w w w . r b o . o r g . b r
Original
article
Is
there
a
difference
in
the
positioning
of
sliding
screws
between
stable
and
unstable
extracapsular
fractures?
夽
Pedro
José
Labronici
a,∗,
Rodrigo
Freitas
da
Silva
a,
Ana
Maria
Santos
Viana
a,
Saulo
Santos
Blunck
a,
José
Sergio
Franco
b,
Sergio
Ricardo
Neto
a,
Robinson
Esteves
Santos
Pires
c,d,
Roberto
Canto
eaProf.Dr.DonatoD’ÂngeloOrthopedicsandTraumatologyService,HospitalSantaTeresa,Petrópolis,RJ,Brazil
bDepartmentofOrthopedicsandTraumatology,SchoolofMedicine,FederalUniversityofRiodeJaneiro,RiodeJaneiro,RJ,Brazil cFederalUniversityofMinasGerais,BeloHorizonte,MG,Brazil
dHospitalFelícioRocho,BeloHorizonte,MG,Brazil eUniversityofUberlândia,Uberlândia,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received3January2014 Accepted27February2014 Availableonline24February2015
Keywords:
Femoralfractures Hipfractures Bonescrews
a
b
s
t
r
a
c
t
Objective:Toanalyzethetip–apexdistance(TAD),cervicodiaphysealangleandGardenangle instableandunstableextracapsularfracturesofthefemurtreatedwithaplateandsliding screw.
Method:Hipradiographsinanteroposterior(AP)andlateralviewon117patientswere eval-uated.Thefractureswereclassifiedasstableorunstable,usingtheAOclassification,and thereductionachievedwasassessedinaccordancewiththefollowingcriteria:TAD>3cm; Gardenalignmentindex(AP)<160◦;andAPcervicodiaphysealvarusangle<125◦.Whentwo
ormorecriteriawerepresent,thequalityoftheosteosynthesiswasclassifiedas“notideal”.
Results:ThepatientswithunstablefracturespresentedAPcervicodiaphysealanglesthat weresignificantlygreater(p=0.05)thaninthosewithstablefractures.Thepatientswith unstablefracturespresentedlateralcervicodiaphysealanglesthatweresignificantlysmaller (p=0.05)thaninthosewithstablefractures.Therewerenosignificantdifferencesinthe remainderofthecriteriaevaluated.
Conclusion:Thisstudydidnotfindanysignificantdifferencesinthemeasurements evalu-ated,exceptinrelationtothecervicodiaphysealangle.Satisfactoryreductionwasachieved bothforthestableandfortheunstablefractures,whenweusedaplateandslidingscrew totreatproximalextracapsularfracturesofthefemur.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedattheProf.Dr.DonatoD’ÂngeloOrthopedicsandTraumatologyService,HospitalSantaTeresa,andatthePetrópolis SchoolofMedicine,Petrópolis,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](P.J.Labronici).
http://dx.doi.org/10.1016/j.rboe.2015.02.002
Existe
diferenc¸a
no
posicionamento
do
parafuso
deslizante
entre
as
fraturas
extracapsulares
estáveis
e
instáveis?
Palavras-chave:
Fraturasdofêmur Fraturasdoquadril Parafusosósseos
r
e
s
u
m
o
Objetivo: Analisaradistânciaponta-ápice(DPA),oângulocervicodiafisárioeoângulode Gardenemfraturasextracapsularesinstáveiseestáveisdofêmurtratadascomplacae parafusodeslizante.
Método: Foramavaliadasradiografiasdoquadrilnasincidênciasemanteroposterior(AP) eperfilde117pacientes.Asfraturasforamclassificadascomoestáveiseinstáveis,pela classificac¸ãoAO,eareduc¸ãoobtidafoiavaliadadeacordocomoscritériosdedistância ponta-ápice(DPA>3cm),índicedealinhamentodeGarden(AP)<160◦eângulo
cervicodi-afisário(AP)emvaro<125◦.Quandodoisoumaiscritériosestavampresentes,aqualidade
daosteossíntesefoiclassificadacomo«nãoideal».
Resultados: OspacientescomfraturainstávelapresentaramCDAP(p=0,05) significativa-mentemaiordoqueosestáveis.Ospacientescomfraturainstável apresentaramoCD Perfil(p=0,05)significativamentemenordoqueoscomfraturaestável.Nãohouvediferenc¸a significativaentreorestantedoscritériosavaliados.
