SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Supination-external
rotation
ankle
fractures:
analysis
of
clinical
results
after
syndesmotic
screw
removal
夽
João
Mendonc¸a
de
Lima
Heck,
Rosalino
Guareschi
Junior,
Luiz
Carlos
Almeida
da
Silva
∗,
Marcelo
Teodoro
Ezequiel
Guerra
HospitalUniversitáriodeCanoas,Servic¸odeOrtopediaeTraumatologia,GrupodePéeTornozelo,Canoas,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19September2016 Accepted6October2016 Availableonline19October2017
Keywords: Anklefractures
Fractureinternalfixation Ankleinjuries
Orthopedicsurgery
a
b
s
t
r
a
c
t
Objective:Toevaluatethepostoperativeresultsofpatientswithsupination-externalrotation anklefractureswhounderwentsyndesmoticscrew(SS)removal.
Methods:Retrospectivecohortstudyassessingthelatepostoperativeresultsof35patients operatedfromJanuary2013toJune2015.Patientsundergoingtreatmentofruptureofthe distaltibiofibularsyndesmosiswithSSfixationandwhodidnothaveanyconcomitant surgicalinjuriesinsitesotherthantheanklewereincluded.Patientswhodidnotcomplete appropriatefollow-upaftersurgerywereexcludedfromthestudy.
Results:Therewasnostatisticalsignificantdifferenceintheevaluatedoutcomesamongthe patientswhohadtheirSSremovedandthosewhoremainedwiththeSS.
Conclusion:SSremovaldidnotsignificantlyaltertheclinicalresultsofpatientssurgically treatedwithSSforsupination-externalrotationfractures.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Fraturas
do
tipo
supinac¸ão-rotac¸ão
externa:
análise
dos
resultados
clínicos
da
retirada
do
parafuso
transindesmoidal
Palavras-chave: Fraturasdotornozelo Fixac¸ãointernadefraturas Traumatismosdotornozelo Cirurgiaortopédica
r
e
s
u
m
o
Objetivo:Avaliaroresultadopós-operatóriodospacientescomfraturadotornozelo pelo mecanismodesupinac¸ão-rotac¸ãoexternaqueforamsubmetidosaretiradadoparafuso transindesmoidal(PT).
Métodos:Estudodecoorteretrospectivoqueavaliouosresultadospós-operatóriostardios de35pacientesoperadosentrejaneirode2013ejunhode2015.Foramincluídospacientes submetidosaotratamentodarupturadasindesmosetibiofibulardistalcomfixac¸ãocom
夽
StudyconductedattheHospitalUniversitáriodeCanoas,Servic¸odeOrtopediaeTraumatologia,GrupodePéeTornozelo,Canoas,RS, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.C.Silva).
http://dx.doi.org/10.1016/j.rboe.2017.10.008
PTequenãoapresentavamlesõescirúrgicasconcomitantesemoutrossítiosquenãoo tornozelo.Pacientesquenãoforamdevidamenteacompanhadosnopós-operatórioforam excluídos.
Resultados:Nãohouvediferenc¸aestatisticamentesignificativanosdesfechosavaliadosentre ospacientesquetiveramoPTremovidoeosquepermaneceramcomoPT.
