jcoloproctol(rioj).2015;35(1):63–66
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Hyperplastic
polyposis:
a
case
report
Thiago
Almeida
Flauzino
a,∗,
Gabriela
N.S.
Fardin
a,
Adriana
F.
Sena
a,
Leonardo
R.F.
Gama
b,
Flávia
L.M.
Ribeiro
a,
Giovanni
J.Z.
Loureiro
a,
Luciano
P.N.
Gama
a,
Rossini
C.
Gama
aaVitóriaApartHospital,Serra,ES,Brazil bGastrenterologist,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20January2014 Accepted11August2014 Availableonline28January2015
Keywords:
Hyperplasticpolyposissyndrome Videolaparoscopiccolectomy Polyposis
a
b
s
t
r
a
c
t
Objective:Theauthorspresentacasereportofhyperplasticpolyposissyndromefromthe ColoproctologyService,VitóriaApartHospital,Vitória-ES.
Casestudy:Ourcaseisa24-year-oldmanwhosufferedfromfatigue,malaiseandmicrocytic andhypochromicanemia,whoseupperdigestiveendoscopypresentedseveralhyperplastic polypsinthestomachandwhosecolonoscopyrevealedcolonicpolyposismainlyintheright colon;thehistopathologyshowedtubularadenomawithmoderateatypiaintheascending colon.Thus,avideolaparoscopicrightcolectomywasperformed;theanalysisofthe sur-gicalfragmentshowedmultiple(morethan30)polypsdistributedthroughthececumand ascendingcolon.
Conclusion: Thehistopathologicaldiagnosisofhyperplasticpolyposisisachallengingtask. Ingeneral,mostpolypsarehyperplastic,but serratedandclassicadenomasalsooccur. Theseassociatedadenomatousinjuriescanbethecauseofmalignanttransformation.So far,thereisnoconsensusabouttheappropriatetreatment;however,acolectomyprocedure maybebeneficialinascenarioofalargenumberofhyperplasticpolyps,concurrentserrated adenomas,ormultiplehigh-riskadenomatouslesions.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Polipose
hiperplásica:
relato
de
caso
Palavras-chave:
Síndromepoliposehiperplásica Colectomiavideolaparoscópica Polipose
r
e
s
u
m
o
ASíndromePoliposeHiperplásica(HPS),descritaem1980,éconsideradacomoapresenc¸a depóliposhiperplásicosmúltiplos,grandese/ouproximaise,ocasionalmente,umnúmero menordeadenomasserrados,adenomasclássicosepóliposmistos.Agrandemaioriados pacientessãoassintomáticos,sendoodiagnósticoumachadoincidentaldacolonoscopia. Notocanteaoprognóstico,amaioriadosautoresconsideraHPSumachadoincidentalsem
∗ Correspondingauthor.
E-mail:[email protected](T.A.Flauzino).
http://dx.doi.org/10.1016/j.jcol.2014.08.013
64
jcoloproctol(rioj).2015;35(1):63–66potencialdemalignizac¸ão,porém,estudosrecentestêmdescritolesõesgenéticas sincrôni-casàHPSeaocâncercolorretal.
Objetivo: OsautoresapresentamumrelatodecasodeSíndromePoliposeHiperplásicado servic¸odecoloproctologiadoVitóriaApartHospital,Vitória-ES.
CasoClínico: Trata-sedeumpacientede24anos,masculino,queapresentavafadiga, adi-namiaeanemiamicrociticaehipocrômicaqueapresentounaEndoscopiaDigestivaAlta: diversospóliposhiperplásicosnoestômagoenaColonoscopia:poliposecolônica princi-palmenteemcólondireitocujohistopatológicodemonstrouadenomatubularcomatipia moderadanoascendente.Paratalfoirealizadocolectomiadireitavideolaparoscópicaem queaanálisedapec¸amostroumúltiplospóliposhiperplásicosdistribuídospelocecoecólon ascendente,superiora30.
Conclusão:OdiagnósticohistopatológicodeHPSédesafiador.Emgeral,amaioriadospólipos sãohiperplásicos,mastambémocorremadenomasserradoseadenomasclássicos.Tais lesõesadenomatosasassociadaspodemseracausadetransformac¸õesmalignas.Ainda nãoháconsensodotratamentoadequado,porém,acolectomiapodeserbenéficaquando hágrandenúmerodepóliposhiperplásicos,adenomasserradosconcomitantesoumúltiplas lesõesadenomatosasdealtorisco.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Hyperplasicpolyposiswasdescribedin1980.Thisdiseaseis regardedasthe presenceofmultiplelargeand/or proximal hyperplastic polyps, and sometimes fewerserrated adeno-mas,classicalpolypsandmixedadenomas.Theydifferfrom isolatedhyperplasticpolyps,ascanreachupto3cm.1
Usu-allythesehyperplasticpolypsarefoundintheproximalcolon, occurequally amongmenand womenandexhibitfamilial character.Whileitisacceptedthatsmallhyperplasticpolyps havenomalignantpotential,therearecasesof adenocarcino-mataassociatedwithhyperplasticpolyposis(HPS).
