R e v is ta d a S o c ie d a d e B ra s ile ir a d e M e d ic in a T ro p ic a l 2 2 ( 1 ) : 1 3 -18 , j a n - m a r , 1 9 8 9
FAM ILY O CCURRENCE OF SCHISTOSOM AL HEPATO SPLENOM EGALY
A N D M A TER N A L E FFE C T
Jo sé T avares-N eto and Aluizio Prata
In th is p a p e r w e p r e s e n t a s tu d y o f m e m b e rs o f 2 6 5 n u c le a r fa m ilie s , a g e d s i x o r m ore. T h is s tu d y is b a s e d o f f a m i l y h er ed og ra m s, a n d ta k e s in to a c c o u n t th e c lin ic a l
fo r m o f s c h is to s o m ia s is o b s e r v e d before tr e a tm e n t w ith ox a m n iq u in e . T h e p r o b a b il ity o f occu rren c e o f tw o o r m o re c a s e s o fh e p a to s p le n o m e g a ly is low , n o tw ith s ta n d in g th e f a c t
th a t it w a s o b s e r v e d in 3 8 fa m ilie s . E v e n le ss f r e q u e n t is th e occu rren ce o f th re e o r m o re c a s e s o b s e rv e d in 1 7 f a m i li e s ( P —0 .0 0 2 ). T he co n c e n tr a tio n o f th e h e p a to sp le n ic fo r m w as h ig h e r a m o n g s ib lin g s th a n i t w a s a m o n g m o th e rs a n d ch ildren , o r f a th e r s a n d ch ildren . I t w a s f o u n d to b e n o t s ig n ific a n t betw e en h u s b a n d (f a th e r) a n d w ife (m oth e r). T h ese o b s e r v a tio n s rein fo rce th e e v id e n c e f o r th e p r e s e n c e o f a g e n e tic c o m p o n e n t in
s u s c e p tib ility to th e h e p a to s p le n ic f o r m o f th e d ise a s e . In c a s e s in w h ic h th e m o th e r w a s h e p a to sp le n ic th ere w a s a h ig h e r in c id en ce o f h e p a to s p le n ic ch ildr en ; th e r e la tiv e r is k w a s a le a s t f i v e tim e s h ig h er th an in th o se in w h ich th e f a t h e r w a s th e a ffec te d m e m b e r
(th e m a te r n a l effect). I n c a s e s w h ere b oth m e m b e rs w ere a ff e c te d b y th e h e p a to in te s tin a l
fo r m , th e r is k to th e f i l i a l g e n e r a tio n w a s s im ila r to th a t o f the p o p u la tio n in ge n e ra l. Thus, in th e p r o c e s s to w a r d s s e v e re f o r m s o f s c h is to s o m ia s is m a n s on i, p r e a n d p o s t n a ta l f a c to r s m ig h t b e in vo lv e d.
Key-words: Schistosom iasis. Fam ily occurrence. Maternal effect
The occurrence o f two or more cases o f schisto somal hepatosplenomegaly in the same nuclear family was first observed in 1958 by K lõetzel13 in the State o f Pernambuco. In a rural area o f the State o f Minas Gerais, Conceição & Coura8, using a more systematic methodology, verified that the number o f families, having two or more members affected by the hepatosplenic (H S) form was much higher than that expècted. Such an association was not pointed out by Wahab26 in Egypt.
To expand these studies, we decided to evaluate the familial occurrence o f schistosomal hepatosple-nomegaly, in a larger group o f patients. W e report an investigation o f nuclear families, based on data ob tained from heredograms and clinical examinations.
M A T E R IA L A N D M E T H O D S
The study was carried out in a hyperendemic area o f schistosom iasis mansoni in the city o f Catolân-diâ, (12 ° Latitude, 4 4 ° 5 0 ’ Longitude, W . Gr.), in the State o f Bahia, Brazil. In this region there is no malaria
Faculdade de Medicina do Triângulo Mineiro - Uberaba- M G and Núcleo de Medicina Tropical e Nutrição - Univer sidade de Brasília.