Conclusão: AretiradadoPTnãoalterousignificativamenteoresultadoclínicodospacientes tratadoscirurgicamentecomPTporfraturasdotiposupinac¸ão-rotac¸ãoexterna.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Anklefracturescanrangefromnon-displacedandavulsion fracturestocomplexfractures,whichrequirereductionand surgicalfixation;thiscanberealizedbydifferentmethods.1
Rotationallesionsarethemostfrequent,andcanbe clas-sifiedaccordingtotheLauge-Hansenclassification;themost common subgroup is fractures caused by the supination-externalrotationmechanism(SER).2Thistypeoffractureis
subdivided into four stages: stage I, lesion of the anterior syndesmosis(anteriortibiofibular ligament)(SER1);stageII, obliquelateralmalleolusfracturewithfracturelinedirection fromanteroinferiortoposterosuperior(SER2);stageIII,lesion ofthe posteriortibiofibularligament orposteriormalleolus fracture(SER3);andstageIV,medialmalleolusfractureor del-toidligamentinjury(SER4).3
Whenananklefractureoccurswithsyndesmoticdiastasis (SD),severalmethodscanbeusedforsurgicalrepair,including syndesmosisfixationwithsyndesmoticscrews(SS).4–6
How-ever,noneofthefixationmethodshaveshowntobesuperior toothers.SS,despitebeingthemostcommonlyusedmethod, alsopresentsfailuresfromboththeclinicaland biomechani-calstandpoints.Oneofthedrawbacksofthisfixationmethod isthatSSremovalisoftennecessary,whichcanleadto addi-tionalcomplications.7,8
Thisstudyisaimedatevaluatingthepostoperativeresults ofpatientswithanklefracturesbytheSERmechanismthat underwentsyndesmoticscrewremoval(SSR).
Material
and
methods
Thisisaretrospectivecohortstudy,whichassessedthelate postoperativeresultsof35patientsoperatedbetweenJanuary 2013andJune2015.ThisstudywasapprovedbytheResearch Ethics CommitteeunderregistrationNo. 117817/2014/CAAE 40153914.4.0000.5328.
Theinclusioncriteriaconsistedofpatientswhounderwent surgicaltreatment byopen reduction and internalfixation of unilateral closed ankle fractures with SER-type trauma mechanism, without other associated fractures, who had undergone preoperative examinations without a cast with bilateralankleradiographywithanteroposterior,mortiseand lateralviews,andwhosignedtheInformedConsentForm.
Exclusioncriteriawere asfollows:patients submittedto conservative treatment of the fracture for reasons unique tothe patientor becausetherewas nosurgicalindication;
associatedfractures;lackofadequateskincondition,edema, and phlyctena in the lateral region of the foot, without resolution until the moment of surgery; ankle fractures by mechanisms other than the SER type; lack of clinical conditionsduetovasculardisorders,cardiopathies,or decom-pensateddiabetes;severetraumaticbraininjury;psychosocial issues; heavy smoking; refusal to undergo surgical treat-ment;bilateralfractures;fixationofthesyndesmosiswithtwo screws,removaloftheone-thirdtubularplateorotherfixation materialorbothinassociationwithSSR;spontaneous break-ingoftheSS;andrefusaltosigntheInformedConsentForm. Duringthisperiod,92feetof75patientsweresubmitted tothesamesurgicaltreatmentforanklefracture with syn-desmoticlesion.Allpatientswerecalledinforreassessment; 35 patientsunderwent surgicaltreatmentwithSS,met the inclusioncriteria,andwereincludedinthestudy.
Allpatientswereassessedbythesamesurgeonwho per-formedthesurgery.TheAmericanOrthopedicFootandAnkle Society(AOFAS),GlobalSocialFunctioningScale(GSFS),visual analog(VAS),andMedicalOutcomesStudy36(SF-36)scales wereused.9
Clinically,the followingaspectswere analyzed:rangeof motion(ROM)oftheankleinflexionandextension,returnto normalactivities,calfdiameter,anklewidth,physicaltherapy duringpostoperativerecovery,andcomorbidities.The Lauge-Hansenclassificationwasusedtocategorizethefractures.2
Likewise,allpatientsunderwentlatepostoperative analy-siswithbilateralankleradiographswithmonopodalsupport inlateralandanteroposteriorviews,andanteroposteriorview with15◦ofinternalrotation.
Thesamplewasdividedintotwogroups,accordingtothe needforSSR.GroupIwascomposedofpatientswhoremained withSS.GroupIIincludedpatientswhounderwentSSR. Indi-cationforSSRwasbasedonthepatient’scomplaintsregarding irritationattheSSfixationsite.