Conclusão: Esteestudonãoencontroudiferenc¸asignificativaentreasmedidasavaliadas, excetooângulocervicodiafisário.Foiconseguidaumareduc¸ãosatisfatória,tantonas frat-urasestáveiscomonasinstáveis,quandousamosplacaeparafusodeslizantenasfraturas proximaisextracapsularesdofêmur.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Plates and sliding screwsare currently the implants most oftenusedforfixation ofintertrochantericfractures ofthe femur.1Thisisbecauseofanintrinsiccharacteristicoftheir
design,whichmakesitpossibletocollapsethefracturewith controlledimpactionintoastableposition,while maintain-ingaconstantcervicodiaphysealangle,withoutpenetration ofthefemoralhead.2–4 Theplateandslidingscrewjointhe
limbtogetherwithoutmakingcuts,soastoresistpenetration andthethreadedscrewincreasesthefixationintheproximal fragment.Thegreatadvantageofthisisthatthescrewcan beinserteddeeplywithoutanydangerthatthejointmight becomeperforatedlateron,althoughtheplacementneedsto bepreciseinordertoavoidfailures.5
Themostcommon cause offailure offixationof extra-capsular fractures that are treatedwith plates and sliding screwsrelatestosituationsinwhichthescrewinthefemoral headcutsout.The incidenceofthissituation ranges from 5.3%to16.8%.1,2,6–8Itoccurswhenthecervicodiaphysealangle
collapsesinvarusandthethreadedscrewextrudessuperiorly throughthefemoralhead.2,3Baumgaertneretal.2introduced
theconceptofthetip–apexdistance(TAD)asastrong progno-sticfactorforthiscomplication.
TADwasdefinedbyBaumgaertneret al.2 asthesumof
thedistanceinmillimeters, onradiographsin anteroposte-rior(AP)andlateralviews,fromthetipofthethreadedscrew to the apex of the femoral head, with appropriate correc-tionformagnification.2,6,9IthasbeendemonstratedthatTAD
greaterthan2.5cmisassociatedwithincreasedriskofimplant failure2,6,9 with greater occurrenceofcut-out.1–3,6,9,10 Some
studieshavesuggestedthatvalueslowerthan2cmoughtto betheideal.1
TheaimofthepresentstudywastoanalyzeTAD, cervi-codiaphysealangleandGardenangleinstableandunstable extracapsularfracturestreatedwithaplateandslidingscrew.
Materials
and
methods
BetweenMay1998andJuly2011,408patientswithunstable and stableextracapsular fractures ofthefemurunderwent surgicaltreatmentbymeansofreductionandfixationusing aplateandslidingscrewatHospitalSantaTeresa, Petrópo-lis,stateofRiode Janeiro.Amongthese,291patientswere excludedbecausetheypresentedradiographswithincorrect viewsordidnotpresentoneoftheviewsneededfor analy-sisontheTADmeasurements;orbecausetheywereunder60 yearsofage;orbecausetheypresentedpathologicalfractures andtreatmentwithcephalomedullarynails.Allthepatients wereoperatedonatractiontable.
Thetechnicalqualityoftheosteosynthesiswasanalyzed by means of observation and using radiographs produced during the immediate postoperative period. According to Baumgaertneretal.2,6 TADwasdescribedasthesumofthe
Fig.1–Stableintertrochantericfractureofthefemurtreatedwithaplateandslidingscrew.
indicatesthedegreeofrotationofthefemoralhead.Inthe anteroposterior projection, the cervicocephalic trabeculae formanangleof160–175◦ withthemedialcorticalboneof
thefemoraldiaphysis;inthelateralprojection,thealignment ofthetrabeculaeshouldbe180◦.FromtheGardenalignment
index,adequatereductionistakentobeatrabecularangleof between160◦and180◦,bothinAPandinlateralview.
TheAOclassificationforhipfractureswasused,12andthis
wassubdividedintostablefractures(31A1)orunstable frac-tures(31A2)(Figs.1and2).Thequalityoftheosteosynthesis wasclassifiedas“ideal”or“notideal”,inaccordancewiththe followingcriteria:(1)TAD>3cm;(2)Gardenalignmentindex (AP)<160◦;and(3)cervicodiaphysealangle(AP)invarus<125◦.
