w w w . r b o . o r g . b r
Original
Article
Epidemiology
of
fractures
of
the
proximal
third
of
the
femur
in
elderly
patients
夽
Daniel
Daniachi
∗,
Alfredo
dos
Santos
Netto,
Nelson
Keiske
Ono,
Rodrigo
Pereira
Guimarães,
Giancarlo
Cavalli
Polesello,
Emerson
Kiyoshi
Honda
DepartmentofOrthopedicsandTraumatology,IrmandadedaSantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11March2014 Accepted10July2014 Availableonline27June2015
Keywords:
Epidemiology Hipfractures Elderlypeople
a
b
s
t
r
a
c
t
Objective:Thiswasanepidemiologicalstudyonfracturesoftheproximalthirdofthefemur inelderlypatientswhoweretreatedatateachinghospitalinthecentralregionofSãoPaulo.
Methods:Thesubjectswerepatientsovertheageof60yearswhowereattendedovera 1-yearperiod.Aquestionnaireseekingbasicsociodemographicdataandinformationon comorbiditiespresentedandmedicationsusedwasdrawnup.Thecircumstancesofthe fracturesandtheircharacteristics,thetreatmentinstitutedandtheintra-hospitalmortality ratewereevaluated.
Results:The113patientsincludedinthestudypresentedameanageof79years.Theratio betweenthesexeswasthreewomentoeachman.Only30.4%ofthepatientsreportedhaving osteoporosisandonly0.9%hadhadtreatmentforthedisease.Low-energytraumawasthe causeof92.9%ofthefractures.Femoralneckfracturesaccountedfor42.5%ofthefractures andtrochantericfractures,57.5%.Fivepatientsdidnotundergooperations;39underwent jointreplacement;and69underwentosteosynthesis.Themeanlengthofhospitalstaywas 13.5daysandthemeanlengthofwaitingtimeuntilsurgerywas7days.Theintra-hospital mortalityratewas7.1%.
Conclusion: Thepatientsattendedatthisinstitutionpresentedanepidemiologicalprofile similartowhatisfoundintheBrazilianliterature.Chronickidneyfailureisasignificant factorwithregardtointra-hospitalmortality.Preventivemeasuressuchasearlydiagnosis andtreatmentofosteoporosisandregularphysicalactivitypracticeswerenotimplemented. ©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedwithintheHipGroup,DepartmentofOrthopedicsandTraumatology,IrmandadedaSantaCasadeMisericórdiade SãoPaulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.Daniachi).
http://dx.doi.org/10.1016/j.rboe.2015.06.007
Epidemiologia
das
fraturas
do
terc¸o
proximal
do
fêmur
em
pacientes
idosos
Palavras-chave:
Epidemiologia Fraturasdoquadril Idoso
r
e
s
u
m
o
Objetivo: Estudoepidemiológicodasfraturas doterc¸oproximaldofêmur empacientes idosos,tratadosemhospital-escolanaregiãocentraldeSãoPaulo.
Métodos: Pacientes a partir 60 anos atendidos no período de um ano. Questionário foielaboradocominformac¸õessociodemográficasbásicas,comorbidadesapresentadase medicac¸õesemuso.Foramavaliadascircunstânciasdafraturaesuascaracterísticas, trata-mentoinstituídoetaxademortalidadeintra-hospitalar.
Resultados: Os113 pacientesincluídos no estudoapresentavam 79 anos em média.A proporc¸ão entreos sexosfoi de três mulherespara cadahomem.Somente 30.4% dos pacientesrelataramosteoporoseesomente0.9%tratavamadoenc¸a.Traumadebaixa ener-giafoiacausade92,9%dasfraturas.Fraturasdocolodofêmurrepresentaram42,5%das fraturasetrocantéricas57,5%.Cincopacientesnãoforamoperados,39foramsubmetidosa substituic¸ãoarticulare69foramsubmetidosaosteossíntese.Otempomédiodeinternac¸ão foide13,5diasedeesperaatéacirurgiasetedias.Ataxademortalidadeintra-hospitalar foide7,1%.