InthesurgicalprocedurefortheinsertionofaSS,patients underwentspinalanesthesia,andwerethenpositionedina dorsalrecumbentposition,withacushionunderthe sacroil-iac region,ipsilateral tothe fracture, and withthe kneeat approximately30◦–45◦offlexion,heldbyamedicalassistant. Preoperatively2gofintravenouscephalothinwere adminis-tered.Thereafter,trichotomyandantisepsiswereperformed withalcoholicchlorhexidine,andsterilesheetswereplaced. ThelimbwassubjectedtovenousdrainagewithanEsmarch bandage,followedbytheapplicationofatourniquetonthe proximalportionofthethigh.Surgerybeganwiththefibula, throughaposterolateralapproach,10fromthedistalendofthe
theplacementofthechosenplate,preservingtheintegrityof thefibulartendonsheathandavoidingextensivedetachment oftheperiosteumandligaments.Subsequently,byamedial approachtothe ankle,10 themedialmalleoluswasreached
fordefinitivetreatmentofboneand/orligamentinvolvement, whenpresent.Theselectedplate wasalwaysthatofsmall fragments(AO one-thirdtubularplate) appliedonthe pos-terolateralaspectofthefibula,oftheshortestpossiblesize; therelationshipwiththefibulartendonsinthedistalportion ofthefibulawasobservedandinterfragmentarycompression wasperformedbyusingacompressionscrew.11
In order to assess the integrity ofthe syndesmosis, an intraoperativecottontestwasperformedbyholdingthefibula withaBackhaustowelclamp,followedbylateraltraction.The stresstestwasconsideredpositivewhenalateral displace-mentgreaterthan3or4mmwasobserved;inthesecases,the syndesmosiswasfixed12 throughtheinsertionofacortical
screw.Orthogonallytotheplate,thescrewisinsertedfrom thefibulatothetibia,withfixationofbothfibularcorticesand onetibialcortex, paralleltothe jointsurface,2–5cmabove itandangled atabout30◦ anteriorly,wheneverpossible,as allowedbythefractureline.
When a deltoid ligament rupture was observed, it was repairedwithabsorbablesurgicalsutures.Themedial malle-olus fracture was reduced and then fixed with a cortical screwforsmallfragments(3.5mm)associatedwitha1.5-mm Kirschnerwirebyusingthetensionbandtechniqueorbyusing twoparallel4-mmcancellousscrews,accordingtothesizeof thefragment.Aftersutureinlayers,thelimbwasimmobilized inacastandkeptelevated.
Patientswere discharged on theday aftersurgery, after radiographyinanteroposteriorandlateralviewsofthe oper-atedankle,withacast;patientsreceivedrecommendationsto keeptheirfootelevated,aswellastousetwocrutchesanda closeddressing.Inthefirstpostoperativeweek,thecastwas removed,adressingwasdone,andanewcastwasmadeat90◦. Inthesecondpostoperativeweek,thestitcheswereremoved, anorthopedicwalkingbootwasprescribed,andphysical ther-apywasinitiated.Sixthweekspostoperatively,anewcontrol radiographwasperformed,andweight-bearingwaspermitted accordingtotolerance.Atthreemonths,incaseofirritative symptomsoftheSS,SSRwasperformed.Inthesixth post-operativemonth,patientsweredischargedfrom outpatient follow-up.
Thequantitative variables were described as mean and standarddeviations;categoricalvariablesweredescribed as single(n)andrelative(%)frequencies.TheShapiro–Wilktest wasusedtoassessthenormalityofdistribution.Toassessthe meandifferencebetweenthetypesofmaterial,thet-testfor independentsamplesortheMann–Whitneytestwereused. Toverify theexistenceofanassociationbetweenthetypes ofmaterialandcategoricalvariables,Fisher’sexacttestwas used.Thesignificancelevelwassetat5%.Thestatistical anal-yseswereperformedwithSPSSversion18.0.
Results
Thepatients wereevaluatedclinicallyandradiographically, andfractureconsolidationwasobservedinallpatientsaround
Table1–Demographicandclinicalcharacteristicsofthe sample.