Financial support from C N Pq and the Ministry of Health. Address: Faculdade de Medicina do Triângulo Mineiro - Praça Thomaz Ulhoa, 706 — 38025 — Uberaba-MG, Brasil. Recebido para publicação em 3/12/88.
or kalaazar and the population has been under study since 1976 with regular clinical examinations, quanti tative parasitological tests and periodic treatment24. In one stool examination (K ato-K atz) 70% o f the population w as showed to have eggs o f S c h is to s o m a m a n so n i.
In 1986 all households in the area under study were visited and submitted to clinical examination. A t that time a heredogram was made in the presence o f the mother, taking into consideration the order of birth, including that o f the deceased, stillbirths, and abor tions.
A ll possible information about ancestors and descendents, occurrence o f consanguinity, as well as information about the existence o f other illnesses in the family were considered. In the few cases where the mother was abseiit (either by death or change o f residerice) we interviewed the father and, in his absence, we interviewed the oldest child. A ll given information was checked in a subsequent visit.
T a v a r e s - N e to J , P ra ta A . F a m i l y o c c u rren c e o f s c h is to s o m a l h e p a to sp le n o m e g a ly a n d m a te r n a l e ffe c t R e v is ta d a S o c ie d a d e B ra s ile ir a d e M e d ic in a T ro p ic a l 22: 1 3 -1 8 , j a n - m a r , 1 98 9.
For the statistical analysis we used the program system “ Statistical Package for the Social Science” , or special programs in A L G O L language. In the study o f familial recurrence we used the binomial distribution p (x) = (xn) px.qx-n (Siegel, 1975).
R E SU L T S
Tw o hundred and seventy one nuclear families (father, mother and children) lived in the 233 homes under study. There was no information on at least 25% o f the members o f 6 families. In the remaining 265
families (97.8% ) there were 1 386 members who were 6 years old or older. Members under six were excluded because the HS form has never been report ed before age 6 14 19, Chit o f 26 families, the father (n = 1 6 ), the mother (n = 9 ), both ( n = l ) , or children (n = 1 5 ) had not been physically examined before treatment with oxamniquine.
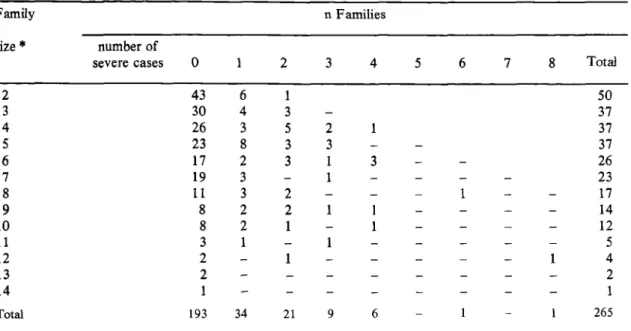
In relation to the H S form o f the schistosomiasis mansoni, no cases were recorded in 193 families (72.8% ), in 34 families one case was recorded (12.8% ), and in 38 families (14.4% ), there were two or more cases o f hepatosplenomegaly. Am ong those, 8 families presented four or more cases (table 1).
Table 1 - Distribution o f hepatosplenic schistosomotic individuals in nuclear families o f different sizes.
Family
size *
n Families
number o f
severe cases 0 1 2 3 4 5 6 7 8 Total
2 43 6 1 50
3 30 4 3 37
4 26 3 5 2 1 37
5 23 8 3 3 - - 37
6 17 2 3 1 3 _ - 26
7 19 3 - 1 - - - 23
8 11 3 2 - - 1 - - 17
9 8 2 2 1 1 - - - - 14
10 8 2 1 - 1 - - - - 12
11 3 1 - 1 - - - 5
12 2 - 1 - - - 1 4
13 2 - - - 2
14 1 - - - - - - 1
Total 193 34 21 9 6 - 1 - 1 265
(*) Number o f family members (father, mother and children, 5 years old and older).
