopyisdecreasing.Furthermore,2.15%polypssentfor pathol-ogyanalysiswerefoundtobemalignant.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](R.Nisihara).
http://dx.doi.org/10.1016/j.jcol.2017.02.001
Achados
anatomopatológicos
de
pólipos
colorretais
analisados
em
Curitiba
–
Brasil
Palavras-chave:
Colonoscopia Pólipo
Câncercolorretal
r
e
s
u
m
o
Contexto: Ocâncercolorretal(CCR)éaterceiracausademortepor doenc¸amalignano mundoe,noBrasil,ocupaaquartaposic¸ão.Ospóliposadenomatosossãoconsiderados lesõespré-malignaseasuaressecc¸ãodiminuiataxademorbimortalidade.
Objetivos: Verificaraprevalênciadaslesõespré-malignasemalignas,correlacionandocom aidadeegênero,comperfildalesãoencontrada:tamanho,localizac¸ão,aspectomorfológico, tipohistológicoegraudedisplasia.
Métodos: Estudoretrospectivo,observacionaledescritivo.Foramanalisadososresultados doslaudosencaminhadosaumLaboratóriodePatologia,noperíododejaneiroadezembro de2013,emCuritiba,Paraná,Brasil.
Resultado: Nototal,analisou-se4640laudosdepolipectomiascolorretais,oriundosde3089 pacientes,dosquais97,6%realizaramexameporcolonoscopia.Emrelac¸ãoaogênero,56,5% erammulherese43,5%homens.Aidademédiafoi57,6anos(entre15e92anos).Oslocais predominantesderetiradadospóliposforamreto(26,2%)esigmoide(24,2%)doscasos. Emrelac¸ãoaosaspectoshistológicos,otipomaiscomumfoiadenoma,presenteem75,1% dospólipos,dosquais74,2%eramdotipotubulare21,7%serrilhado.Dentreospóliposnão adenomatosos,predominouohiperplásicocom88,7%doscasos.Apresenc¸ademalignidade foiobservadaem100casos(2,15%).
Conclusão: Opresenteestudoevidencioumaiorfrequênciadepóliposcolorretaisem mul-heres,emboraosadenocarcinomasestejamdistribuídosigualmenteemambosossexos. Alémdisso,a médiadeidadedosindivíduosquefazemcolonoscopiaestádiminuindo. Malignidadefoiencontradaem2,15%dospóliposencaminhadosparaanálise anatomopa-tológica.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
Colorectalcancer(CRC)isthethirdcauseofdeathsrelated tomalignantdiseasesallovertheworld1anditisthefourth
leadingcauseinBrazil.1,2In2012,CRCfrequencyreachedout
29,870cases.AccordingtoBrazilian’sCancerNational Insti-tute (Instituto Nacional do Câncer – INCA),3 in south region,
CRCcan befoundin 20.4and 21.8 per thousandmenand women respectively.3 The prevalence is higher for people
among60–79yearsandalsoforfemalesex.2,3InBrazil,
rec-ommendationsofthegovernmentalpublichealthinstitution (MinistériodaSaúde)preconizescreeningstrategiesusingfecal occultbloodtestinindividualsfrom50to75years,followed bysigmoidoscopyorcolonoscopyifthefirsttestispositive. Colonoscopy isthe gold-standard for CRC due to its cost-effectiveness.4
Colorectalpolypsare projectionsin largebowel mucosa and can be either neoplastic or not. Neoplastic polyps areadenomasandcarcinomas,whilenon-neoplasticpolyps are hamartomas, inflammatory, hyperplasic or metaplas-tic polyps.2,5 The adenoma histological type increases 2–3
timesthe risk ofCRC development.Itis possibletoresect polyps before its malignization. This procedure decreases morbimortality rates for CRC and increases to 90% the five-year survival rate.4 According to the National Polyp
Study, after an adenoma resection, the recurrence risk is 32–41.7%.1
Inthis study,weanalyzedthepathological reportsfrom polypectomiesinaLaboratoryofPathologyinCuritiba,Brazil, in 2013. The aim was to establish the frequency of pre-malignant and malignant lesions and correlate them with patientdemographicalinformation(ageandgender),aswell aswiththefindingsofthelesionitself,suchaslocalization, morphologicalandhistologicaltypeandpresenceof dyspla-sia.
