jcoloproctol(rioj).2015;35(1):42–45
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Anal
fistula
surgery
in
an
outpatient
setting:
the
Dubai
experience
Wessam
Hazim,
Labib
Al-Ozaibi
∗,
Hadiel
Azam,
Alya
Al-Mazrouei,
Faisal
Al-Badri
SurgicalDepartment,RashidHospital,DubaiHealthAuthority,Dubai,UnitedArabEmirates
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8October2014
Accepted27November2014
Availableonline28January2015
Keywords:
Analfistula
Proctology
Ambulatorysurgery
Daycasesurgery
a
b
s
t
r
a
c
t
Aim:Todeterminewhethersurgeryfortranssphinctericandcomplexfistula-in-anocanbe
performedsafelyasadaycase.
Method:Thisisaretrospectivestudyof66patientswithtranssphinctericandcomplexanal
fistulas,initiallymanagedwithpreliminarylooseSetonfollowedbyfistulectomyand
sphinc-terrepair2–4monthslaterbetweenMarch2011andMarch2014.Patientswereseenatthe
clinic1week,3monthsand1yearpost-operativelyandwereobservedforcomplications
andrecurrences;incontinencewasnoteddownandwasgradedaccordingtotheCleveland
Clinicscore.
Result:Twenty-fivepatients(38%)hadhighorcomplexfistulasand32(48.5%)hadahistory
ofprevioussurgery.Allcasesweredoneinanoutpatientsetting.TheSetonwaskeptinsitu
for2–5months(2.6months)followedbyfistulectomyandsphincterrepair.Completehealing
wasachievedwithinapproximately3.6weeks(2–8weeks).Fifty-onepatientswerefollowed
upsuccessfullyforoneyear.Twopatientshadtemporaryflatusincontinencewhichhad
resolvedover2–3months.Recurrencehadoccurredin2(3.9%)patients.
Conclusion:Transsphinctericandcomplexfistulascansafelybeoperatedonasdaycase
surgerieswithhighpatientsatisfactionandlesscomplicationinthepopulationwestudied.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All
rightsreserved.
Cirurgia
de
fístula
anal
em
regime
ambulatorial:
a
experiência
Dubai
Palavras-chave:
Fístulaanal
Proctologia
Cirurgiaambulatorial
Cirurgiasempernoitehospitalar
r
e
s
u
m
o
Objetivo:Determinarsecirurgiasparafístulastransesfincterianaseparafistulaeinano
com-plexaspodemserrealizadascomseguranc¸aemambienteambulatorial,sempernoitedo
pacientenohospital.
Método:Trata-sedeumestudoretrospectivode66pacientescomfístulastransesfincterianas
efístulasanaiscomplexas,inicialmentetratadospreliminarmentecomsetondedrenagem,
seguidoporfistulectomiaereparodoesfíncter2–4mesesmaistarde,entremarc¸ode2011e
marc¸ode2014.Ospacientesforamreexaminadosnoambulatórioumasemana,trêsmeses
∗ Correspondingauthor.
E-mail:[email protected](L.Al-Ozaibi).
http://dx.doi.org/10.1016/j.jcol.2015.01.005
jcoloproctol(rioj).2015;35(1):42–45
43
eanoapósacirurgia,tendosidoobservadosparacomplicac¸õeserecorrências;casosde
incontinênciaforamanotadoseclassificadosdeacordocomoescoredaClevelandClinic.
Resultado: Vinteecincopacientes(38%)apresentaramfístulasaltas oucomplexase32
(48,5%)tinham históriadecirurgia prévia.Todosos casosforamtratadosem ambiente
ambulatorial.Osetonfoimantidoinsitudurante2–5meses(2,6meses),seguidopor
fis-tulectomiaereparodoesfíncter.Acuracompletaseconcretizouemcercade3,6semanas
(2–8semanas).Cinquentaeumpacientesforamacompanhadoscomsucessoaolongode
umano.Doispacientestiveramincontinênciatemporáriaparagases,resolvidaaolongode
2–3meses.Recorrênciaocorreuem2(3,9%)pacientes.