Whentwoormorecriteriawerepresent,thequalityofthe osteosynthesiswasclassifiedas“notideal”.
Table1presentsthecharacterizationofthemean,standard
deviation(SD),medianandminimumandmaximumofthe numericalvariablesofthetotalsampleofthisstudy.
Amongthe 117 records examined, 74 (63.2%) related to unstablefractures,59(50.4%)tofracturesontherightsideand 66(56.4%)tofracturesinfemales.
Table1–Descriptionofthenumericalvariablesinthe
totalsample.
Variable Mean SD Median Minimum Maximum
AP 1.21 0.43 1.20 0.20 2.50
Lateral 1.18 0.44 1.10 0.10 2.20
TAD 2.39 0.84 2.20 0.30 4.10
GardenAP 162.7 8.4 162 125 178
Gardenlateral 173.1 4.8 174 160 180
CDAP 135.5 11.3 134 112 170
CDlateral 171.5 5.8 172 150 180
Source:HospitalSantaTeresa,Petrópolis,stateofRiodeJaneiro, Brazil.
SD,standarddeviation;AP,anteroposterior;TAD,tip–apexdistance; CD,cervicodiaphysealangle.
Statistical
methodology
Thedescriptiveanalysispresentedtheobserveddataintables, intheformofmeans,standarddeviationsandmedians.
The inferential analysis consistedofthe nonparametric Mann–Whitney test for comparing the numerical variables betweenthesubgroupsofstableandunstablefracturesand the2(Chi-square)testforcategoricalvariables.
A nonparametric method was used because the vari-ables didnotpresent normal(Gaussian) distribution,given that the hypothesis ofnormality wasrejected through the Kolmogorov–Smirnovtest.
Thecriterion used fordeterminingsignificancewas the levelof5%.Thestatisticalanalysiswasprocessedusingthe SAS6.11software(SASInstitute,Inc.,Cary,NC,USA).
Results
Toshowanydifferencesamongthestudyvariables,Table2
presents themeans,standard deviations(SD)andmedians of the variables according to stability (unstable or stable) and the corresponding descriptive level (p-value) from the Mann–Whitneytest.
Itwasobservedthattherewerenosignificantdifferences inthevariablesstudiedbetweenthetwogroupsoffractures, asillustratedinFigs.3–5.
Fig.2–Unstableintertrochantericfractureofthefemurtreatedwithaplateandslidingscrew.
similartothatofthesubgroupwithstablefractures(60.5%), withp=0.50.
It was also observed that there were differences in the study variables between the two groups of fractures (unstableand stable),separately accordingto side(rightor left).
Tables 3 and 4 presented the means, standard
devia-tions(SD)andmediansofthevariablesaccordingtostability (unstableorstable)andthecorrespondingdescriptivelevels (p-values) ofthe Mann–Whitney test,for theleft and right sides,respectively.
Itwasobservedthatthepatientswithunstablefractures presented AP cervicodiaphyseal angles that were signifi-cantlygreaterthanthoseofthepatientswithstablefractures (p=0.05),asshowninFig.6.Therewerenostatistically sig-nificantdifferencesin theother variables betweenthetwo subgroups.
Itwasalsoseenthatthepatientswithunstablefractures presentedlateralcervicodiaphysealanglesthatwere signifi-cantlysmallerthanthoseofthepatientswithstablefractures
Stable fracture Unstable fracture
180
170
160
150
140
130
120
Garden (degrees)
Lateral AP
Fig.3–Comparisonbetweenstableandunstablefractures usingtheGardenangle.
Table2–Analysisonvariablesaccordingtostability.
Variable Unstable(n=74) Stable(n=43) p-Valuea
Mean±SP Median Mean±SD Median
AP 1.23±0.43 1.2 1.17±0.43 1.2 0.58
Lateral 1.22±0.44 1.1 1.11±0.45 1 0.19
TAD 2.45±0.83 2.2 2.28±0.85 2.2 0.33
GardenAP 163.0±8.8 164 162.1±7.9 162 0.32
Gardenlateral 172.8±5.0 174 173.7±4.4 174 0.44
CDAP 135.6±11.6 133 135.5±10.8 134 0.87
CDlateral 170.7±6.5 170 172.9±4.1 172 0.093
Source:HospitalSantaTeresa,Petrópolis,stateofRiodeJaneiro,Brazil.