Methods
Positivo University Ethics Committee approved the
research and the protocol number of the approval is 28872014.7.0000.0093. This study analyzed exclusively medical reports and was exempted of Free and Informed ConsentTerm,ensuringdataconfidentiality.
Allpatientsincludedwerefromoutpatientclinics submit-tedtoretosigmoidoscopyorcolonoscopyinthisperiod.
Thereportsstandardizationwasbasedonthe Histopatho-logical Reports Patterning Manual (Manual de Padronizac¸ão Histopatológica)fromBrazilianSocietyofPathology,4thedition (2015).Reportswithoutenoughinformationaboutage,sexor polyplocationwereexcluded.
Data were organized in spreadsheets using Excel
(Microsoft®). For statistical analysis Graph Pad Prism 5.0 was used. Statistical significance level adopted was 5% (p≤0.05), applyingFisherand Chisquareteststoassociate nominal variables and Mann–Whitney or T student test for continuousvariables.
Results
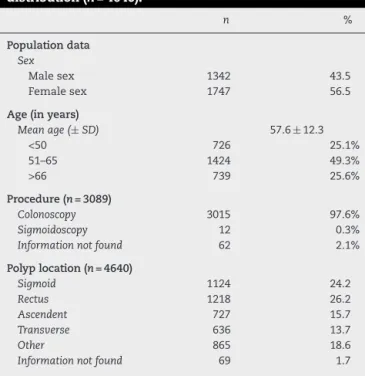
Threethousandandeightyninepolypectomies histopatho-logical reports were analyzed, totaling 4640 polyps. The averagenumber ofpolypsforeachpatientwas1.5. Popula-tiondata(n=3089)andpolyps(n=4640)locationdistribution areshowninTable1.Womenpresentedhigherfrequencyof polypsthanmen(p<0.001).
Histologicaltypesandpresenceofdysplasiaareshownin
Table2.Adenomatouspolypsrepresented75.1%ofallcases.
Malignantcasesrepresented2.1%(n=100),dividedin:92cases ofadenocarcinoma,8casesofcarcinoma,which 5casesof small-cellcarcinoma,2casesofmucinouscarcinomaand1 caseofsquamous-cellcarcinoma.
Themainlocationforadenocarcinomacaseswassigmoid (35%),followedbyrectus(29.9%).Themeanagewas62.3±11.4 years.Stillforadenocarcinomacases,64.1% wereclassified aslowgrade/welldifferentiatedand29.3%asinvasive.These itemsareincludesinTable3.
Agegroupsdistribution, mostfrequentlocationand sex proportionforadenocarcinomacasesareshowninTable4.
Table1–Populationdata(n=3089)andpolypslocation
distribution(n=4640).
n %
Populationdata Sex
Malesex 1342 43.5
Femalesex 1747 56.5
Age(inyears)
Meanage(±SD) 57.6±12.3
<50 726 25.1%
51–65 1424 49.3%
>66 739 25.6%
Procedure(n=3089)
Colonoscopy 3015 97.6%
Sigmoidoscopy 12 0.3%
Informationnotfound 62 2.1%
Polyplocation(n=4640)
Sigmoid 1124 24.2
Rectus 1218 26.2
Ascendent 727 15.7
Transverse 636 13.7
Other 865 18.6
Informationnotfound 69 1.7
Table2–Histologicaltypesinallpolypsstudied.
n %
Hystologicaltype
Hyperplasic 900 19.4
Inflammatory 87 1.9
Lymphoid 27 0.6
Adenoma 3488 75.1
Malignanta 100 2.15
Hystologicalsubtypesforadenomas % Presenceof dysplasia
Tubular 74.2% 5.3%
Tubulo-villous 3.7% 61.5%
Villous 0.4% 76.9%
Serrated 21.7% 0.2%
Dysplasiadegree(foradenomasonly)
Lowdegree 93.4%
Highdegree 6.6%
a Amongthemalignantcases:92adenocarcinomas,8carcinomas
(5small-cellcarcinoma,2mucinouscarcinomaand1 squamous-cellcarcinoma).
Table3–Detailedinformationaboutalladenocarcinoma (n=92)foundinthestudy.