Prior to treatment, the frequency o f the schis tosomotic hepatosplenomegaly (5 6 /9 2 2 ) in individuals residing in the area, and aged 6 or more, was 6% (q = 0 .0 6 ). Because the same individual might be a parent in one family and a child in another, to avoid counting twice the same person, for the calculation o f this frequency we took less than the total o f family members (n = 1,386).
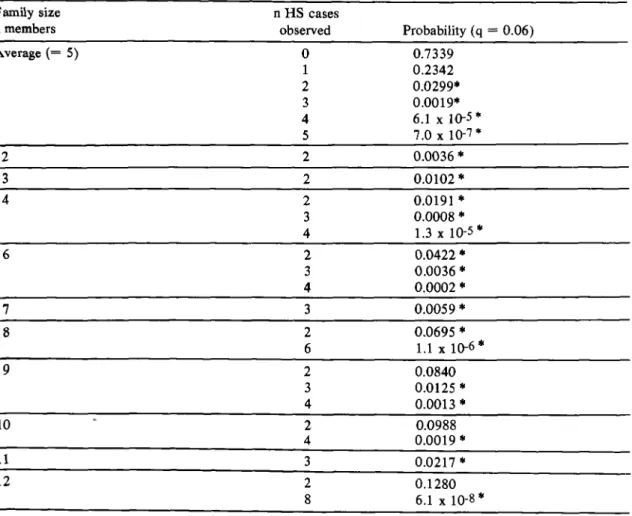
The average family had 5.2 members (1 ,3 8 6 /2 6 5 ). Thus, the probability (P) from zero to 5 cases [P(x) = (xn) .px .qn‘x] is displayed on table 2 along with other family sizes, according to the number o f cases ( > 2) o f hepatosplenomegaly observed on Table 1. The probability o f occurrence o f two cases o f H S in a single family would be statistically unlikely, and even more so the occurrence o f three cases (P = 0 .0 0 1 9) for families with five members. However,
even in a family with 12 members the observation o f eight cases had a P = 6,1 x 10-8. The occurrence o f three cases in these families would have P < 0.05.
Table 3 showns that the nuclear families o f different sizes had respective numbers o f observed families “n” with tw o or more cases H S that cor related to the expected number (rig); in this situat ion, tv, was 38. Considering the fact that the expected number o f families with two or more cases was equal to 11, the difference was highly significant ( x ^ = 69.14
p < 0.00001).
T a v a r e s- N e to J, P r a ta A . F a m i l y o c c u rre n ce o f s c h is to s o m a l h e p a to sp le n o m e g a ly a n d m a te r n a l e ffe c t R e v is ta d a S o c ie d a d e B r a s ile ir a d e M e d ic in a T r o p ic a l 2 2 : 1 3 -1 8 , ja n - m a r , 1 98 9.
Table 2 - Expected probability o f hepatosplenic (H S ) cases, according to the average size of the nuclear family, and the number observed in the different family sizes.
Fam ily size n H S cases
n members observed Probability (q = 0.06)
Average ( = 5 ) 0 0.7339
1 0 .2 3 4 2
2 0.0299*
3 0.0019*
4 6.1 x 10“5 * 5 7.0 x 10-7*
2 2 0 .0 0 3 6 *
3 2 0 .0 1 0 2 *
4 2 0.0191 *
3 0.0 0 0 8 * 4 1.3 x 10-5*
6 2 0 .0 4 2 2 *
3 0 .0 0 3 6 * 4 0 .0 0 0 2 *
7 3 0.0 0 5 9 *
8 2 0.0695 *
6 1.1 x 10-6 *
9 2 0.0 8 4 0
3 0.0125 *
4 0.0013 *
10 2 0.0988
4 0 .0 0 1 9 *
11 3 0.0217 *
12 2 0.1280
8 6.1 x 10-8 *
(*) Significant: p < 0.05
Table 3 - Expected(e) and observed(0) number o f families and filial generation o f different sizes, for q = 0 .06 with two or more cases o f hepatosplenic (H S) form.