Theguidelinesrecommendsomecriteriaforadefinitionof thediagnosisofHPS;thesecriteriaarealsousedbytheWorld HealthOrganization(WHO)andwereintroducedin2000.The criteriaare1:atleastfivehyperplasticpolyps
histopatholog-icallydiagnosedproximally tothe sigmoidcolon,with two ofthemmeasuringmorethan 10mmindiameter; or2 any
numberofhyperplasticpolypsoccurringproximallytothe sig-moidcoloninapatientwithafirst-degreerelativewithHPS; or3morethan30hyperplasticpolypsofanysize,butspread
throughoutthecolon.3
Althoughahyperplasticpolypisanon-neoplasticpolyp, it may present genetic changes, including chromosomal rearrangements, such as: Kras and BRAF proto-oncogenes’ mutation and low levels of DNA’s unstable microsatellites (MSI-H).TP53mutationsandincreasedp53 immunosuppres-sion are limited to areas of intraepithelial neoplasia and serratedadenomas.HighlevelsofMSI-Hareassociatedwith lossofDNAcapacityforerrorrepair,andthisisthelikelycause ofcolorectalinjuriesinHPSpatients.TheHPSalsoexhibits histopathologicfeaturesthatdifferfromnormalmucosa,for instance,anincreaseinthecryptproliferationzone(although confinedtothebaseofthecrypt),serratedarchitectural orga-nizationinbasilarareasofthecrypt,basilarexpansionofthe crypt,invertedcryptsandprevalenceofcryptswithreduced
maturation.Asmallportionofcasespresentssomedegreeof dysplasia,andevenanassociationwithtubular,tubulovillous, villousandserratedadenomata.4
Thevastmajorityofpatientsareasymptomatic,andthe diagnosisisanincidentalfindingfromcolonoscopy;aportion of patients may suffer rectal bleeding. Therefore, a high-definitioncolonoscopyandmultiplebiopsiesareessentialfor obtainingthisdiagnosis.
Withregardtoprognosis,mostauthorsconsiderHPSasan incidentalfinding,withnopotentialforcolorectal adenocarci-noma;however,recentstudieshavedescribedgeneticlesions occurringsynchronouslytoHPSandtocolorectalcancer, sup-porting the concept of the sequence:hyperplastic polyp – adenoma–colorectalcarcinoma.5-13
jcoloproctol(rioj).2015;35(1):63–66
65
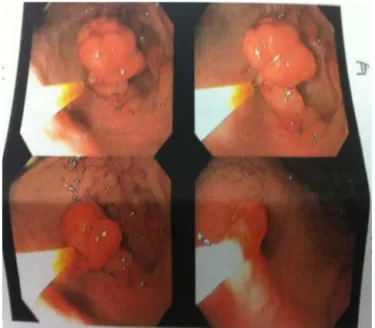
Fig.2–Colonoscopy:colonpolyposis.
Fig.3–Surgicalfragmentfromrightcolectomy,with intestinalpolyposis.
Objective
TheauthorspresentacasereportofHPSsyndromefrom Colo-proctologyService,VitóriaApartHospital,Vitória-ES.
Case
report
Our case is a 24-year-old man who suffered from fatigue, malaiseand microcytic and hypochromicanemia. No fam-ily historyofcolorectal canceror familialpolyposis.In the diagnosis,UpperDigestiveEndoscopy(UDE)revealedseveral polypsinthestomach,thelargestofthemmeasuring3cm, with a histopathologic study compatible withhyperplastic polyps;colonoscopy:colonicpolyposis(cecumandascending andtransversecolon),measuring1–5cm,witha1.5-cmpolyp inthesigmoidcolonandtwo1-cmsessilepolypsinthe rec-tum.Inthefaceofsuchfindings,polypectomywasperformed inthedistalcolonicsegmentsand,bysampling,intheright colon.Histopathologicalstudy(HPTL):retentionpolyp asso-ciatedwithlymphoidhyperplasiaintherectumandsigmoid colon;tubularadenomawithmoderateatypiainthe ascend-ingcolon(Figs.1–5).