Table3–Analysisonthevariablesaccordingtothestabilityoftherightside.
Variable Unstable(n=41) Stable(n=18) p-Valuea
Mean±SP Median Mean±SP Median
AP 1.20±0.44 1.2 1.13±0.37 1.15 0.66
Lateral 1.17±0.40 1 1.04±0.36 1.05 0.38
TAD 2.37±0.79 2.2 2.17±0.67 2.25 0.46
GardenAP 164.3±7.2 164 161.9±6.3 162 0.21
Gardenlateral 173.1±4.9 174 173.6±4.3 174.5 0.81
CDAP 137.0±11.4 135 131.4±7.6 128 0.053
CDlateral 171.9±5.4 172 172.9±3.7 172.5 0.50
Source:HospitalSantaTeresa,Petrópolis,stateofRiodeJaneiro,Brazil.
AP,anteroposterior;TAD,tip–apexdistance;CD,cervicodiaphysealangle;SD,standarddeviation. a Mann–Whitneytest.
Stable fracture Unstable fracture
180
170
160
150
140
130
120
110
100
CD (degrees)
Lateral AP
Fig.4–Comparisonbetweenstableandunstablefractures usingthecervicodiaphysealangle(CD).
(p=0.05),asshowninFig.6.Therewerenostatistically sig-nificantdifferences intheother variables betweenthe two subgroupsofpatients.
Stable fracture Unstable fracture
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
TAD
Fig.5–Comparisonbetweenstableandunstablefractures usingthetip–apexdistance(TAD).
The subgroup with unstable fractures was seen to present lateral cervicodiaphyseal angles that were signifi-cantlysmallerthanthoseofthesubgroupwithstablefractures (p=0.05),asshowninFig.7.Therewerenostatistically
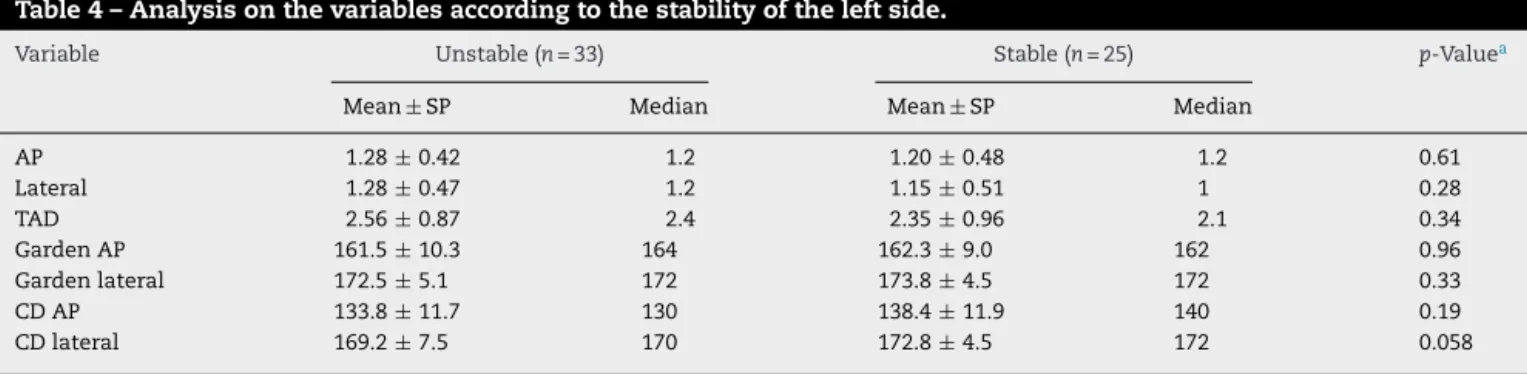
sig-Table4–Analysisonthevariablesaccordingtothestabilityoftheleftside.
Variable Unstable(n=33) Stable(n=25) p-Valuea
Mean±SP Median Mean±SP Median
AP 1.28±0.42 1.2 1.20±0.48 1.2 0.61
Lateral 1.28±0.47 1.2 1.15±0.51 1 0.28
TAD 2.56±0.87 2.4 2.35±0.96 2.1 0.34
GardenAP 161.5±10.3 164 162.3±9.0 162 0.96
Gardenlateral 172.5±5.1 172 173.8±4.5 172 0.33
CDAP 133.8±11.7 130 138.4±11.9 140 0.19
CDlateral 169.2±7.5 170 172.8±4.5 172 0.058
Source:HospitalSantaTeresa,Petrópolis,stateofRiodeJaneiro,Brazil.