Variable Removalofthescrew pa
No Yes
Operatedside 1.000
Right 10 67% 5 33%
Left 14 70% 6 30%
Gender 0.721
Male 9 64% 5 36%
Female 15 71% 6 29%
Lauge-Hansenclassification 0.174
SER2 2 67% 1 33%
SER3 12 86% 2 14%
SER4 10 56% 8 44%
Returntoactivities 1.000
No 6 67% 3 33%
Yes 18 69% 8 31%
Comorbidities 0.689
No 18 72% 7 28%
Yes 6 60% 4 40%
Physicaltherapy 0.652
No 4 57% 3 43%
Yes 20 71% 8 29%
Datapresentedasnand%.
a p-ValueforFisher’sexacttest.
thesixthpostoperativeweek.Regardinggender,14weremale and21female;fivemale(36%)andsixfemale(29%)patients underwentSSR(Table1).
Regardingthetypeoftrauma,fivepatientshadtraffic acci-dents, onebyautomobileand four bymotorcycleaccident; ninesufferedsportsinjuries,ofwhomsixwerecausedby soc-cerplayingandthreebyskating;eighthadfallsfromaheight, onebyafallfromahorse,onebyafallfromastaircase,andsix byfallsfromtheirownheight;and13sufferedanklesprains. Amongthosewho underwentSSR,twohad suffereda soc-cerinjury,onewasinvolvedinamotorcycleaccident,three sufferedanklesprain,andthreefromfalls.
Regarding the operated side, 15 underwent right ankle surgery,fiveofwhom(33%)underwentSSR;20underwentleft anklesurgery,sixofwhom(30%)underwentSSR(Table1).
Inthepresentsample,threepatientsunderwentSER2-type trauma,andSSRwasperformedinone(33%);14sufferedSER3, andSSRwasperformedintwo(14%);and18sufferedSER4, and SSRwasperformedineight(44%).Intheevaluationof thereturntothelevelofactivitypriortosurgery,26patients (74%)returned tonormalactivities. Tenpatients (28%)had comorbidities,ofwhomfour(40%)underwentSSR.
Regarding physicaltherapy, seven(28%)didnotundergo physicaltherapy;ofthese,three(43%)underwentSSRandone (9%)presentedsuperficialinfection,whichwasmanagedwith surgicaldebridementandantibiotictherapy.
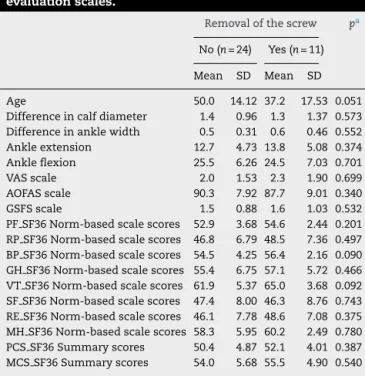
Table2–Resultsofthegroupsinrelationtoage, physicalexaminationmeasurements,andclinical evaluationscales.
Removalofthescrew pa
No(n=24) Yes(n=11)
Mean SD Mean SD
Age 50.0 14.12 37.2 17.53 0.051
Differenceincalfdiameter 1.4 0.96 1.3 1.37 0.573 Differenceinanklewidth 0.5 0.31 0.6 0.46 0.552 Ankleextension 12.7 4.73 13.8 5.08 0.374 Ankleflexion 25.5 6.26 24.5 7.03 0.701 VASscale 2.0 1.53 2.3 1.90 0.699 AOFASscale 90.3 7.92 87.7 9.01 0.340 GSFSscale 1.5 0.88 1.6 1.03 0.532 PFSF36Norm-basedscalescores 52.9 3.68 54.6 2.44 0.201 RPSF36Norm-basedscalescores 46.8 6.79 48.5 7.36 0.497 BPSF36Norm-basedscalescores 54.5 4.25 56.4 2.16 0.090 GHSF36Norm-basedscalescores 55.4 6.75 57.1 5.72 0.466 VTSF36Norm-basedscalescores 61.9 5.37 65.0 3.68 0.092 SFSF36Norm-basedscalescores 47.4 8.00 46.3 8.76 0.743 RESF36Norm-basedscalescores 46.1 7.78 48.6 7.08 0.375 MH SF36Norm-basedscalescores 58.3 5.95 60.2 2.49 0.780 PCS SF36Summaryscores 50.4 4.87 52.1 4.01 0.387 MCSSF36Summaryscores 54.0 5.68 55.5 4.90 0.540
Datapresentedasmeanandstandarddeviation(SD).
a p-ValuefortheMann–Whitneytest.
inclinicaloutcomesbetweenthegroupsubmittedtoSSRin comparisontothegroupthatremainedwiththeSS.