Conclusão:Pacientesatendidosnainstituic¸ãoapresentamperfilepidemiológicosemelhante àquelesencontradosemliteraturanacional.Insuficiênciarenalcrônicaéumfator signi-ficativoparamortalidadeintra-hospitalar.Medidaspreventivascomodiagnósticoprecoce etratamentodaosteoporoseepráticaregulardeatividadesfísicasnãosãoadotadas.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
AgingofthepopulationisaBrazilianreality.In1991,thetotal numberofelderlypeople,i.e.individualsaged60yearsand over,was10.7millionor7.2%ofthepopulation.In2011,this groupamountedto23.5millionor12.1%ofthepopulation.
Thistrendhasledtogreaterconcernregardingproblems ofdiseasesrelatingtothisagegroup,whichincludefractures oftheproximalthirdofthefemur.Thesecauseahighrateof morbidityandmortality.1–3Alargenumberofthesepatients
diewithintwoyearsandmanyneverrecovertheirqualityof lifeorfunctionalindependence.4–6
Amongelderlypeople,thesefracturesoccurinrelationto low-energytrauma.Themaincauseisfallsfromastanding position.3,5,7,8 Severalriskfactorshavebeencorrelatedwith
fracturesoftheproximalthirdofthefemurand,amongthese, advancedageandosteoporosisstandout.2,9,10
These fractures can be divided into femoral neck, transtrochantericandsubtrochantericfractures.5,6Allofthem
should be treated surgically,1,5 but there is no consensus
regarding the best surgical technique for each of them. Nonetheless,therearefactorsrelatingtothetreatmentthat maymodifythemortalityrateamongthesepatients.These includethelengthoftimebetweenhospitaladmissionand surgery,useofprophylacticantibiotictherapy,anduseof post-operativephysiotherapy.3,4,11–13
Theobjectiveofthisstudywastodeterminethe epidemi-ologicalprofileoffracturesoftheproximalthirdofthefemur amongelderlypeople whowere treatedinthe orthopedics departmentofahospital.Thus,thestudyaimedtoanalyzethe causesofthefractures,theircharacteristicsandthetreatment
instituted.Inadditionitaimedtoobservewhethermeasures werebeingtakentoavoidsimilarnewoccurrences.
Sample
and
method
Thiswasaprospectiveobservationalstudyconductedina sin-gleteachinghospitalinthecentralregionofthecityofSão Paulo.Thestudyincludedelderlypatientswithfracturesof theproximalthirdofthefemurwhowereattended consecu-tivelybetweenAugust1,2009,andJuly31,2010.Patientswere excludediftheyrefusedtoparticipateorwerenotina condi-tiontoanswerquestions.Patientswerealsoexcludedifthey hadadiagnosisofmetastaticfractureorafracturerelatedto neoplasticprocessesinthefemur.
Aquestionnairewasdrawnupbythepresentauthors,to beanswered bythepatientsthemselves orbyarelativeor caregiverwhomightbelivingwiththepatient.Inthis ques-tionnaire,inadditiontobasicsociodemographicinformation suchassex,age,nationality,ethnicityandworkactivity,the traumamechanism,theplacewheretheeventoccurredand timewhenitoccurredwereevaluated.Thepatientswerealso askedabout anycomorbidities,includingosteoporosis,that theywereawareofhaving,alongwiththemedicationsthat theywereusing.
Theotherdatagatheredinthe presentstudycomprised thetypeoffracture,totaldurationofhospitalstay,presence ofosteoporosisseenonradiography,lengthofwaitingtime untilsurgeryandtreatmentinstituted.
neckfractures,weusedGarden’sclassificationandgenerically definedtypesIandIIasstablefractures,whiletypesIIIandIV correspondedtounstablefractures.
Todefinethepresenceorabsenceofosteoporosisasseen onradiography,Singh’smethodwasapplied.14
Thisstudy was previously approvedbyour institution’s researchethicscommittee.
Results
Thequestionnairewasansweredby113patients(28malesand 85females)andthesewereincludedinthestudy.Theirages werebetween60and99years(meanof79).Regarding occu-pation,109wereonlydoinghousework.Fourpatientswere economicallyactive.Noneofthemwereinstitutionalizedand only18werelivingalone.