Conclusão: Fístulas transesfincterianas e fístulas complexas podem ser operadas com
seguranc¸acomocasosambulatoriais,sempermanênciahospitalarnoturna,comgrande
satisfac¸ãodopacienteemenoscomplicac¸õesnapopulac¸ãoestudada.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.
Todososdireitosreservados.
Introduction
Most of the proctology cases nowadays are done as
day case surgeries without any significant complications.
Normally, ‘lay-open’ fistulotomies and fistulectomies for
inter-sphinctericfistulasaredoneasdaycases.High
trans-sphinctericandcomplicatedfistulas,whichrequireddivision
ofa large portion of the externalsphincter, were done as
inpatientsurgeries mainly due tothe fear of incontinence
andpostoperativepain.Theaimofsurgicaltreatmentofanal
fistulaistocurethediseasebypreventingrecurrencewhile
simultaneouslyensuringthatfecalcontinenceismaintained.
Theincidenceofpost-operativefecalincontinencefollowing
fistulectomyhas been reported to be 20.3%.1 Itis still not
clearwhichapproachissafesttobeperformedasadaycase
surgeryintermsofriskofimmediateorearlypost-operative
complications,asthosecomplicationscouldaffect the
out-comeofthesurgery.Theoptimaltreatmentofanalfistulas
shouldincludeminimalcomplications,lowrecurrencerates,
nohospitaladmissionsandnegligiblepatientinconveniences.
Theaimofthisstudyistopresentanexperienceoftreating
fistula-in-anoinanoutpatientsetting.
Method
Datawerecollectedfromrecordsof66patientswho
under-wentpreliminarySeton placementfollowedbyfistulectomy
andsphincterrepair2–4monthslaterbetweenMarch2011and
March2014.FistulaswerecharacterizedusingParks’
Classifi-cation.Perianalfistulasweredefinedascomplexiftheyhad
multipleexternalopenings,highfistulasiftheyhadan
inter-nalopeningatthelevelofthedentatelineandlowfistulasif
theyhadaninternalopeningbelowthedentateline.Patients
withconcomitantanalpathologyorinflammatorybowel
dis-easewereexcludedfromthestudy.Lowfistulas,whichwere
treatedbythe lay open technique, were alsoexcluded. All
patientshadanASAphysicalstatusclassificationoflessthan
3.
Theprocedurewas performedundergeneralanesthesia
withthepatientinlithotomyposition.Afterinitialevaluation,
theexternalandinternalopeningswerelocatedusingaprobe
andairinjectionalongthetract.AlooseSetonwasinserted
under general anesthesia using 2 braided, non-absorbable
sutures(4/0prolene),whichwereloopedaroundthefistula
tract.Itwasnottightenedatanytimeduringthefollow-up
norwasitremoveduntilthetimeoffistulectomy.Twotofour
monthslaterthecompletefistulawasexcisedwith
immedi-aterepairofthesphinctersandthewoundwaskeptopen.
Setoninsertionandfistulectomyweredoneasdaycases.The
patientswereobservedfor4–6handwerethendischarged.
Patientswerereviewedattheclinic1week,3monthsand
1yearpostoperatively.Duringthefollow-upperiod,details
ofhealing(i.e.absenceofdischarge),recurrence,and
compli-cationswere gathered.Continencewasevaluatedaccording
totheClevelandClinicscore.2Theexcisedfistulasweresent
forhistopathologytoruleoutinflammatoryboweldiseaseand
cancer.
Finally,thedatawereanalyzedusingIBMSPSSSTATISTICS
BASE21.