Information n (%)
Malesex 42 50.5
Femalesex 40 49.5
Meanage(years) 62.3±11.4
Location
Sigmoid 34 35
Rectus 29 29.9
Ascending 10 10.3
Transverse 6 6.1
Other 16 16.4
Informationnotfound 2 2.2
Differentiationgrades
Lowgrade/welldifferentiated 60 65.2 Moderatelydifferentiated 29 31.5 Highgrade/poorlydifferentiated 2 2.2 Informationnotfound 1 1.1
Invasion
Invasive 27 29.3
Intramucosal 34 36.9
Insitu 15 16.3
Informationnotfound 16 17.5
Table4–Agegroupsdistribution,mostfrequentlocation esexproportioninadenocarcinomacases.
Age(inyears) Women Men Location(most frequent)
≤50(n=13) 9(20.9%) 4(8.1%) Sigmoid(46.1%) 51–65(n=39) 16(37.2%) 23(46.8%) Sigmoid(43.5%) >66(n=40) 18(41.9%) 22(45.1%) Sigmoid(27.5%)
Discussion
AccordingtoINCAdata,inBrazil,theCRCannualincidence
totalizes32,600, andit ismorecommon inwomen.3
advanced stage of disease. However, CRC is a preventable disorder.Screeningstrategiesforhigh-riskpopulation have beenrelevanttodecrease mortality.Detectionand removal of polyps are important preventive actions before malig-nancy,sincesometumorsemergeaspolyplesionsatfirst.3
Histological study must be performed in order to provide epidemiologicalinformation,thusnewpreventivestrategies could be developed and managed in different geographic regions.Inthisresearch,histologicalreportsfromcolorectal polypswereanalyzedduringtwelvemonthsinasingle Pathol-ogyLaboratoryinCuritiba-PR.
Inthisstudy,polypsweremorefrequentinwomen, like-wisepreviousresearches.6–8 Themeanagefoundwaslower
thantheoneshowedinnationalliterature.Almostonethirdof polypswereobservedinpeopleyoungerthan65years.Valarini etal.8analyzed444casesinCuritibaandrelatedameanageof
58(±12.1years).Amongadenocarcinomacases,themeanage washigher,with62.3(±11.4years).Themeanagegroupwas 50–65years-old.Adenocarcinomawasequallyfoundinmen andwomenandthisdatadiffersfromliterature,sinceCRCis morefrequentinfemalesex.5
Polypremovalwasperformedbycolonoscopyin97.6%of thecases,showingthatthisprocedureispreferredinstead, accordingtonationalrecommendations.5 Polypectomy
per-formedby this procedure can decrease in 76–90%the risk ofCRC,inallstagesofitsdevelopment,beinganimportant preventiveactionforprecursorlesions.5,9
Themostfrequentlocationwas rectus, followedby sig-moid. However, Santos and cols (2008, n=1579)10 showed
ascendingcolonasamorefrequentlocationforthislesions. In the present study, more than two thirds of all cases wererelatedasadenomahistologicaltype.Santosandcols presented the adenoma histological type in 47.3%. Low degreedysplasiawasdescribed in93.4%ofthecasesinour sample.
Amongadenoma,themostfrequenttypewasthetubular. Whencomparedtoothernationalstudies,8,10inourstudywas
foundahigher frequencyofadenomatous polyps’serrated type(21.7%).Serratedtyperepresentsagroupofpolypswith severalrecentlyrecognizedsubtypesassociatedtodifferent colonoscopicappearance,histology,molecularalterationand riskofprogressiontomalignancy.11Managementofpatients
with these polyps depends on understanding their natu-ralhistory,especiallythetransitiontomalignancy.Thereis evidencethat these lesions are associatedwithCRC, how-ever, prospective studies are needed to assess the risk of CRC inpatients diagnosedwith serrated polyp.11 However,
regardless of the histological type identified, according to the National Polyp Study,1 adenomatous polyps should be
monitored.