Discussion
Thisstudyevaluatedthepostoperativeoutcomeofpatients submittedtoSSRwhencomparedwiththegroupofpatients whoremainedwithSS.Severalstudieswarnedagainst rou-tineimplantremovalafterfracturehealing,5,6,13,14andSSRis
associatedwithpotentiallyhighcomplicationrates. Further-more,itcannotbepredictedwhetherremovalwillresultin functionalimprovement.15,16
Another argumentagainst routinescrewremoval isthe large amount of resources needed (operating room and time) and economic costs involved (regarding, for exam-ple, secondary surgery, surgery time, and treatment of complications).5,17
Severalauthorshavereportedthephenomenonof recur-rentSDafterSSR;in2011,Hsuetal.4reportedaDSrecurrence
of15%.4,18–20 Inthepresentseries,nocasesofSDafterSSR
wereobserved.
Inthepresent series, theprimary complaintofpatients fortheindicationofSSRwaslocalirritationsymptoms pro-ducedbySSlocatedinthesubcutaneouslayer.Nodifference betweenthecomplaintswasobservedafterSSR;thisfinding isinagreementwithSchepersetal.5andBoyleetal.,21who
demonstratedthatthereisnostatisticaladvantageinSSR. Among patients who underwent SSR, the most posi-tiveeffectsobservedwereanklemobilityimprovementand painreductionindailyactivities. Despitethe improvement reportedbythesepatients,nostatisticallysignificant differ-encewasobservedbetweenthetwogroups.Thus,itcanbe
deductedthatinthegroupofpatientswhounderwentSSR, thereissomebiasinfavoroftheprocedure,incasesinwhich thepatienthim/herselfoptedforSSR.7,21
The time indicated for the SSR varies in the literature between threeand sixmonths.18,19 Atthis medicalcenter,
SSRswereperformedatthreemonths,withnoserious out-comesinthepresentseries.
In recentliterature,differentclinical assessment instru-ments have been used to evaluate clinical outcomes in patientswithanklefractures.Generally,theAOFASscale,VAS, SF-36,GSFS,andphysicalexaminationoftheankleROMare used.TheOlerudandMolander22scoreshavealsobeenused
incurrentliterature.21,23However,thisscorewasnotincluded
inthepresentstudy;inturn,theAOFASscorewaspreferred,as itallowsanassociatedobjectiveandsubjectiveevaluation.In thepresentstudy,theresultsofthedifferentinstrumentsused werestatisticallysimilarbetweenthetwogroupsanalyzed.
Themainlimitationofthepresentstudyisitsretrospective natureandthesmallsample,duetothefactthatourhospital attendstohighlycomplexpatients,manywithmultiple frac-tures,whichwerenotincludedintheanalysis.Furthermore, inthepresentstudy,theuseofprophylacticantibioticsduring SSRwasnotincludedintheanalysisbecause,atthetimeof surgery,itwasnotaroutinepracticeatthishospitaltouse prophylacticantibioticsinthistypeofsurgery.
Conclusion
SSRdoesnotsignificantlyaltertheclinicaloutcomeofpatients surgicallytreatedwithSSduetoSER-typefractures.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.TejwaniNC,ParkJH,EgolKA.Supinationexternalrotation anklefractures:asimplerpatternwithbetteroutcomes. IndianJOrthop.2015;49(2):219–22.
2.Lauge-HansenN.Fracturesoftheankle.II.Combined experimental-surgicalandexperimental-roentgenologic investigations.ArchSurg.1950;60(5):957–85.
3.SinghR,KamalT,RoulohaminN,MaoharanG,AhmedB, TheobaldP.Anklefractures:aliteraturereviewofcurrent treatmentmethods.OpenJOrthop.2014;4(11):292–303.