Results
Afterobtainingtheethicalcommitteeapproval, 66patients
with transsphincteric and complex anal fistulaswho were
managed withpreliminarylooseSetonfollowedby
fistulec-tomyandsphincterrepair,werereviewed.Fifty-nine(89.4%)of
thepatientsweremaleand7(10.6%)werefemale.Theoverall
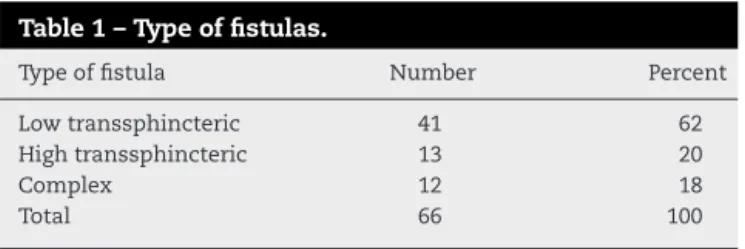
meanagewas38.5(range25–61)years.Thetypesoffistulas
aredepictedinTable1.
Thirty-two (48.5%) patients gave a history of previous
surgery, 27 ofwhichhad incision and drainageofperianal
abscessesand5ofwhichhadpreviousfistulasurgeries.The
Table1–Typeoffistulas.
Typeoffistula Number Percent
Lowtranssphincteric 41 62
Hightranssphincteric 13 20
Complex 12 18
44
jcoloproctol(rioj).2015;35(1):42–45Setonwasinsertedandkeptinsitufor2–5months(average2.6
months).Thesecondprocedureconsistedoffistulectomyand
sphincterrepair;allcasesweredoneasdaycasesandwere
performedundergeneralanesthesia.
During the follow-up period there were no
signifi-cant complications. Four (6%) patients experienced
signifi-cant post-operativepain, which required oralnonsteroidal
anti-inflammatorymedications andacetaminophens.Three
patients(4.5%)hadminimal bleedingwhich wascontrolled
bypressuredressingalone.Thecompletehealingtimeofthe
woundwas between2and 8weeks(average 3.5weeks) in
whichnomoredressingwasrequired.
Fifty-one(77.3%)patientscompletedafollowupof12–24
months (mean 16 months); they were assessed for
recur-renceandpresenceofincontinence.Whiletwopatients(3.9%)
reported atransient incontinence ofgasin the immediate
postoperativeperiod(scores3and 4,respectivelyaccording
tothe Cleveland Incontinence Score), theyhad completely
recoveredby3monthspostoperative.Thefistulaswere
com-pletelycuredin49(96.1%)ofthepatients.Recurrenceoccurred
in only two patients (3.9%); one of them was re-operated
usingthesameprocedure–looseSetonfor4monthsfollowed
byfistulectomyandsphincterrepair–forwhichduringthe
follow-uphedidnothaveanyremainingsignsofrecurrence,
whiletheother patient wentthrough another fistulectomy
withoutpreliminarySetoninanotherhospitalandcontinued
tohaverecurrence.
Patientswereinterviewedfortheirsatisfactionofthe
pro-cedurebeingdone asadaycaseand 64outofthe66were
satisfied.Twopatientspreferredthesurgerytobedoneinan
inpatientsettinginordertoreceivepostoperativeanalgesia
andrest.
Discussion
Inabusy hospitalwheretheshortage ofbeds isthe main
issue,the admissionofsuchcaseswasincreasingtheload
andthecostonhospitalresources.Inaddition,thenumberof
casesthatwouldhavebeenoperatedonwouldhavebeenfar
lessduetothelongwaitinglistforadmission.Before2011,all
casesoffistulasweredoneasinpatientandbetweenJanuary
2010andFebruary2011;only8fistulacaseswereadmittedand
operatedon.Thenumberofadmissiondaysvariesbetween2
and5days(ameanof3days).
