www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Canine
fossa
puncture
in
endoscopic
sinus
surgery:
report
of
two
cases
夽
Federico
Sireci
a,∗,
Matteo
Nicolotti
b,
Paolo
Battaglia
c,
Raffaele
Sorrentino
b,
Paolo
Castelnuovo
c,
Frank
Rikki
Canevari
baUniversityofPalermo,DepartmentofExperimentalBiomedicineandClinicalNeurosciences(BioNeC),Otorhinolaryngology
Section,Palermo,Italy
bSSAntonioBiagioeCesareArrigoHospital,OtorinolaryngologySection,Alessandria,Italy cUniversityofInsubria,DepartmentofOtorhinolaryngology,Varese,Italy
Received17November2016;accepted1March2017 Availableonline22March2017
KEYWORDS
Caninefossa puncture; Middlemeatal antrostomy; Maxillarysinusitis; Angledmicrodebrider
Abstract
Introduction:Chronicrhinosinusitiswithnasalpolyposisisacommonchronicdiseasethatoften affectsmaxillarysinus.Endoscopicsinussurgeryisthemostcommonprocedurefortreatingthe majorityofmaxillarysinuslesions.
Objective:Todemonstratetheroleofcaninefossa punctureduringendoscopicsinussurgery procedureinpatientswithseveremaxillarysinusdisease.
Methods:Wepresent2caseswherecaninefossapuncturehasbeenperformedasmethodto obtainacompleteaccesstothemaxillaryantrum.
Results:Accordingourexperience,2caseson296endoscopicsinussurgery(0.6%)where antros-tomyandusedofangledmicrodebriderwerenotsufficient,caninefossapuncturehasbeen performedasanalternativemethodtoobtainacompleteaccesstothemaxillaryantrum.
Conclusion:Althoughtheadventofendoscopicsinussurgery,ourcasessupportthefactthat actuallycaninefossapunctureisaminimallyinvasivetechniqueusefulinselectedcases. © 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:SireciF,NicolottiM,BattagliaP,SorrentinoR,CastelnuovoP,CanevariFR.Caninefossapunctureinendoscopic sinussurgery:reportoftwocases.BrazJOtorhinolaryngol.2017;83:594---9.
∗Correspondingauthor.
E-mail:[email protected](F.Sireci).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2017.03.001
PALAVRAS-CHAVE
Punc¸ãodafossa canina;
Antrostomiameatal média;
Sinusitemaxilar; Microdebridador angular
Punc¸ãodafossacaninaemcirurgiaendoscópicasinusal:relatodedoiscasos
Resumo
Introduc¸ão: Arinossinusitecrônicacompoliposenasaléumadoenc¸acrônicacomumque fre-quentementeafetaoseiomaxilar.Acirurgiaendoscópicasinusaléoprocedimentomaiscomum paratrataramaioriadaslesõesdoseiomaxilar.
Objetivo: Demonstraropapeldapunc¸ãodafossacaninaduranteoprocedimentodecirurgia endoscópicasinusalempacientescomdoenc¸agravedoseiomaxilar.
Método: Apresentamos2casosemqueapunc¸ãodafossa caninafoirealizadacomométodo paraobteracessocompletoaoantromaxilar.
Resultados: Deacordo comnossaexperiência, 2casos em 296 cirurgia endoscópicasinusal (0,6%)ondeantrostomiaeousodemicrodebridadorangularnãoforamsuficientes,apunc¸ão dafossacaninafoirealizadacomoummétodoalternativoparaobteracessocompletoaoantro maxilar.
Conclusão:Apesardoadventodacirurgiaendoscópicasinusal,osnossoscasosapoiamofatode queapunc¸ãodafossacaninaéumatécnicaminimamenteinvasivaútilemcasosselecionados. © 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Chronic rhinosinusitis(CRS) with nasal polyposis(NP) is a commonchronicdiseasethatseriouslyaffectsthequalityof life.1Obliterationoftheostiomeatalunitisthemost
com-monfactorinfluencingthepathogenesisofthisinflammatory process.2 Endoscopicsinus surgery (ESS)is the most
com-monprocedurefortreatingCRSthatisrefractorytomedical treatment.