____________________Fam ilies_______________ ___________ Filial generation________________ C ases H S 2: 2
Size n 0 ea Size n o ea
2 50 1 0.2 2 36 4 0.1
3 37 3 0.4 3 41 4 0.4
4 37 8 0.7 4 22 5 0.4
5 37 6 1.2 5 24 2 0.8
6 26 7 1.2 6 21 5 1.0
7 23 1 1.4 7 13 3 0.8
8 17 3 1.4 8 14 3 1.1
9 14 4 1.4 9 + 11 3 1.1
10 12 2 1.4
11 + 12 3 1.7
Total 265 38 11.0 182 29 5.7
X f = 6 9 .1 4 p < 0.00001 X \ = 9 8 .3 2 p < 0.00001
T a v a r e s - N e to J , P r a ta A . F a m i l y o c cu rre n c e o f s c h is to s o m a l h e p a to sp le n o m e g a ly a n d m a te r n a l e ffe c t R e v i s t a d a S o c ie d a d e B ra s ile ir a d e M e d ic in a T r o p ic a l 2 2 : 1 3 -1 8 , ja n - m a r , 1 9 89 .
cases in 1 group and 8 cases in one group. The probability calculation q = 0 .0 6 , o f individuals affected for different sizes o f filial groups, presented results similar to those o f nuclear families. The expected number o f filial groups with two or more cases H S referred to in table 3 was significantly inferior to that observed (x? = 9 8 .3 2 p < 0.00001). Familial occurrence was also analysed pairing the clinical forms H I or H S - father/mother; father/ child (father/childi); father/child2 ; father/childn) mother/child; (mother/child^...); and sibling/sibling (siblmgj and sibling2; siblingj/siblingj; sibling2/ sibling3 ...).
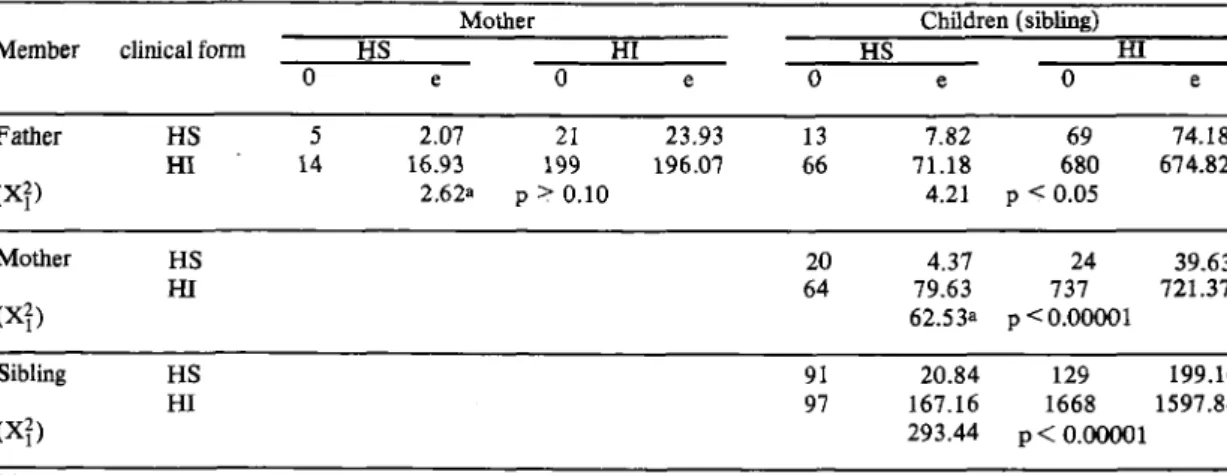
In Table 4 the results o f these pairings are displayed observing the concentration o f schisto-somotic hepatosplenomegaly cases between father and children, mother and children, and siblings (siblings and siblings) in a significantly statistical form. A
situation o f both presenting the clinical form H S was accountable for at least 80% o f the total chi square. Nevertheless between husband and wife (or father and mother) the distribution was random (p >; 0 .10).