Stable fracture Unstable fracture
180
175
170
165
160
155
150
145
140
135
130
125
CD (degrees)
Lateral AP
Fig.6–Comparisonbetweenstableandunstablefractures usingthecervicodiaphysealangle(CD),rightside.
Stable fracture Unstable fracture
180
175
170
165
160
155
150
145
140
135
130
125
CD
(degrees)
Lateral AP
Fig.7–Comparisonbetweenstableandunstablefractures usingthecervicodiaphysealangle(CD),leftside.
nificantdifferencesin theother variables betweenthetwo subgroupsatthe5%level.
Fig.8showstheincidenceofthestableandunstable frac-turesrelatingtothe117patientsanalyzed.
Fig.9showstheidealandnon-idealreductionsinthestable andunstablefractures.
Itwasseenthat79%ofthestablefracturesand81%ofthe unstablefracturespresentedidealreductions.
Discussion
Inoursetting,themajorityofintertrochantericfracturesare still treated using plates and sliding screws. The success of treatments using this type of implant depends on the impactionofthe headand necksegments intheproximal
0% 10% 20% 30% 40% 50% 60% 70%
Stable n=43 Unstable n=74
Stable n=43 Unstable n=74
Fig.8–Comparisonofabsolutenumbersbetweenstable andunstablefractures.
regionofthefemur,intoastableposition.Afterthishasbeen achieved,theloadonthefracturewillbesharedbetweenthe boneandimplantandthebonewillabsorbapproximately75% ofthe load transmitted.13 Kaufer14 described fivevariables
thatcouldaffecttheresistanceofthecombinationofimplant andfracturefragment:(1)bonequality;(2)fragment geome-try;(3)fracturereduction;(4)implantmodel;and(5)implant choice.Amongthese,thelastthreeareunderthecontrolof thesurgeon.Accordingtotheliterature,complications relat-ingtotheplateandslidingscrewoccurinaround16–23%of thecases.Therefore,adequateplacementofthescrewis fun-damentallyimportant.15–17Thesecomplicationsmayinclude
lossofthereduction,pseudarthrosis,skewedconsolidation withvarusdeformityofthefemoralneck,shorteningorscrew cut-out.7,16,18–23Ourmainobjectiveherewastoanalyzethe
positionsoftheplate andslidingscrewthroughcomparing stableandunstableintertrochantericfractures.
Despitethemechanicaladvantagesofplatesand sliding screws,slidingscrewcut-outremainsasignificantproblem, especially incasesof unstable fractures.However,internal
0 10 20 30 40 50 60 70 80
Stable Unstable
Non-ideal reduction Ideal reduction
fixationofstableintertrochantericfractureshasshownlow incidenceofcomplications.5,7,24
Many authors have triedto quantify the positioning of theslidingscrew.25–27Clawson5recommendedthatthescrew
should be placed6mm from the subchondral bone. Some authorshavedescribedthelocationofthescrewinrelation tothedistancefromthecentralaxisofthefemoralheadand neck,onAPandlateralradiographs.25–27Thescrew
penetra-tiondepth hasbeen calculatedaccordingtothenumber of turnsthatwouldbeneededtoadvancethescrewinsidethe bone.Thenine-zonesystemusedbyKyleetal.24didnot
rep-resentthescrewpenetrationdepth.Larssonetal.28tookinto
considerationthedirectionanddepthofthescrewanddivided thefemoralheadintoperpendicularaxesandtheremaining quadrantsinto11 zonesinbothradiographs.Bridleet al.29
usedsimilaraxes,butdividedeachradiographintonineareas. Parker30usedaproportionaltechniquefordefiningthe
direc-tionofthescrew,butnotitsdepth,inbothradiographicviews. The two mainmethods forquantifying the positioning ofthe screwthathavebeendescribed are theproportional methoddescribedbyParker30andthetip–apexdistance(TAD)
methoddescribedbyBaumgaertneretal.,apudEvans31and
Garden.32Thelattermethodhasbeenshowntobeauseful
intraoperativeindicatorforscrewpositioningatdepthandfor centralplacementinthe femoralhead.Thisisperhapsthe mostimportantindicatorforpreciseplacementofthescrew and hasbeen shown in several studies tohave prognostic value after treatments for intertrochanteric fractures.2,17,33