Although themajority ofmaxillarysinus lesionscan be removed through the widened natural ostium performing partialuncinectomyandmiddlemeatalantrostomy(MMA), somepatientshaveextensivediseasethatisdifficultto han-dlepurelyendoscopically.
In fact endoscopicaccessby natural ostium onlyallow toclearthe posteriorlateralwall, theposteriorregionof theroof,andtheposteriorwallofthemaxillarysinusbut noanteriorandinferiorregions.Failuretoremovemassive polyposis and fungal debrisfrom the maxillary sinus may resultinanearlypostoperativerecurrenceofsymptomsand diseaseforthepatient.3
One solution is the traditional Caldwell Luc approach performed through the anterior wall of the maxillary sinus. This is, however, associated with significant mor-bidity such as facial numbness or paresthesia (9%) for damage of the infraorbital and anterior superior alveolar nerves, oroantralfistulas (1%),gingivolabial wound dehis-cences (1.5%), and dacryocystitis (2.5%). This technique has been superseded by endoscopic medial maxillectomy useful totreat benigntumors,not inflammatorydisease.4
Canine fossa puncture (CFP) has been proposed as an alternative method of obtaining access to the maxillary antrum.
Although afewstudieshave demonstratedthebenefits of CFPin management of theseverely diseased maxillary sinus,theefficacyandsuperiorityofthismethodcompared withconventionalMMArequirefurtherinvestigation.5
The aimof thisstudy is toreview theliterature about theindicationsofCFPinpatientswithseveremaxillarysinus diseaseandcomparethissurgicalprocedurewithmaxillary sinusclearancethroughMMA.
Presentation
of
cases
series
Wereviewedall endoscopicsinussurgery(ESS) performed atourdepartmentin2015.Atotalof296endoscopicsinus surgerieswereperformedduringthisperiod.Ofthese, com-binedapproachendoscopic sinussurgery andcaninefossa puncture(CFP)wasperformedin2(0.6%)caseswhenthere wasdifficultyinvisualizationandclearanceofdisease.
Inparticular,CFPconsistinatrocarplacedinthecanine fossa.Thelandmarksincanineapproachare:themid pupil-larylineandhorizontallinerunningalongthelowerborder ofnasalala andlateralaspect ofcaninefossa highabove the3rdand4thteeth(canineandpremolar),inferolateral toinfraorbitalforamen.Thetrocarshouldbeaimedtoward the maxillo ethmoidangle toavoid pterygopalatine fossa andorbitallesions.Inmostpatientsthetrocarwasinserted usingagentletwistingmotion.Insomepatientswiththicker bone,gentletapping withahammerwasrequired forthe trocartobeinserted.6,7Afterremovalofthetrocara4mm
microdebriderblade wasplaced throughthe passage cre-atedbythetrocar.Themicrodebriderbladewasvisualized inthemaxillarysinuswitha40◦ or70◦ endoscopeviathe
middlemeatalantrostomy.Polypsanddiseasedtissuecanbe removedfromthemaxillarysinususingthemicrodebrider. Bothcases treated by CFP resulted free of complications aftersurgeryandfreeofdiseaseduringfollow-up.