Thestrategytooperatetranssphinctericandcomplexanal
fistulasasdaycasesstartedinMarch2011,andupuntilMarch
2014the numberofcasesdone onanoutpatientbasishad
increasedto66cases. Thisstrategyhad aidedthe hospital
managementtoimprovethebedoccupancyrateandinturn,
thecosteffectiveness.
A day care clinic is defined as an institution in which
patientsundergoelectiveoperationsonthedayoftheir
admis-sionandaredischargedwithin24hofthesurgery.3
Nowadays,proctologic conditions are increasingly
man-agedonanoutpatientbasis.Thishasbeenassociatedwitha
successfulpostoperativeoutcome.Severalfactorsplayarole
inthisrecentincrease,suchasmodernanestheticprocedures,
shortoperationtimeand alowcomplicationrates. Careful
patientselectionremainsthekeytoasuccessfuloutcome.
InColoproctology, thehigh incidenceofanorectal
disor-ders and the economicimpact ofvarious typesofsurgical
treatmenthavemotivatedattemptstodiscoverpossibilities
ofoutpatientmanagement.While30–50%ofallsurgeriescan
besafelydoneinoutpatientsectors,thisratereaches90%in
thecaseofanorectaloperations.4Amongallthesurgical
spe-cialties, anorectalsurgeryhasbenefitedthe mostfrom the
useoflocalanesthesiaandambulatorysurgery.Many
stud-iesagreethattheoutpatientenvironmentissafeforanorectal
surgery.5
Despite thesocial,economicand medicaladvantagesof
ambulatory proctologic surgery, the majority of surgeons
are reluctant to put this into practice for several reasons
suchasdifficultyinassuringadequate paincontrol,fearof
postoperativecomplications,andthelackofpatient’s
dissem-ination knowledge about safety and feasibilityof daycare
surgeries.6
Several studies have been conducted to analyze the
feasibility of day case surgeries in proctology. Different
procedures have been tested such as haemorrhoidectomy,
sphincterotomy,anorectalpolypexcisionandpilonidalsinus
surgery.
In regards to fistula-in-ano surgeries, its feasibility has
beenproveninseveralstudies.InthestudybyCarditelloetal.7
172 fistulas-in-anohavebeenoperatedoninanoutpatient
setting.Thirty-fourpercentofpatientswerehospitalizedfor
24h,whiletheremainingwashospitalizedfor7–10h.No
con-siderable complicationshave beendocumented apart from
postoperativepain.
InapaperwrittenbyGuptaetal.,themeanhospitalstay
was7.3h(range4–21h)whiletheoverallcomplicationratewas
2.5%, whichincludedbleeding, urinaryretention,infection,
continenceproblemsandrecurrence.8
Conclusion
Transsphincteric and complex anal fistulas can be treated
safelyandeffectivelyinanoutpatientsettingwithless
com-plicationandwithhighpatientsatisfactioninthepopulation
westudied.Itwasproventobecosteffectiveandimproved
thehospitalcapacity.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ToyonagaT,MatsushimaM,KiriuT,SogawaN,KanyamaH, MatsumuraN,etal.Factorsaffectingcontinenceafter fistulotomyforintersphinctericfistulainano.IntJColorectal Dis.2007;22:1071–107.
2.JorgeJM,WexnerSD.Etiologyandmanagementoffecal incontinence.ColonRectum.1993;36:77–97.
3.MassonJL.OutpatienthemorrhoidectomyusingtheCO2laser.
JChir.1990;127:227–9.
jcoloproctol(rioj).2015;35(1):42–45
45
5.BergantinoA.Thesurgicaltherapyofhaemorrhoidal pathologyperformedinone-daysurgery.MinervaChir. 1999;54:485–90.
6.KolbertG,KirschJ.Outpatientsurgeryinproctology.WienMed Wochenschr.2004;154:73–5.
7.CarditelloA,MeduriF,CardilloP,MuleV,LaRoccaT,CaminitiF. Proctologicday-surgery:resultsof2000surgicalinterventions. ChirItal.2001;53:219–24.