TAD<2.5cmhasbeenreportedtorepresentagood progno-sisfortheresults.However,somestudieshavetakentheview thattheidealwouldbeTAD<2cm.2,17,33
Several authors have reported that failures are practi-cally nonexistent in relation to fixation of stable two-part intertrochantericfractures.7,34Themostcommonmechanical
complicationafterusingaplateandslidingscrewis progres-sivecollapseinvarusthroughthefemoralhead,withproximal migrationandpossiblyscrewcut-outinthehead.6,7Adequate
positioningofthescrewinsidetheheadprotectsagainstthese complications.6,7 Nonetheless, divergencesofopinion exist
inrelationtoinstability.26,34–36LindskogandBaumgaertner37
demonstratedthatageandunstablefractureswerealso inde-pendent factors for a prognosis of cut-out. Baumgaertner etal.6 reportedcut-outratesrangingfrom 4%to20%,with
higherratesinunstable fractures.Haidukewych38 reviewed
unstablefractures (AO/OTAtypesA3.1 andA3.3)and found complicationrates ofup to56% (consistingof cut-outand pseudarthrosis)whenaplate and slidingscrewwere used. Ourresultsshowedthattherewasnosignificantdifference inTADbetweenstablefractures (2.28±0.85cm) and unsta-blefractures(2.45±0.83cm).OurTADresultsof2.39±0.84cm remainedwithinthelimitdeterminedbyBaumgaertner,i.e. below2.5cm.OurdatadonotsupportthehypothesisthatTAD mightbehigher(therebyfavoringcomplications)incasesof unstablefracturesbecauseofpossibledifficultyinreducing suchfractures.
Studiesoncadaversandradiographicstudieshave demon-stratedthatthemeancervicodiaphysealangleinthegeneral populationis127±7◦.39,40 Nosignificantdifferencesin
rela-tion to side and gender have been demonstrated, despite culturaldifferences.41TheAPradiographicevaluationofthe
cervicodiaphysealanglewasshowntobemoreprecisewhen thefemurwasinternallyrotatedat10◦,giventhatexternal
rotationmightleadtoanapparentincreaseinthe cervicodi-aphysealangle.42Thepresentstudydemonstratedthatgood
reductionisanimportantfactorforavoidingcomplications. However,sincenointra-orinterobservercomparisonswere made,wecannotconcludethattherewasnosignificant differ-enceincervicodiaphysealangleonAPradiographs,between stableand unstablepatients(135.5±10.8◦ and135.6±11.6◦,
respectively),oronlateral-viewradiographs(172.9±4.1◦ and
170.7±6.5◦,respectively).
Somestudieshaveindicatedthatcorrectreductionof frac-tures seenonradiographs, especiallyinAPview,and good correctionofthetrabecularangletoaround165–170◦are
asso-ciatedwithreductionoftheriskofcut-out.41,43Pervezetal.1
confirmedthevalueoffracturereductiononradiographsinAP view,withanincreaseincut-outratesincasesoffracturesthat had beenreducedinvarus.Fracture reductionand implant positioningaredirectlyrelated.Therefore,correctreduction ofthefractureisaprerequisiteforimplantplacement.44
WeobservedthatthecervicodiaphysealangleinAPview wassignificantlygreaterinunstablefracturesandthatthere wasatendencytowardreductioninvalgus.Wealsoobserved inlateral viewthat thecervicodiaphysealanglewas signif-icantly smallerinunstable fractures,which suggestedthat therewasatendencytowardposteriorcollapse.
Conclusion
Theresultsfromthisstudyconfirmedthatthereareno sig-nificant differences between the measurements evaluated, exceptthecervicodiaphysealangle.Moreover,bothforstable andforunstablefractures,goodreductionisanimportant fac-torforavoidingcomplicationswhenplatesandsidingscrews areusedforextracapsularfracturesofthefemur.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.PervezH,ParkerMJ,VowlerS.Predictionoffixationfailure
afterslidinghipscrewfixation.Injury.2004;35(10):994–8.