Fallswere reportedby115patients. Theothers had suf-feredhigh-energytrauma.Amongthefalls,81hadoccurred inthepatient’sownhome,while24wereinthestreets.Most oftheseeventsoccurredinthepatient’s bedroom,followed bythebathroom.Approximatelytwo-thirdsofthefractures occurredduringtheday.Sixty-fivepatientshadahipfracture duringthecolderseasons,while48were duringthehotter seasons.
Only16patientssaidthattheydidnothaveanytypeof disease.Thedisease mostfrequentlyfoundonitsownwas systemicarterialhypertension,in23patients.Fifteenpatients werediabetic,sevenwerediagnosedwithAlzheimerandsix hadhypothyroidism.Twenty-twopatientshadthreeormore comorbidities.
Twopatientsweredoingregularphysicalactivities(walking inbothcases).
Whenaskedaboutpreexistingdiseases,onlytwopatients reportedthattheyhadosteoporosis.Weincludedaspecific questionaboutthisdiseaseinthequestionnaire.Whenasked whethertheyhadosteoporosis,34patients(30.1%)saidthat theydid.Weanalyzedtheradiographs ofthesepatients in accordancewiththecriteriadescribedbySingh14andfound
that107patients(94.7%)hadosteoporosis.
Twenty-twopatients were notmakinguse ofany medi-cation.Captopril was the medication most used.Only one patientreportedusingspecificmedicationfortreating osteo-porosis(alendronate).Noneofthepatientswereusingvitamin D.
The type of fracture most commonly encountered was transtrochanteric, in 57 cases. There were 48 cases of femoral neck fractures and eight cases of subtrochanteric fractures.
Five patients had not undergone any operation, while 108 had undergone some type of surgical intervention. Osteosynthesis was the treatment instituted in all the casesofsubtrochanteric fractures and in56 (98.2%) ofthe transtrochanteric fractures. One case of transtrochanteric fracturewastreatedwithjointreplacementbecauseadvanced arthrosiswaspresentedinthis joint.Inrelationtofemoral neckfractures,39wereconsideredtobeunstableandwere treatedwithjointreplacement,whileeightstablecases under-wentfixation.
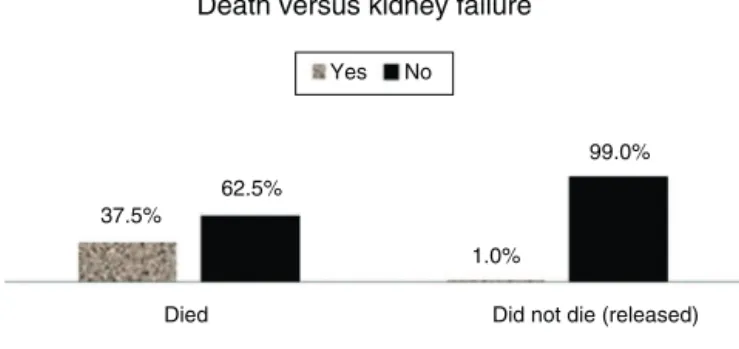
Died Did not die (released)
Death versus kidney failure
1.0% 62.5%
99.0% Yes No
37.5%
Fig.1–Theonlyriskfactorthatwasfoundtoseparately
increasemortalityinthehospitalwaschronickidney
failure.Thepercentageofpatientswithkidneyfailurewas
significantlygreateramongthepatientswhodiedthan
amongthosewhodidnotdie.
Themeandurationofthepatients’hospitalstaywas13.5 daysandthe meanlengthoftimethatthepatientswaited betweenhospitaladmissionandthesurgerywas7days.
Thenumberofpatientsreleasedfrom hospitalwas 115. Eight patients (7.1%) died whilein hospital, amongwhom sixwereover80yearsofageandthreehadbeendiagnosed withchronickidneyfailure.Fiveofthesepatientshadfemoral neck fractures(four ofthem underwent jointreplacement) andthreehadtranstrochantericfractures(whichunderwent fixation).
Weanalyzedthecasesofdeathinthehospitalinrelation toseveralvariables,especiallythefollowing:typeoffracture, typeofsurgery,numberofassociateddiseases,seasonofthe year,radiographicosteoporosisandage.Atthe5%significance level,therewasnorelationshipbetweendeathandthe vari-ables,ascanbeseeninTable1.