Malignpolypswerefoundin2.1%cases.Thisfrequency iswithinthestandardforthisgeographicregion.11,12Among
them, 65% were described in rectus and sigmoid. Most of themwerewell-differentiatedandlowdegree;nevertheless, invasivetumorsrepresented29.3%.Similarratesfor adeno-carcinomainpolypsweredescribedinotherstudiesinBrazil’s southregion(2.66%and2.1%).11,12Inourstudy,5cases(0.1%)
werealsodiagnosedas polypsclassified assmall-celltype, allinwomen.Small-cellcarcinomasaremalignanciesderived fromcellsoftheneuroendocrinesystem.Colorectalsmall-cell
carcinomaisararetumoranditsincidenceislessthan0.2% amongallkindsofCRCs.13
A limitation of our study was lack ofclinical informa-tion concerning our patients, since only histopathological reportswereanalyzed.Wecouldnotreachtheclinical indica-tionfortheprocedure(colonoscopyorpolypectomy)foreach patient.
In conclusion, this present study analyzed histological findings inpolypectomiesmedicalreports. Itwasobserved that polypswere more frequentin women, although ade-nocarcinoma caseswere distributed equallyin bothsexes. In addition, the mean age of people submitted to the procedure (colonoscopy/polypectomy)isdecreasing.Beyond that, themostfrequentlocationforpolypswasrectus, fol-lowed bysigmoid. Adenoma typewas foundin twothirds of all cases, and the tubular subtype was the most fre-quent. Besides, adenocarcinoma represented 2.1% of all cases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BondJH.Polypguideline:diagnosis,treatment,and
surveillanceforpatientswithcolorectalpolyps.AmJ
Gastroenterol.2000;95:3053–63.
2.NetoJRT,AricieriJS,TeixeiraFR.Aspectosepidemiológicos
dospóliposelesõesplano-elevadascolorretais.RevBras
Coloproct.2010;30:419–29.
3.MinistériodaSaúde.InstitutoNacionaldoCâncerJosé AlencarGomesdaSilva.RiodeJaneiro:1996–2013.Available
in:http://www.inca.gov.br/.
4.RostirollaRA,Pereira-LimaJC,TeixeiraCR,SchuchAW,
PerazzoliC,SaulC.Desenvolvimentode
neoplasias/adenomasavanc¸adoscolorretaisnoseguimentoa
longoprazodepacientessubmetidosacolonoscopiacom
polipectomia.ArqGastroenterol.2009;46:167–72.
5.ParadaAA,ProjetoDiretrizes.RastreamentoeVigilânciado
CâncerColo-retal.Prevenc¸ãosecundáriaedetecc¸ãoprecoce.
SociedadeBrasileiradeEndoscopiaDigestiva;2008.
p.1–34.
6.HossneRS,MaranhãoMF,CarvalhoFA,MendesFG.Estudo
retrospectivodoresultadoanatomopatológicode100
polipectomiascolonoscópicasrealizadasnaFMB-UNESP.Rev
BrasColoproct.2007;27:251–5.
7.RochaBP,FerrariAP,ForonesNM.Frequênciadepóliposem
doentesoperadosdecâncercolorretal.ArqGastroenterol.
2000;37:31–4.
8.ValariniSBM,BortoliVT,WassanoNS,PukanskiMF,MaggiDC,
BertolloLA.Correlationbetweenlocation,sizeandhistologic
typeofcolorectalpolypsatthepresenceofdysplasiaand
adenocarcinoma.JColoproctol.2011;31:241–7.
9.BeckerF,NuskoG,WelkeJ,HahnEG,MansmannU.Follow-up
aftercolorectalpolypectomy:abenefit-riskanalysisof
Germansurveillancerecommendations.IntJColorectalDis.
2007;22:929–39.
10.SantosJM,FelícioF,LyraJHF,MartinsMRC,CardosoFB.
Análisedospóliposcolorretaisem3.491videocolonoscopias.
RevbrasColoproctol.2008;28:299–305.
11.RostyC,HewettDG,BrownIS,LeggettBA,WhitehallVLJ.
ofdiagnosis,pathogenesis,andclinicalmanagement.J
Gastroenterol.2013;48:287–302.
12.SimunicM,PerkovicN,Rosic-DespalatovicB,TonkicA,
ArdalicZ,TitlicM,etal.Colonoscopicpolypectomiesand
recommendationsonthecolonoscopyfollow-upintervals
dependingonendoscopicandhistopathologicalfindings.
ActaInformMed.2013;21:166–9.
13.YazijiH,BroghamerWLJr.Primarysmallcellundifferentiated
carcinomaoftherectumassociatedwithulcerativecolitis.