2.BaumgaertnerMR,CurtinSL,LindskogDM,KeggiJM.The
valueofthetip–apexdistanceinpredictingfailureoffixation
ofperitrochantericfracturesofthehip.JBoneJointSurgAm.
1995;77(7):1058–64.
3.LorichDG,GellerDS,NielsonJH.Osteoporoticpertrochanteric
hipfractures:managementandcurrentcontroversies.Instr
CourseLect.2004;53:441–54.
4.JacobsRR,ArmstrongHJ,WhitakerJH,PazellJ.Treatmentof
intertrochanterichipfractureswithacompressionhipscrew
andanailplate.JTrauma.1976;16(8):599–603.
5.ClawsonDk.Trochantericfracturestreatedbythesliding
screwplatefixationmethod.JTrauma.1964;4:737–52.
6.BaumgaertnerMR,SolbergBD.Awarenessoftip–apex
distancereducesfailureoffixationoftrochantericfractures
7. DavisTR,SherJL,HorsmanA,SimpsonM,PorterBB,
CheckettsRG.Intertrochantericfemoralfractures.Mechanical
failureafterinternalfixation.JBoneJointSurgBr.
1990;72(1):26–31.
8. JensenJS,TøndevoldE,MossingN.Unstabletrochanteric
fracturestreatedwiththeslidingscrew-platesystem.A
biomechanicalstudyofunstabletrochantericfracturesIII.
ActaOrthopScand.1978;49(4):392–7.
9. StapleySA,KumarBA,ParkerMJ.Thepredictionoffixation
failureofintertrochantericfracturesofthefemurusingthe
slidinghipscrew:whichisthebestmethod?JBoneJointSurg
Br.2000;82Suppl.1:56.
10.WaltonNP,Wynn-JonesH,WardMS,WimhurstJA.Femoral
neck-shaftangleinextra-capsularproximalfemoralfracture
fixation:doesitmakeaTADofdifference?Injury.
2005;36(11):1361–4.
11.LyTV,SwiontkowskiMF.Treatmentoffemoralneckfractures
inyoungadults.JBoneJointSurgAm.2008;90(10):2254–66.
12.MarshJL,SlongoTF,AgelJ,BroderickJS,CreeveyW,DeCoster
TA,etal.Fractureanddislocationclassificationcompendium
–2007:OrthopaedicTraumaAssociationclassification,
database,andoutcomescommittee.JOrthopTrauma.2007;21
Suppl.10:S1–133.
13.FrankelVH,BursteinAH.Orthopedicsbiomecanics.The
applicationofengineeringtothemusculoskeletalsystem.
Philadelphia:LeaandFebiger;1970.
14.KauferH.Mechanicsofthetreatmentofhipinjuries.Clin
OrthopRelatRes.1980;(146):53–61.
15.BannisterGC,GibsonAG,AckroydCE,NewmanJH.The
fixationandprognosisoftrochantericfractures.A
randomizedprospectivecontrolledtrial.ClinOrthopRelat
Res.1990;(254):242–6.
16.SimpsonAH,VartyK,DoddCA.Slidinghipscrews:modesof
failure.Injury.1989;20(4):227–31.
17.WolfgangGL,BryantMH,O’NeillJP.Treatmentof
intertrochantericfractureofthefemurusingslidingscrew
platefixation.ClinOrthopRelatRes.1982;(163):148–58.
18.KauferH,MatthewsLS,SonstegardD.Stablefixationof
intertrochantericfractures.JBoneJointSurgAm.
1974;56(5):899–907.
19.KyleRF.Fracturesoftheproximalpartofthefemur.JBone
JointSurgAm.1994;76:924–50.
20.MadsenJE,NaessL,AuneAK,AlhoA,EkelandA,StrømsøeK.
Dynamichipscrewwithtrochantericstabilizingplateinthe
treatmentofunstableproximalfemoralfractures:a
comparativestudywiththeGammanailandcompression
hipscrew.JOrthopTrauma.1998;12(4):241–8.
21.LiuM,YangZ,PeiF,HuangF,ChenS,XiangZ.Ameta-analysis
oftheGammanailanddynamichipscrewintreating
peritrochantericfractures.IntOrthop.2010;34(3):323–8.
22.NordinS,ZulkifliO,FaishamWI.Mechanicalfailureof
dynamichipscrew(DHS)fixationinintertrochanteric
fractureofthefemur.MedJMalaysia.2001;56Suppl.D:12–7.