Theonlyriskfactorforhighermortalityinthehospitalthat wasfoundseparatelywaschronickidneyfailure.The percent-ageofthepatientswithkidneyfailurewassignificantlygreater amongthepatientswhodied,incomparisonwiththepatients whodidnotdie(Fig.1).
Thesamevariableswerealsoevaluatedinrelationtothe totaldurationofthehospitalstayandthetimethatelapsed betweenhospitaladmissionandthesurgicaltreatment.None ofthesewereshowntobestatisticallysignificantinrelation tothelengthoftimespentwaitingfortheoperation.Thetype ofsurgerywasstatisticallysignificantinrelationtothetotal duration ofthe hospitalstay.Thepatients whounderwent osteosynthesisstayedinhospitalforlesstimethandidthose whounderwentjointreplacement(Tables2and3).
Therewasadifferencebetweenthepercentagesofpatients whoreportedhavingosteoporosisandwhopresented osteo-porosisseenonradiography,suchthatthepercentageofthe patients withosteoporosisseenonradiography was signif-icantly greater than the percentage reporting osteoporosis (Fig.2).
Discussion
Table1–Deathinthehospitalcomparedinrelationtothefollowingvariables:typeoffracture,typeofsurgery,number ofassociateddiseases,seasonoftheyear,radiographicosteoporosisandage.
Death(yesorno)comparedwiththevariables Died(%) Didnotdie(%) Total(%) pvalue
Typeoffracture
Stablefemoralneck 0(0) 9(8.6) 9(8) 0.387b
Unstablefemoralneck 4(50) 35(33.3) 39(34.5)
Unstablesubtrochanteric 0(0) 8(7.6) 8(7.1)
Transtrochanteric 4(50) 53(50.5) 57(50.4)
Total 8(100) 105(100) 113(100)
Typeofsurgery
Fixation 3(42.9) 65(64.4) 68(63) 0.420a
Replacement 4(57.1) 36(35.6) 40(37)
Total 7(100) 101(100) 108(100)
Numberofassociateddiseases
0 0(0) 16(15.2) 16(14.2) 0.273b
1or2 6(75) 70(66.7) 76(67.3)
3or4 2(25) 19(18.1) 21(18.6)
Total 8(100) 105(100) 113(100)
Seasonoftheyear
Winter 3(37.5) 33(31.4) 36(31.9) 0.150b
Autumn 4(50) 25(23.8) 29(25.7)
Spring 1(12.5) 26(24.8) 27(23.9)
Summer 0(0) 21(20) 21(18.6)
Total 8(100) 105(100) 113(100)
Osteoporosisseenonradiography
Yes 8(100) 99(94.3) 107(94.7) 1.000a
No 0(0) 6(5.7) 6(5.3)
Total 8(100) 105(100) 113(100)
Agegroup
60–70years 0(0) 22(21) 22(19.5) 0.115b
71–80years 2(25) 33(31.4) 35(31)
>80years 6(75) 50(47.6) 56(49.6)
Total 8(100) 105(100) 113(100)
Source:Filesofthehospitalservice. a Fisher’sexacttest.
b Likelihoodratiotest.
theproportionsof3:1.Thepatients’meanagewas79years. Inaprevioussampleinthesamehospital(2004–2005), Hun-griaetal.8foundpredominanceofwomenintheproportions
of2:1andamean ageof78.2 years.Ramalho etal.9 found
proportionsof3.3:1andameanageof78.5years.
Inourstudy,wefoundthat92.9%ofthefractureswere asso-ciatedwithlow-energytrauma.Thiswasalowerproportion thanintheUnitedStates,whereStevensandSogolow7
cor-relatedmorethan95%ofthefractureswithfalls.Previously publishedBrazilianstudieshavereportedslightlylower per-centages:Hungriaetal.,887.3%;Asturetal.,391.4%;andRocha
etal.,573.5%.Thegreatmajorityofthesefallsoccurredinside
thepatients’homes:inourseries,76.9%;Hungriaetal.,873.4%;
andPereiraetal.,1362.6%.Themajorityofthefallsoccurred
duringtheday,predominantlyinthebedroom,followedby thebathroom,i.e.inplaceswheretheseelderlyindividuals werealone.Thesefindingscorroboratedthetheorydefended byHungriaetal.,8Siqueiraetal.10andPinheiroetal.,15among
others,thatimprovementstoelderlypeople’shousing,suchas removalofunnecessaryfurniture,avoidanceofslipperyfloors, supportbarsnexttothetoiletbowlandshower,andavoidance ofrugsandmats,couldavoidmanyfractures.