Results
The patient underwent a partial right colectomy by videolaparoscopy; the surgical fragment measured
66
jcoloproctol(rioj).2015;35(1):63–66Fig.5–Colonoscopyfromnormalcontrol.
162mm, containing 50 sessile and pedunculated polypoid lesions.
The histopathological study of the surgical specimen revealed multiple (more than 30) hyperplastic polyps dis-tributed throughout the cecum and ascending colon; this findingfulfillsthecriteriaforHPSsyndrome.Theresearchfor BRAFgenemutationwasinconclusive.
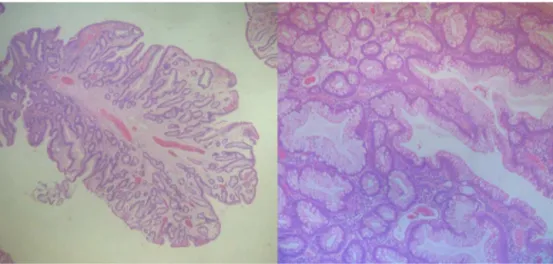
Apolypoidlesionwithacentralfibrovascularbundleand disorganization of crypt architecture was also noted; the cryptsshowed attheirbaseaproliferativezone, withhigh numberofcells,butwithoutdysplasia,characterizinga hyper-plasticpolyp.
Thepatient’s recovery wasuneventful, and he was dis-chargedonthe4thpostoperativeday.Currentlythepatient isunderrigorousclinicalandendoscopicfollow-up.
Conclusion
ThehistopathologicaldiagnosisofHPSisachallengingtask. Ingeneral,mostofthepolypsarehyperplastic,butserrated andclassicadenomascanalsooccur.Theseassociated adeno-matouslesionscanbethecauseofmalignanttransformation. There is no consensus about the appropriate treatment;
however,colectomymaybebeneficialincasesofalarge num-berofhyperplasticpolyps,concurrentserratedadenomas,or multiplehigh-riskadenomatouslesions.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.PoswarFO,CarneiroJA,MonteiroVA,FreitasMOS. Hyperplasticpolyposis:casereport.RevBrasColoproctol. 2010,July/September;30[RiodeJaneiro].
2.RashidA,HoulihanPS,BookerS,PetersenGM,GiardielloFM, HamiltonSR.Phenotypicandmolecularcharacteristicsof hyperplasticpolyposis.Gastroenterology.2000;119:323–32.
3.SurgicalPathologyoftheGITRACTLiver,BiliaryTractand Pancreas.
4.HamiltonSR,AaltonenLA(eds.).Pathologyandgeneticsof tumoursofthedigestivesystem.
5.HyungSuAhn,SuJinHong,HeeKyungKim,HeeYongYoo, HwaJongKim,BongMinKo.HyperplasticPoliposisSyndrome IdentifiedwithaRAFMutation.GutandLiver.2012:280–3.
6.WilliamsGT,ArthurJF,BusseyHJR,MorsonBC.Metaplastic polypsandpolyposisofthecolorectum.Histopathology. 1980;4:155–70.
7.LageP,SousaR,AlbuquerqueC,ChavesP,SalazarM,CravoM, etal.PoliposeHiperplásica:Caracterizac¸ãoFenotípicae Moleculardeumaentidaderaracomriscoaumentadode cancrodocólonerecto.JPortGastro.2004;11:76–83.
8.GoldsteinNS,BhanotP,OdishE,HunterS.Hyperplastic-like ColonPolypsThatPrecededMicrosatellite-Unstable Adenocarcinomas.AmJClinPathol.2003;119:778–96.
9.BurtRW,JassJR.Hyperplasticpolyposis.In:HamiltonSR, AaltonenLAeditor.WorldHealthOrganizationclassification oftumours.Pathology&genetics.Tumoursofthedigestive system.Lyon:IARCPress;2000.
10.HawkinsNJ,GormanP,TomlinsonIP,BullpittP,WardRL. Colorectalcarcinomasarisinginthehyperplasticpolyposis syndromeprogressthroughthechromosomalinstability pathway.AmJPathol.2000;157:385–92.
11.PlaceRJ,SimmangCL.Hyperplastic-adenomatouspolyposis syndrome.JAmCollSurg.1999;188:503–7.
12.RiccioAAL,GodwinAK,LoukolaA,PercesepeA,SalovaaraR, MasciulloV,etal.TheDNArepairgeneMBD4(MED1)is mutatedinhumancarcinomaswithmicrosatelliteinstability. NatGenet.1999;23:266–8.