4.HsuYT,WuCC,LeeWC,FanKF,TsengIC,LeePC.Surgical treatmentofsyndesmoticdiastasis:emphasisoneffectof syndesmoticscrewonanklefunction.IntOrthop. 2011;35(3):359–64.
5.SchepersT,VanLieshoutEM,deVriesMR,VanderElstM. Complicationsofsyndesmoticscrewremoval.FootAnkleInt. 2011;32(11):1040–4.
6.SchepersT.Toretainorremovethesyndesmoticscrew:a reviewofliterature.ArchOrthopTraumaSurg.
2011;131(7):879–83.
8. ReganDK,GouldS,ManoliA,EgolKA.Outcomesovera decadeaftersurgeryforunstableanklefracture:functional recoveryseen1yearpostoperativelydoesnotdecaywith time.JOrthopTrauma.2016;30(7):e236–41.
9. SooHooNF,VyasR,SamimiD.Responsivenessofthefoot functionindex,AOFASclinicalratingsystems,andSF-36after footandanklesurgery.FootAnkleInt.2006;27(11):
930–4.
10.ErdemMN,ErkenHY,BurcH,SakaG,KorkmazMF,Aydogan M.Comparisonoflagscrewversusbuttressplatefixationof posteriormalleolarfractures.FootAnkleInt.
2014;35(10):1022–30.
11.TucciNetoC,FernandesHJ,TucciNetoPF,dosReisFB, FaloppaF.Tratamentodefraturasdotornozelotipo
Danis-WeberBcomplacaantideslizantepóstero-lateral.Rev BrasOrtop.2003;38(6):320–8.
12.vandenBekeromMP.Diagnosingsyndesmoticinstabilityin anklefractures.WorldJOrthop.2011;2(7):51–6.
13.BusamML,EstherRJ,ObremskeyWT.Hardwareremoval: indicationsandexpectations.JAmAcadOrthopSurg. 2006;14(2):113–20.
14.NaumannMG,SigurdsenU,UtvagSE,StavemK.Incidence andriskfactorsforremovalofaninternalfixationfollowing surgeryforanklefracture:aretrospectivecohortstudyof997 patients.Injury.2016;47(8):1783–8.
15.OncheII,OsagieOE,INuhuS.Removaloforthopaedic implants:indications,outcomeandeconomicimplications.J WestAfrCollSurg.2011;1(1):101–12.
16.vanVlijmenN,DenkK,vanKampenA,JaarsmaRL. Long-termresultsafteranklesyndesmosisinjuries. Orthopedics.2015;38(11):e1001–6.
17.GougouliasN,KhannaA,SakellariouA,MaffulliN. Supination-externalrotationanklefractures:stabilityakey issue.ClinOrthopRelatRes.2010;468(1):243–51.
18.GennisE,KoenigS,RodericksD,OtlansP,TornettaP3rd.The fateofthefixedsyndesmosisovertime.FootAnkleInt. 2015;36(10):1202–8.
19.TuckerA,StreetJ,KealeyD,McDonaldS,StevensonM. Functionaloutcomesfollowingsyndesmoticfixation:a comparisonofscrewsretainedinsituversusroutineremoval. Isitreallynecessary?Injury.2013;44(12):1880–4.
20.vandenBekeromMP,KloenP,LuitseJS,RaaymakersEL. Complicationsofdistaltibiofibularsyndesmoticscrew stabilization:analysisof236patients.JFootAnkleSurg. 2013;52(4):456–9.
21.BoyleMJ,GaoR,FramptonCM,ColemanB.Removalofthe syndesmoticscrewafterthesurgicaltreatmentofafracture oftheankleinadultpatientsdoesnotaffectone-year outcomes:arandomisedcontrolledtrial.BoneJtJ. 2014;96-B(12):1699–705.
22.OlerudC,MolanderH.Ascoringscaleforsymptom evaluationafteranklefracture.ArchOrthopTraumaSurg. 1984;103(3):190–4.