Alsoinrelationtofalls,otherknownriskfactorswere iden-tifiedinoursample.Patientswhousedmorethanonetypeof medicationreportedthatthesewereoftenprescribedby dif-ferentphysiciansandthattheywerealmostneverreviewed withtheaimofpreventingoccurrencesoffalls.Thelatter mea-surewasadvocatedbySiqueiraetal.10Onlytwopatients(1.8%)
weredoingphysicalactivity.Siqueiraetal.10showedthatthere
wasgreaterprevalenceoffallsamongsedentaryelderly peo-ple.BandeiraandCarvalho16concludedthatphysicalactivity
wasapreventivemeasureagainstfracturesoftheproximal femuranddiminishedtheosteoporosisrate.
Only16patientsdidnotreportanypresenceofdiseasesand only22werenotmakinguseofanymedications;76reported havingoneortwocomorbiditiesand21,threeormore.None ofthesedatawerefoundtobestatisticallysignificantwith regardtodeathinthehospitalorgreaterlengthsoftime wait-ingfortheoperation,butwereimportantfactorswithregard tomortalitywithin1yearaftertheoperation.1,2,11
Table2–Waitingtimeuntilsurgerycomparedwiththefollowingvariables:typeoffracture,typeofsurgery,numberof associateddiseases,seasonoftheyear,radiographicosteoporosisandage.
Timeelapsedbetweenhospitaladmissionandsurgeryinrelationtothevariables pvalue
Typeoffracture Stablefemoralneck Unstablefemoralneck Unstablesubtrochanteric Transtrochanteric
Mean±standarddeviation 4.5±2.4 8.6±9.3 8.9±7 5.9±3.6 0.364a
Median(minimum–maximum) 6(1–7) 6(1–50) 8(0–22) 5(0–14)
Typeofsurgery Fixation Replacement
Mean±standarddeviation 6.1±4.1 8.6±9.2 0.279b
Median(minimum–maximum) 6(0–22) 6(1–50)
Numberofassociateddiseases 0 1or2 3or4
Mean±standarddeviation 5.7±4.6 6.7±5.5 9.2±10.1 0.215c
Median(minimum–maximum) 4.5(1–17) 6(0–36) 6.5(2–50)
Seasonoftheyear Winter Autumn Spring Summer
Mean±standarddeviation 7.3±4.8 4.9±3.4 8.2±10.9 7.9±4.3 0.238c
Median(minimum–maximum) 6(0–22) 4(1–12) 6(0–50) 7(1–17)
Radiographicosteoporosis Yes No
Mean±standarddeviation 6.9±6.6 8.8±4.4 0.482d
Median(minimum–maximum) 6(0–50) 9(3–13)
Agegroup 60–70years 71–80years >80years
Mean±standarddeviation 7.8±5.3 8.5±9.5 5.7±3.7 0.221a
Median(minimum–maximum) 6(0–22) 6(2–50) 5(0–17)
a Kruskal–Wallisnonparametrictest.
b Mann–Whitneynonparametrictest.
c Analysisofvariance(ANOVA)model.
d Student’sttest.
proximalfemur.10,16,17Fromanalyzingradiographsofthehip
inanteroposteriorview,wefoundthat94.7%ofthepatients wereosteoporoticinaccordancewiththemethoddescribed bySingh.Specificstudiesontheprevalenceofosteoporosis
showedthatit was33.4%amongpatientsaged60–69years and 72.7% amongpatientsover theage of80 years,inthe seriesreportedbyBandeiraandCarvalho.16Thisdiscrepancy
wasexpected,giventhatoursampleonlydealtwithpatients
Table3–Lengthofhospitalstaycomparedinrelationtothefollowingvariables:typeoffracture,typeofsurgery,number ofassociateddiseases,seasonoftheyear,radiographicosteoporosisandage.