Case1
BE
a
b
d
c
A
AP
AP MT
NS
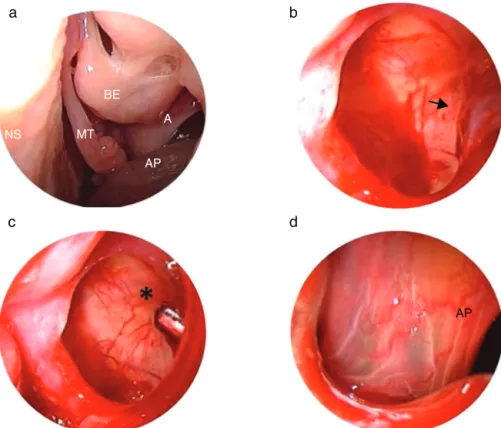
Figure1 (a)Antrochoanalpolypemergingfromthemiddleantrostomyoftheleft maxillarysinusisnotedontheendoscopic examination.(b)Thebaseofthepolyp(blackarrow)ontheanteriorwallofthemaxillarysinusviewedusing45◦endoscope.(c) Microbedrider(asterisk)introducedinsidethemaxillarysinusbythetrocarviewedusing45◦endoscope.(d)Polypviewedbytrocar using0◦endoscope.AP,antrochoanalpolyp;A,antrostomy;MT,middleturbinate;NS,nasalseptum;BE,bullaethmoidalis.
consumption. She reported paracetamol and dried fruit allergy. Three years ago, underwent to functional endo-scopicsinussurgery(FESS)forpresenceofleftantrochoanal polyp.Since3months,shecomplainedaleftnasal obstruc-tion without other symptoms. Therefore, she has been subjected to nasal endoscopy that evidenced a presence of left antrochoanal polyp (Fig. 1) confirmed at cranio-facial computerized tomography (CT). In August 2015 a revision FESS was performed. Due to the fact that polyp implantwasinanteriorregionofmaxillarysinus,acanine fossa puncturewas performed, despite the use of curved blades.Thenasalpackwasremovedthedayafterandthe patientdischarged.Sevendaysofantibioticstherapy amoxi-cillin/clavulanatecombinationandsalinnasalirrigationwas
recommended.Thepatientunderwentnewexaminationat 6monthsremainingfreeofdisease.
Case2
A77-year-oldCaucasianwomanwasadmittedtoour Depart-mentbecauseofleftpurulentrhinorrheaandparesthesiain left maxillaregion since 3 months.She was subjected to dentalimplantonleftmaxillaarchinMarch2015.Herpast medicalhistorywasremarkable;shehadapositiveremote historyforchroniclymphoblasticleukemiaBcellresolved, splenectomy performed for spontaneous splenic rupture, hysterectomyandatrialfibrillation.Ananteriorrhinoscopy
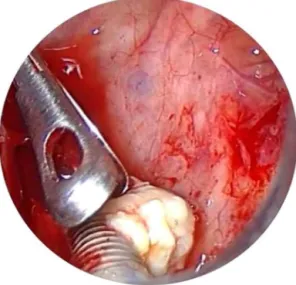
Figure3 Dentalimplantviewbytrocarusing0◦endoscope.
displayedthepresenceofpusfillinghiswholenasalcavity, whichwasoriginatingfromtheostio-meatalcomplex. Dur-ingoralevaluationanoro-antralfistulawasdetectedatthe siteofpreviousdentalextraction.CTscanwithoutcontrast enhancementwasperformedandshowedcomplete opacifi-cationoftheleftmaxillarysinusandaninterruptionofsinus floorcorrespondingtoalveolarprocesswithdentalimplant insidesinus(Figs.2and3).
In April2015patientwassubjectedtoMMAinorderto removedentalimplantsbuttheprocedurecouldnotbe com-pletedtransnasallyneitherwiththeuseofcurvedbladeso a CFPwas required in order toremove the foreignbody. Nasalpackingwasremoved1daypostoperatively,andthe patientwasdischarged.Aftersurgery,weprescribedsaline irrigationandparacetamol.Patienthasbeenvisitedinour sectionat10days,thenat4weeksandfinallyat6months. Meticulous endoscopic dressing and saline irrigation were performed untilthe cavitywashealed. To date patientis freeofdisease.
