rev bras hematol hemoter. 2017;39(2):180–182
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Letter
to
the
Editor
Presence
of
atypical
beta
globin
(
HBB
)
gene
cluster
haplotypes
in
sickle
cell
anemia
patients
of
India
DearEditor,
Sickle cell disease (SCD)is anautosomal recessive disease causedbyatransversiontypeofpointmutationinthebeta globin (HBB) gene. Sickle cell anemia in India is common amongtheethnicpopulationgroupswiththehighest preva-lencebeingseenamongthecasteandtribalpopulationsof CentralandSouthIndia.1TheHBBgeneclusterincludesthe embryonicεgene,thetwofetalglobingenesGandA,a pseudo-gene,theıgeneandfinallytheHBBgeneitself.The
HBBgeneclusterislocatedontheshortarm(p)ofchromosome 11andspansaregionof70kilobases.Identificationof poly-morphicrestrictionendonucleases sitesin andaround the
HBBgenehasledtothedelineationofthefiveHBBgenecluster haplotypesofsicklecellanemia.2Thesehaplotypesofsickle cellanemiaareimportantaspopulationdata,for anthropo-logicalpurposestotracethemigrationofthesicklecellgene andtomonitortheclinicalseverityofthedisease.3Giventhe factthattherearesignificantdifferencesintheclinicaland hematologicalvariables amongpopulations,it isimportant to characterize haplotypes to understand the clinical and phenotypicheterogeneityofthisdevastatingdisease.Hence, thepresentstudyisaimedatdeterminingtheprevalenceof
HBBgeneclusterhaplotypesintheChhattisgarhpopulation. One hundred unrelated random SCD-hemoglobin (Hb) SS patients (56males and 44 females)receiving treatment in the outpatient department of the Sickle Cell Institute, Chhattisgarh,Raipur,wereenrolled.TheInstitutionalEthics Committeeof Pandit Jawahar Lal Nehru Memorial Medical College,Raipur, approvedthe study.Informed written con-sent was obtained from study participants. A 3mL blood samplewascollectedinvacutainers containing ethylenedi-aminetetraacetic acid (EDTA).Genomic DNA was extracted using a standard protocol.4 DNA sequences encompassing the relevant HBB gene cluster polymorphic variant sites wereamplifiedbypolymerasechainreaction(PCR) andthe fragments were subjected to restriction fragment length polymorphism (RFLP). Eight RFLP sites (5′ to ,5 5′ to G␥,6 IVSIIG␥,6IVSIIA␥,6 5′,73′,7 5′,8 andIVSII,6)were analyzed to identify five known global HBB haplotypes.
As phase-unknown genotypes were collected, the haplo-typesitesandfrequencieswereestimatedusingmaximum likelihood with an expectation-maximization method in Arlequin 3.5software.Thedescriptive dataare reportedas means±standard deviation(SD).The statisticalanalysisof thestudydatawasperformedusingtheIBMStatistical Pack-agefortheSocialSciences(SPSS)forWindows,Version22.0.
AnalysisofHBBhaplotypesusingPCR-RFLPrevealedfour haplotypes,Arab-Indian(+,+,+,−,+,+,−,+,+),Senegal(−, +, +, −, +, +, +, +, +), Benin (−, −, −, −, −, +, −, +, +) and Bantu/CentralAfricanRepublic(−,−,+,−,−,−,−,+,+).We didnotfindtheCameroonhaplotypeinourstudy subjects. TheArab-Indianhaplotypewasthemostcommonhaplotype (78%)followed byatypical haplotypes(15%).Senegal,Benin andBantuhaplotypeswerefoundin4%,2%and1%ofthese sicklecelldiseasepatients,respectively.Highprevalencesof two atypical haplotypes (+, −, +, −, +, −, +, + and +, +, +,
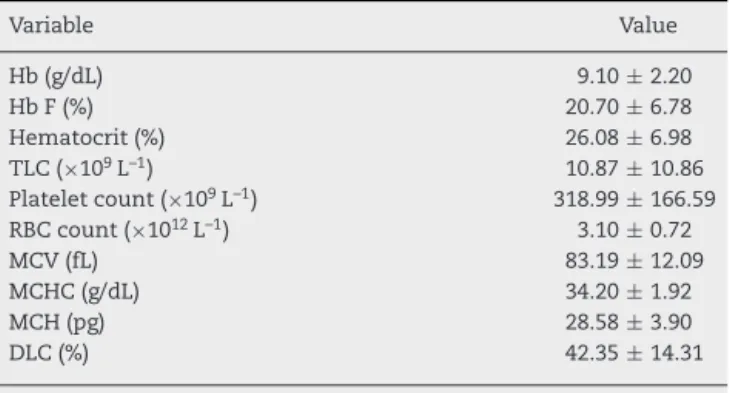
−, +, +, +, +) indicated thatthese haplotypes are common among the samples we examined. Theatypical haplotype structuredetectedinthesamplemighthavebeengenerated througharecombinationprocess.Hematologicalparameters inourstudysubjectsaredocumentedinTable1.Themean hemoglobinconcentrationinthestudygroupisslightlylower thanthenormalrangeof11.0–16.0g/dL.ThemeanHbF con-centration ofthe Arab-Indian haplotypewas 20.70±6.78%, whichissignificantlyhigherthanreportedinpreviousstudies fromIndiaandabroad.9–11
revbrashematolhemoter.2017;39(2):180–182
181
Table1–Hematologicalprofileofstudyparticipants.