23.SaarenpääI,HeikkinenT,RistiniemiJ,HyvönenP,LeppilahtiJ,
JalovaaraP.Functionalcomparisonofthedynamichipscrew
andtheGammalockingnailintrochanterichipfractures:a
matched-pairstudyof268patients.IntOrthop.
2009;33(1):255–60.
24.KyleRF,GustiloRB,PremerRF.Analysisofsixhundredand
twenty-twointertrochanterichipfractures.JBoneJointSurg
Am.1979;61(2):216–21.
25.DohertyJHJr,LydenJP.Intertrochantericfracturesofthehip
treatedwiththehipcompressionscrew:analysisof
problems.ClinOrthopRelatRes.1979;(141):184–7.
26.GreiderJLJr,HorowitzM.Clinicalevaluationofthesliding
compressionscrewin121hipfractures.SouthMedJ.
1980;73(10):1343–8.
27.MulhollandRC,GunnDR.Slidingscrewplatefixationof
intertrochantericfemoralfractures.JTrauma.
1972;12(7):581–91.
28.LarssonS,FribergS,HanssonLI.Trochantericfractures.
Mobility,complications,andmortalityin607casestreated
withthesliding-screwtechnique.ClinOrthopRelatRes.
1990;(260):232–41.
29.BridleSH,PatelAD,BircherM,CalvertPT.Fixationof
intertrochantericfracturesofthefemur.Arandomised
prospectivecomparisonoftheGammanailandthedynamic
hipscrew.JBoneJointSurgBr.1991;73(2):330–4.
30.ParkerMJ.Cutting-outofthedynamichipscrewrelatedtoits
position.JBoneJointSurgBr.1992;74(4):625.
31.EvansEM.Trochantericfractures;areviewof110cases
treatedbynail-platefixation.JBoneJointSurgBr.
1951;33(2):192–204.
32.GardenRS.Low-anglefixationinfracturesofthefemoral
neck.JBoneJointSurgBr.1961;43:647–63.
33.LevyRN,CapozziJD,MontMA.Intertrochanterichip
fractures.In:BrownerD,JupiterJ,LevineA,TaftonP,editors.
Skeletaltrauma:fractures,dislocations,ligamentousinjuries.
Philadelphia:Saunders;1992.p.1442–84.
34.WatsonJT,MoedBR,CramerKE,KargesDE.Comparisonof
thecompressionhipscrewwiththeMedoffslidingplatefor
intertrochantericfractures.ClinOrthopRelatRes.
1998;(348):79–86.
35.ChirodianN,ArchB,ParkerMJ.Slidinghipscrewfixationof
trochanterichipfractures:outcomeof1024procedures.
Injury.2005;36(6):793–800.
36.LarssonS,FribergS,HanssonLI.Trochantericfractures.
Influenceofreductionandimplantpositiononimpaction
andcomplications.ClinOrthopRelatRes.1990;(259):
130–9.
37.LindskogDM,BaumgaertnerMR.Unstableintertrochanteric
hipfracturesintheelderly.JAmAcadOrthopSurg.
2004;12(3):179–90.
38.HaidukewychGJ.Intertrochantericfractures:tentipsto
improveresults.JBoneJointSurgAm.2009;91(3):
712–9.
39.IsaacB,VettivelS,PrasadR,JeyaseelanL,ChandiG.Prediction
offemoralneck-shaftanglefromthelengthofthefemoral
neck.ClinAnat.1997;10(5):318–23.
40.ReikerasO,HoisethA,ReigstadA,FonstelienE.Femoralneck
angles:aspecimenstudywithspecialregardtobilateral
differences.ActaOrthopScand.1982;53(5):775–9.
41.ParkerMJ.Valgusreductionoftrochantericfractures.Injury.
1993;24(5):313–6.
42.KayRM,JakiKA,SkaggsDL.Theeffectoffemoralrotationon
theprojectedfemoralneck-shaftangle.JPaediatrOrthop.
2000;20(6):736–9.
43.BonamoJJ,AccettolaAB.Treatmentofintertrochanteric
fractureswithaslidingnail-plate.JTrauma.1982;22(3):205–15.
44.LimaALP,AzevedoFilhoAJ,AmaralNP,FranklinCE,Giordano
V.Tratamentodasfraturasintertrocanterianascomplacae