Lengthofhospitalstayinrelationtothevariables pvalue
Typeoffracture Stablefemoralneck Unstablefemoralneck Unstablesubtrochanteric Transtrochanteric
Mean±standarddeviation 8.8±3.9 16.3±12.6 14.9±12.9 12.1±8.3 0.202a
Median(minimum–maximum) 9(3–14) 13(1–56) 13(2–43) 10(3–54)
Typeofsurgery Fixation Replacement
Mean±standarddeviation 11±6.9 16.1±12.4 0.027b
Median(minimum–maximum) 9(2–43) 13(1–56)
Numberofassociateddiseases 0 1or2 3or4
Mean±standarddeviation 10.1±6.9 13.3±10.2 16.6±11.7 0.156c
Median(minimum–maximum) 7.5(1–23) 11(2–54) 13(6–56)
Seasonoftheyear Winter Autumn Spring Summer
Mean±standarddeviation 13.1±7.9 12.4±12.3 15.3±12.7 13±6.9 0.738c
Median(minimum–maximum) 12(3–43) 8(5–54) 12(2–56) 11(1–29)
Radiographicosteoporosis Yes No
Mean±standarddeviation 13.4±10.4 13.7±7 0.958d
Median(minimum–maximum) 11(1–56) 12(6–22)
Agegroup 60–70years 71–80years >80years
Mean±standarddeviation 13.8±9.5 14.3±12.4 12.8±9.1 0.779c
Median(minimum–maximum) 11.5(2–43) 11(4–56) 10.5(1–54)
Boldindicatesignificanceis5%. a Kruskal–Wallisnonparametrictest.
b Mann–Whitneynonparametrictest.
c Analysisofvariance(ANOVA)model.
Reported osteoporosis versus radiographic osteoporosis
Radiographic osteoporosis
30.1%
5.3%
69.9% Yes No
94.7%
Reported osteoporosis
Fig.2–Therewasadifferencebetweenthepercentageof
patientswhoreportedhavingosteoporosisandthe
percentagepresentingosteoporosisonradiography,such
thatthepercentageofpatientswithosteoporosisseenon
radiographywasgreaterthanthepercentagereporting
osteoporosis.
Furthermore,thekappacoefficientvaluewaslessthan0.5
(50%),whichindicatesthattherewaslowconcordance
betweenreportedandradiographicosteoporosis.
whohad fractures,whilethe abovementionedserieswas a population-basedstudy.Inaddition,therearestudiesinthe literature,suchastheonebyKootetal.,18thatshowalackof
correlationbetweentheSinghindexanddensitometry. Inde-pendentoftherealprevalenceofosteoporosisinoursample, attentionisdrawntothefactthatonlyonepatientwasusing specific medication for treating this disease (alendronate). Jenningset al.17 conductedan importantsurveyinseveral
hospital services in the United States and concluded that only2%receivedadequatetreatmentforosteoporosisduring hospitalizationandaftertheirrelease.Itisalsonotpartof theroutineatourhospitaltointroducethistypeoftreatment atthismoment.
Theproportionsbetweenthesubtypesoffracturearenot uniform among different series. Ramalho et al.9 reported
that 50.7% were femoral neck fractures and 49.3% were trochanteric fractures.Bentler et al.4 found that 45% were
trochantericfractures.Wefoundthat57.5%weretrochanteric (7.1%subtrochantericand50.4%transtrochanteric)and42.5% wereinthefemoralneck.
Five patients could not be operated, sincetheir clinical conditions made the surgicalrisk very high. Practicallyall the patientswithtranstrochanteric fractures who could be operatedunderwentinternalfixation,asalsodidthosewith stablefracturesofthefemoralneck.Fortyjointreplacements wereperformed:39incasesofunstablefemoralneckfractures andoneinacaseoftranstrochantericfracturewithadvanced arthrosis.Thefirstthingtowhichattentionisdrawnisthefact thatalltheunstablefracturesofthefemoralneckweretreated bymeansofjointreplacementandnoneofthembymeansof reductionandosteosynthesis.However,itneedstobenoted thatoursampleonlyincludedpatientsovertheageof60years, andthatthegreatmajorityofthempresentedosteoporosison radiographyandassociatedcomorbidities.Parkeretal.19
advo-catedhemiarthroplastyinsteadofinternalfixation,forelderly patientswithdisplacedfracturesofthefemoralneck.