Discussion
Nowadays middle meatal antrostomy (MMA) is considered thegoldstandardIthetreatmentofmaxillarysinusitis. Any-way critical areas such as inferior, lateral, anterior wall, recessus zygomaticusandrecessus alveolarisandrecessus prelacrimalis of maxillary sinus are difficult to approach. Forthisreasonmedialmaxillectomyorexternalapproaches suchasCaldwellLucapproachorCFParerequired.6
TheefficacyofthismaneuverontheoutcomeafterFESS has been the subject of a small number of studies. Lee et al. have compared the results of performing a canine fossapuncturewithclearanceofpolypsviaamiddlemeatal antrostomy.Nobenefitof thecaninefossaprocedureover conventionalmiddle meatalantrostomywasseenafter 12 monthsfollowup,howeverseriesaresmallinbothgroups (11CFPvs.13MMA).Theauthorsconcludedthatalthough canine fossa puncture is a useful method for removing severemucosaldiseasethatcannotbereachedthroughthe MMA,itdoesnotguaranteeabettersubjectiveorobjective surgicaloutcomeinpatientswithnasalpolyposis.7However,
Seiberlingetal. inacase controlstudies havefound that patients with the same disease who had a canine fossa puncturehadabetteroutcomethanthosewhodidnot.In fact, all patients were administered the chronic sinusitis survey(CSS)that evidenced a subscore better in the CFP group(Mann---Whitneytest,p=0.02).8
Manyauthorsstudiedthemaxillarysinus areaexplored byendoscopy.
Beswicketal.quantifiedthemaxillarysinusvolumeand mucosalsurfacearea(SA)thatisaccessibleendoscopically viaamiddlemeatalantrostomyineightcadaver maxillary sinusesconfiguredwithimageguidancesoftware.In partic-ularthe authors demonstrated that mean maxillary sinus volumewas16.5±2.5cm3andmeanSAwas31.0±2.3cm2.
The15◦,40◦,70◦and120◦microdebridersaccessedan
aver-ageof10%,25%,41%,and66%,respectively,oftheSA,and of2%,9%,17%,and36%,respectively,ofthevolume.There wasa trendtoward improvedaccessibilityof thesuperior half versus the inferior half of the maxillarysinus. When instruments of different degrees were combinedto max-imize accessibility, 81% of the SA of the sinus could be accessed.Howeverauthorsdidnotquantifyvolumeandarea ofmaxillarysinusexposed.9
Feldtetal.inasampleofcadaversshowedthata signif-icantgreateramountofdebriswasleftafterthetransnasal endoscopictechnique(TN)approachcomparedwithcanine fossatrephination(CFT)(3.88cm3vs.2.88cm3,p=0.015).
MedianbladeutilizationwassignificantlyhigherwiththeTN approachvs.CFT(4vs.1,p<0.002).
Our experience demonstrated as, although using new curvedblades,criticalareassuchasantero-medialportion of MS cannot be reached and treated by antrostomy and therefore CFP has to be performed. According to litera-ture,we performed CFPonly in unilateral lesions.Infact Byunetal. assignedrandomlytwelvepatients tothe CFP and thirteen to MMA groups who completed the follow-up, questionnaires (SNOT-20 and VAS), and postoperative CT evaluation. SNOT-20 and VAS scores improved signifi-cantlyat3,6,and12monthspostprocedureinbothgroups. However,significantimprovementofSNOT-20at12months andVASscoresforpurulentdischarge,foulodor,and post-nasaldrip at 6 and 12 months were observed in the CFP groupcomparedwiththeMMAgroup.PostoperativeCTscan evidencedthatthe volumeof mucosalthickeningwas sig-nificantlygreaterintheMMAgroupthanintheCFPgroup. Inaddition,CFPwasnoteffectiveinpatientswithbilateral CRS anddiffuse NP but provided better managementand subjectiveandobjectivesurgicaloutcomesinpatientswith unilateralCRSaccompanyingNP.AmongunilateralNP,there isanthrocoanalpolyps(ACP).