Variable Value
Hb(g/dL) 9.10±2.20
HbF(%) 20.70±6.78
Hematocrit(%) 26.08±6.98
TLC(×109L–1) 10.87±10.86
Plateletcount(×109L–1) 318.99±166.59
RBCcount(×1012L–1) 3.10±0.72
MCV(fL) 83.19±12.09
MCHC(g/dL) 34.20±1.92
MCH(pg) 28.58±3.90
DLC(%) 42.35±14.31
Valuesaremeans±standarddeviation.
Hb:hemoglobin;HbF:fetalhemoglobin;TLC:totalleukocytecount; RBC:redbloodcell;MCV:meancorpuscularvolume;MCHC:mean corpuscularhemoglobinconcentration;MCH:mean corpuscular hemoglobin;DLC:differentialleukocytecount.
andinareasofMid-WesternAfrica.16Haplotypesspecificto acertain geographicalregion are suggestive ofthe mutant
HBB gene arising separately in these locations.17 However, severalstudiesreportedthepresenceofSenegal,18Benin,10 Bantu,12andCameroon10haplotypesinIndianpopulations. TheatypicalHBBhaplotypesobservedmighthaveoriginated fromthepre-existingcommon haplotypes,duetoshuffling of pre-existing polymorphisms during meiotic recombina-tion.RearrangementsoftheHBBgeneclusterinapparently typical HBB haplotypes has been demonstrated in several studies.19 Atypical haplotypes have also been reported in several studies.11,12,20 Fifteen atypical haplotypes from 20 differenthaplotypeshavebeenidentifiedinRelliandThurpu KapupopulationsofAndhraPradesh.11
Insummary,theanalysisofhaplotypesrevealedthe pres-enceoffourhaplotypes.Althoughourstudyincludesmore SCDpatientscomparedtopreviousstudies,keepingthe diver-sity of Indian populations in mind, our results should be consideredpreliminary and replicationofhaplotype analy-sisshouldbeperformedinmuchlargersamplesfromother regionsoftheIndiansub-continent.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TheauthorsacknowledgefundingfromtheSickleCell Insti-tute Chhattisgarh, Government of Chhattisgarh, and the Chhattisgarh Council of Science & Technology (CGCOST), Government of Chhattisgarh (Project Ref. No.2740/CCOST/ MRP/2015).
r
e
f
e
r
e
n
c
e
s
1. KateSL,LingojwarDP.Epidemiologyofsicklecelldisorderin thestateofMaharashtra.IntJHumGenet.2002;2(3):161–7.
2.PowarsDR,MeiselmanHJ,FisherTC,HitiA,JohnsonC.Beta-S geneclusterhaplotypesmodulatehematologicand
hemorheologicexpressioninsicklecellanemia.Usein predictingclinicalseverity.AmJPediatrHematolOncol. 1994;16(1):55–61.
3.MakaniJ,WilliamsTN,MarshK.SicklecelldiseaseinAfrica: burdenandresearchpriorities.AnnTropMedParasitol. 2007;101(1):3–14.
4.SambrookJ,RussellD.Molecularcloning.Alaboratory manual.ColdSpringHarborLaboratoryPress;2001.
5.LeeYJ,ParkSS,KimJY,ChoHI.RFLPhaplotypesofbeta-globin genecomplexofbeta-thalassemicchromosomesinKoreans. JKoreanMedSci.2002;17(4):475–8.