Themeandurationofthehospitalstaywas13.5daysand themeanlengthoftimespentwaitingforsurgerywas7days. TheseresultsdidnotdiffermuchfromthoseofotherBrazilian series.Mesquitaetal.2foundameanwaitingtimeof6.8days
andameanhospitalstayof14days.Asturetal.,3atHospital
SãoPaulo,found6.89and10.65.IntheUnitedStates,Bentler etal.4conductedalargestudyandfoundameandurationof
hospitalstayof7.2days.
Many authorshavedefendedtheideathatdelay in per-forming the surgery increases the risk of mortality in the hospital and withinthe firstyear after the operation.2,11,12
These studies drew attention to the problem of excessive delays until surgical intervention at hospitals within the BrazilianNationalHealthSystem.Studiesinothercountries have taken into accountwaiting periods of12, 24 or 48h, whereasourpatientswaitedfor7daysonaverage.
We believe that the precarious state of health of our patientsatthetimeofthefractureanddifficultiesfacedby thehospitalserviceindealingwithcasesarethemaincauses ofdelay.Problemswithinthehospitalservicerelatingtolackof bedsforadmissions,lackofbedsintheintensivecareunitand suspensionofoperationsleadtolongerhospitalstaysduring thisphase.
Typeoffracture,ageandnumberofcomorbiditiesdidnot significantlyaffectthetimespentwaitingforthesurgery.
Thetotal duration ofhospitalstay inBrazilian seriesis muchlongerthanthatinothercountries.Weattributethis prolongedtimenotonlytodelaysinschedulingsurgerybut alsotosocialfactorsandthelackofpublicpoliciesfor postop-erativereceptionofthesepatients.Allthepatientswhowere releasedinourserieswenttotheirownhomeorarelative’s home,while14%ofthepatientsintheseriesofBentleretal. didso.4Theotherswerereceivedintosupportservicesuntil
adefinitivecurehadbeenachieved.Typeoffracture,ageand numberofcomorbiditiesdidnotsignificantlyaffectthelength ofhospitalstay.Thepatientswithunstablefracturesandthose whounderwentjointreplacementstayedinhospitalforlonger times thanthose who underwent fixation.Mesquita etal.2
reported similarresults,but attributedthis longer duration togreateramountsoftimespentonpreoperativepreparation forarthroplastyprocedures.Inourseries,thetypeofsurgery didnotaffectthelengthofthewaitforsurgery.
Eightpatientsdiedduringthehospitalstay(rateof7.1%). Sakakietal.1reportedarateof5.5%inareview.OtherBrazilian
studieshavereportedsimilarrates;Pereiraetal.13 reported
8.9%inRiodeJaneiroandRiccietal.6reported5.45%inRio
GrandedoSul.Inanotherreview,Bentleretal.4reported2.7%
patientwhodiedofpneumoniaafter54daysofhospitalstay. ThishypothesisisadvocatedbyPanulaetal.20
Webelievethatmanyofthefactorsstudiedwerenot statis-ticallysignificantbecauseoflimitationsregardingthesample size.Nonetheless,thevaluesfounddidnotcompletelydiffer fromthoseofthelargeseries.Weneedtocontinueto follow-uptheseindividualsinordertocorrelatethevariablesstudied withmortalitywithinthefirstyearaftersurgery.
Conclusion
The patients attended at this institution present an epi-demiologicalprofilesimilartothosereportedintheBrazilian literature.
Chronic kidney failure is a significant factor relating to deathinthehospital.
Simpleandeffectivepreventivemeasures,suchasearly diagnosisandtreatmentofosteoporosisandregularpracticing ofphysicalactivity,havenotbeenadopted.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SakakiMH,OliveiraAR,CoelhoFF,LemeLEG,SuzukiI, AmatuzziMM.Estudodamortalidadenafraturadofêmur proximalemidosos.ActaOrtopBras.2004;12(4):242–9.
2. MesquitaGV,LimaM,SantosAMR,AlvesELM,BritoJNPO, MartinsMCC.Morbimortalidadeemidososporfratura proximaldofêmur.TextoContextoEnferm.2009;18(1): 67–73.