ACPisrelativelyunusualinthesinonasaltract.Itoccurs predominantlyinchildren andyoungadultsandoriginates fromthemaxillaryantrumwithextensionintothe nasopha-rynxororopharynx.Simpleexcisionofthepolypvialimited surgicalprocedures suchassimple polypectomyresults in highrecurrencerates.Completeremovalofthepolypinthe antrum,includingitssiteoforigin,isessentialtominimize recurrence.However,abroadbasesuchasalateral,inferior, oranteriorlocationofthepolypmakeseradicationdifficult viaaMMA.Inthissituation,someauthorschoosethe tradi-tionalCaldwell-Lucoperation,eveninchildren.10However,
numbness,facialswelling,riskforinjuryofthetoothbuds and roots, and possible asymmetric facialgrowth, makes itlessfavorablethanendoscopicsinussurgery.Infact,we preferred CFP as alternative method of accessing almost theentiremaxillaryantruminyoung/adultpopulation.Few studieshave reportedthe efficacyofthe CFPapproachin treatingACPinthepediatricpopulation(≤15yearsold)and thelong-termeffectonchangesinthemaxillarysinus vol-umeand surgical outcome hasnot been determined.Jae YongLeeetal.studiedalittlesampleofsevenpatientswith ACPremovedviatheCFPapproach.Afterameanfollow-up periodof43.9months,theauthorscomparedthechangesin themaxillarysinusvolumebetweentheoperatedand nor-mal sides, using the pre- and postoperative CT data. No contracturesor decreaseinthemaxillarysinus volumeon thediseasedsidewereobserved inanyofthepatients on postoperativeCT.Noneofthepatientsshowedevidenceof recurrenceontheendoscopicandCTexaminationsandonly twopatientscomplainedofmildfacialswellingandtingling sensation,whichresolvedspontaneouslywithin2weeks.11
ThereforeCFPcanbeperformedtotreatACPinyoungbut alsoinchildrenwhenMMAisnotsufficient.
Important indications to CFP are chronic odontogenic sinusitis(COS).Approximately5---15%ofthepopulation suf-fersfromchronicrhinosinusitis,andin10---12%ofthem,itis ofdentalorigin.12Itisproducedbyperiapicalgranulomasor
smallinflammatorycystsofthemolarsorbicuspids,chronic oroantralfistula(OAF),largeodontogeniccystsoccupyinga greatpartofthemaxillarysinus,andforeignbodies(dental fillings,teethroots,andimplants)pressedthroughoutthe rootcanalorfistulaintotheantrum.Weshowedacaseof implantmigrateinleftmaxillarysinusnotaccessiblefrom antrostomybycurvedinstrumentsbecauseplacedinmedial wallofmaxillarysinus.
Venetis et al. presented 20 cases with odontogenic sinusitis, 5 (25%) in which a foreign body was removed from maxillary sinus by combined transnasal and canine fossa endoscopic approach. The surgical procedure was performed withconventional instrumentation throughthe widenedantrorhinostomyorthroughabonywindowatthe anteriorsinus wall.Attheendof theprocedure,the win-dow was repositioned and stabilized with two to three absorbablesutures.Intwocases,withsizeableforeign bod-ies,thepreservation of thebony windowwasimpossible, andamodifiedCaldwell---Lucoperationwasperformedwith preservation of the healthy sinus mucosa.13 According to
Barziliaietal.weavoidCaldwell---Lucoperationbecauseit isassociatedwithsignificantmorbiditysuchasfacial numb-nessorparesthesia(9%)fordamageoftheinfraorbitaland anterior superior alveolar nerves, oroantral fistulas (1%), gingivolabialwound dehiscences(1.5%),anddacryocystitis (2.5%).14ActuallyCaldwell-Lucprocedureisrationalincases
offungaldiseaseandinendoscopicmedialmaxillectomyfor treatinginvertedpapilloma.Infactinourcase,awideMMA combinedwithCFPwasenoughtoremovedentalimplant.