6.RahimiZ,KarimiM,HaghshenassM,MeratA.Beta-globin geneclusterhaplotypesinsicklecellpatientsfromsouthwest Iran.AmJHematol.2003;74(3):156–60.
7.FalchiA,GiovannoniL,VaccaL,LatiniV,VonaG,VaresiL. Beta-globingeneclusterhaplotypesassociatedwith beta-thalassemiaonCorsicaisland.AmJHematol. 2005;78(1):27–32.
8.Akhavan-NiakiH,Derakhshandeh-PeykarP,BanihashemiA, MostafazadehA,AsghariB,AhmadifardMR,etal.A comprehensivemolecularcharacterizationofbeta thalassemiainahighlyheterogeneouspopulation.Blood CellsMolDis.2011;47(1):29–32.
9.NgoD,BaeH,SteinbergMH,SebastianiP,SolovieffN,Baldwin CT,etal.Fetalhemoglobininsicklecellanemia:genetic studiesoftheArab-Indianhaplotype.BloodCellsMolDis. 2013;51(1):22–6.
10.BhagatS,PatraPK,ThakurAS.Fetalhaemoglobinand beta-globingeneclusterhaplotypesamongsicklecell patientsinChhattisgarh.JClinDiagnRes.2013;7(2): 269–72.
11.RamanaGV,ChandakGR,SinghL.Sicklecellgenehaplotypes inRelliandThurpuKapupopulationsofAndhraPradesh. HumBiol.2000;72(3):535–40.
12.NiranjanY,ChandakGR,VeerrajuP,SinghL.Someatypical andraresicklecellgenehaplotypesinpopulationsofAndhra Pradesh,India.HumBiol.1999;71(3):333–40.
13.TineRC,NdiayeM,HanssonHH,NdourCT,FayeB,Alifrangis M,etal.Theassociationbetweenmalariaparasitaemia, erythrocytepolymorphisms,malnutritionandanaemiain childrenlessthan10yearsinSenegal:acasecontrolstudy. BMCResNotes.2012;5:565.
14.NagelRL,RanneyHM.Geneticepidemiologyofstructural mutationsofthebeta-globingene.SeminHematol. 1990;27(4):342–59.
15.BitounguiVJ,PuleGD,HanchardN,NgogangJ,WonkamA. Beta-globingenehaplotypesamongCamerooniansand reviewoftheglobaldistribution:isthereacaseforasingle sicklemutationorigininAfrica?OMICS.2015;19(3): 171–9.
16.FlintJ,HardingRM,BoyceAJ,CleggJB.Thepopulation geneticsofthehaemoglobinopathies.Bailliere’sClin Haematol.1998;11(1):1–51.
17.OnerC,DimovskiAJ,OlivieriNF,SchiliroG,CodringtonJF, FattoumS,etal.BetaShaplotypesinvariousworld populations.HumGenet.1992;89(1):99–104.
18.LabieD,SrinivasR,DundaO,DodeC,LapoumeroulieC,Devi V,etal.HaplotypesintribalIndiansbearingthesicklegene: evidencefortheunicentricoriginoftheSmutationandthe unicentricoriginofthetribalpopulationsofIndia.HumBiol. 1989;61(4):79–91.
19.ZagoMA,SilvaWAJr,GualandroS,YokomizuIK,AraujoAG, TavelaMH,etal.Rearrangementsofthebeta-globingene clusterinapparentlytypicalbetaShaplotypes.
182
revbrashematolhemoter.2017;39(2):180–18220.LyraIM,Gonc¸alvesMS,BragaJA,GesteiraMdeF,CarvalhoMH, SaadST,etal.Clinical,hematological,andmolecular characterizationofsicklecellanemiapediatricpatientsfrom twodifferentcitiesinBrazil.CadSaúdePública.
2005;21(4):1287–90.
SandorRudyL.Nongbria,HenuKumarVermab, BhaskarV.K.S.Lakkakulab, PradeepKumarPatraa,∗ aPtJawaharLalNehruMemorialMedicalCollege,Raipur,India bSickleCellInstitute,Chhattisgarh,Raipur,India
∗Corresponding author at: Dept. of Biochemistry, Pt. J.N.M.
MedicalCollege,Raipur,Chattisgarh,India. E-mailaddress:[email protected](P.K.Patra).
Received30September2016 Accepted27January2017 1516-8484/
©2017Associac¸ ˜aoBrasileiradeHematologia,Hemoterapiae TerapiaCelular.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).