3. AsturDC,ArlianiGG,BalbachevskyD,FernandesHJA,ReisFB. Fraturadaextremidadeproximaldofêmurtratadasno HospitalSãoPaulo/Unifesp:estudoepidemiológico.RevBras Med.2013;68(4):11–5.
4. BentlerSE,LiuL,ObrizanM,CookEA,WrightKB,GewekeJF, etal.Theaftermathofhipfracture:dischargeplacement, functionalstatuschange,andmortality.AmJEpidemiol. 2009;170(10):1290–9.
5. RochaMA,AzerHW,NascimentoVDG.Evoluc¸ãofuncional nasfraturasdaextremidadeproximaldofêmur.ActaOrtop Bras.2009;17(1):17–21.
6. RicciG,LongarayMP,Gonc¸alvesRZ,UngarettiNetoAS, ManenteM,BarbosaLBH.Avaliac¸ãodataxademortalidade
emumanoapósfraturadoquadrilefatoresrelacionadosà diminuic¸ãodasobrevidanoidoso.RevBrasOrtop.
2012;47(3):304–9.
7.StevensJA,SogolowED.Genderdifferencesfornon-fatal unintentionalfallrelatedinjuriesamongolderadults.Inj Prev.2005;11(2):115–9.
8.HungriaNetoJS,DiasCR,AlmeidaJDB.Características epidemiológicasecausasdafraturadoterc¸oproximaldo fêmuremidosos.RevBrasOrtop.2011;46(6):660–7.
9.RamalhoAC,Lazaretti-CastroM,HauacheO,VieiraJG,Takata E,CafalliF,etal.Osteoporoticfracturesofproximalfemur: clinicalandepidemiologicalfeaturesinapopulationofthe cityofSãoPaulo.SãoPauloMedJ.2001;119(2):48–53.
10.SiqueiraFV,FacchiniLA,PicciniRX,TomasiE,ThuméE, SilveiraDS,etal.Prevalenceoffallsandassociatedfactorsin theelderly.RevSaúdePública.2007;41(5):749–56.
11.BottleA,AylinP.Mortalityassociatedwithdelayinoperation afterhipfracture:observationalstudy.BrMedJ.
2006;332(7547):947–51.
12.SebestyénA,BonczI,SándorJ,NyárádyJ.Effectofsurgical delayonearlymortalityinpatientswithfemoralneck fracture.IntOrthop.2008;32(3):375–9.
13.PereiraSR,PutsMT,PortelaMC,SayegMA.Theimpactof prefractureandhipfracturecharacteristicsonmortalityin olderpersonsinBrazil.ClinOrthopRelatRes.
2010;468(7):1869–83.
14.SinghM,NagrathA,MainiPS.Changesintrabecularpattern oftheupperendofthefemurasanindexofosteoporosis.J BoneJointSurgAm.1970;52(3):457–67.
15.PinheiroMM,CiconelliRM,JacquesNO,GenaroPS,Martini LA,FerrazMB.OimpactodaosteoporosenoBrasil:dados regionaisdasfraturasemhomensemulheresadultos–the BrazilianOsteoporosisStudy(BRAZOS).RevBrasReumatol. 2010;50(2):113–27.
16.BandeiraF,CarvalhoEFD.Prevalênciadeosteoporosee fraturasvertebraisemmulheresnapós-menopausa atendidasemservic¸osdereferência.RevBrasEpidemiol. 2007;10(1):86–98.
17.JenningsLA,AuerbachAD,MaselliJ,PekowPS,Lindenauer PK,LeeSJ.Missedopportunitiesforosteoporosistreatmentin patientshospitalizedforhipfracture.JAmGeriatrSoc. 2010;58(4):650–7.
18.KootVCM,KesselaerSM,CleversGJ,deHoogeP,WeitsT,van derWerkenC.EvaluationoftheSinghindexformeasuring osteoporosis.JBoneJointSurgBr.1996;78(5):831–4.
19.ParkerMJ,KhanRJ,CrawfordJ,PryorGA.Hemiarthroplasty versusinternalfixationfordisplacedintracapsularhip fracturesintheelderly.Arandomisedtrialof455patients.J BoneJointSurgBr.2002;84(8):1150–5.