Inliterature,differentopinionsaboutapproachtofungal maxillarsinusitis arereported.We didnot showany case of CFP in fungal disease because in most of the patients it can beremoved throughthe MMA using various curved instruments and saline irrigation without great difficulty. Also, if fungal invasion into sinus tissue is confirmed by histologicalexamination, a systemic antifungal treatment
postoperativelyisparamounttoreducediseaseand poten-tialrecurrences.15
InsteadtherearenoindicationstoperformCFPand/or Caldwell-Luc approachin maxillar sinus malignant tumor. According to literature, endoscopic medial maxillectomy canbeconsideredasfirstchoiceindifficultmaxillarysinus tumor removalbecause an unnatural opening like CFAor Caldwell Luc in locally invasive disease with malignant potentialasthetumorcanextendthroughthisopening in recurrentcases.16
Conclusions
Although the advent of ESS, our cases support the fact that actually canine fossa puncture is a minimally inva-sive technique useful in selected cases. In fact, only in 0.6%ofcasesweusedthistechniquewithoutpostoperative complications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FokkensW,LundV,BachertC,ClementP,HelllingsP,Holmstrom M,etal.EAACIpositionpaperonrhinosinusitisandnasalpolyps executivesummary.Allergy.2005;60:583---601.
2.ByunJY, Lee JY.Canine fossa puncture for severemaxillary diseaseinunilateralchronicsinusitiswithnasalpolyp. Laryn-goscope.2013;123:79---84.
3.LeeJY,LeeSH,HongHS,LeeJD,ChoSH.Isthecaninefossa punctureapproachreallynecessaryfortheseverelydiseased maxillarysinusduringendoscopicsinussurgery.Laryngoscope. 2008;118:1082---7.
4.DeFreitasJ,LucenteFE.TheCaldwell-Lucprocedure: institu-tionalreviewof670cases.Laryngoscope.1988;98:1297---300. 5.SathanantharS,NagaonkarS,PaleriV,LeT,RobinsonS,Wormald
PJ. Canine fossa puncture and clearance of the maxillary sinusfortheseverelydiseasedmaxillarysinus.Laryngoscope. 2005;115:1026---9.
6.AnandV,SantoshS,AishwaryaA.Canine fossaapproachesin endoscopicsinussurgery---ourexperience.IndianJOtolaryngol HeadNeckSurg.2008;60:214---7.
7.Petersen RJ. Canine fossa puncture. Laryngoscope. 1973;83:369---71.
8.Seiberling K, Ooi E, Miin Yip J, Wormald PJ. Canine fossa trephinefortheseverelydiseasedmaxillarysinus.AmJRhinol Allergy.2009;23:615---8.
9.BeswickDM,RodriguezKD,OldsCE,KassJI,SchaitkinBM. Quan-tificationofmaxillary sinusaccessibility viaa middlemeatal antrostomy.AmJRhinolAllergy.2015;29:394---6.
10.Myers EN, Cunningham MJ. Modified Caldwell-Luc approach for the treatment of antral choanal polyps. Laryngoscope. 1986;96:911---3.
11.LeeJY,BaekBJ,KimDW,ByunJY,LeeSW,HongHS.Changes inthemaxillarysinusvolumeandthesurgicaloutcomeafter thecaninefossapunctureapproachinpediatricpatientswith anantrochoanalpolyp:resultsofaminimum3-yearfollow-up. AmJRhinolAllergy.2009;23:531---4.
13.VenetisG, BourlidouE,Liokatis PG,ZouloumisL.Endoscopic assistanceinthediagnosisandtreatmentofodontogenic max-illarysinusdisease.OralMaxillofacSurg.2014;18:207---12. 14.BarzilaiG,GreenbergE,UriN.IndicationsfortheCaldwell-Luc
approachintheendoscopicera.OtolaryngolHeadNeckSurg. 2005;132:219---20.
15.PagellaF,MattiE,GiourgosG,ColomboA,DeBernardiF, Castel-nuovoP.Iscaninefossaaccessnecessaryforsuccessfulmaxillary fungusballtreatment.Rhinology.2009;47:385---8.