In Table 4 one can see that the occurrence o f the H S form was significantly higher among siblings, reaching ahighchi square ( x | = 29 3 .4 4 ). Between mother and children ( x | = 62 .5 3 ), the statistical significance was higher than between father and children (x f = 4.21). On account o f this, the couples were divided in the following types as far the clinical form was concerned: “ A ” , both affected by the H I form; “B” , H S father and H I mother, “ C” HI, father and H S mother, and “D ” , both H S. On table 5, these types of couples were correlated with the children according to the clinical form o f the schistosomiasis. The distribution was not equal among the four types o f couples (x^ = 85.99 p < 0 .0 0001).
Table 4 - Correlation of clinical forms of schistosomiasis mansoni among members of the nuclear families.
Member clinical form
Mother Children (sibling)
HS HI HS m
0 e 0 e 0 e
0
eFather HS 5 2.07 21 23.93 13 7.82 69 74.18
H I 14 16.93 199 196.07 66 71.18 680 674.82
(X?) 2.62a p > 0.10 4.21 p < 0.05
Mother HS 20 4.37 24 39.63
H I 64 79.63 737 721.37
(X?) 62.53a p < 0.00001
Sibling HS 91 20.84 129 199.16
HI 97 167.16 1668 1597.84
(X?) 293.44 p < 0.00001
(a) Yates correction.
Table 5 - Distribution o f hepatosplenic (H S ) and hepatointestinal (H I) schistosom iasis mansoni in children, according with the ones found at the parental generations.
Couple H S
number o f children
HI H S
Father Mother no ne «o ne % RRa
“A ” HI HI 40 59.77 638 618.23 5.9 1.0
“ B” H S HI 10 6 .44 63 66.56 13.7 2.4
“ C ” HI HE 17 3.09 18 31.91 48.6 14.6
“D ” H S HE 3 0 .7 0 5 7.30 37.5 9.3
(a) Risk as related to the population (5 6 /9 2 2 ). X 3 = 85.99 p < 0.00001
In cases where one o f the parents or both had the H S form, there was a significantly, higher occurrence o f H S children. Between couples “ C ” and “D ” the frequency o f H S children was similar (x? = 0 .4 9 p >
T a v a r e s -N e to J , P r a ta A . F a m i l y o c c u rre n ce o f s c h is to s o m a l h e p a to sp le n o m e g a ly a n d m a te r n a l e ffe c t R e v is ta d a S o c ie d a d e B ra s ile ir a d e M e d ic in a T r o p ic a l 2 2 : 1 3 -1 8 , ja n - m a r , 1 9 89 .
observations have correlation with the relative risks of hepatosplenomegaly in children from each type of couple. W hile the risk to the children o f couples “ C” and “ D ” was o f 13.4, that o f couples “ B” was o f 2.4, and that o f couples “A ” was similar to the risk o f the population in general. Thus, the risk o f having HS children was higher when one o f the parents was HS. This risk is at least five times higher when the mother (as compared to the father) is affected by this serious form o f the disease.
D IS C U S S IO N
In Brazil the H S form of the schistosomiasis mansoni occurs with much higher frequency in whites than in blacks^ 20 24 25, The mestizo, children o f black and white parents, show an intermediary fre quency, which is significantly inferior them that ob served in white individuals24. However, in Brazil the whites have better social and economic standards, including a higher rate o f literacy16 22 24 This fact would lead us to expect an inverted observation. Find ings such as these corroborated the participation o f a genetic component in the susceptibility to the H S form o f schistosomiasis mansoni15.
The occurrence o f this severe form was present significantly in the filial generation. In average families, the occurrence o f two H S cases would be remote, and the occurrence o f three or more cases would be a very rare eventuality indeed. For example, in an average family o f five, with q = 0.0 6 , the probability o f having three or more severe cases would be 0.002. W hen q = 0 .19 the probability is below (5%). However, eight families presented four or more cases for q = 0.06; the probability would be 6 .1 x lO-5. If the average size o f the family were 10 and q = 0.1 4 , the probability o f having four cases would be inferior to 0 .0 4 (4% ). Nevertheless we observed 38 families with two or more cases; 17 families having three or more cases.
In infectious parasitic diseases o f low frequency ( < 1%) the probability o f contagion among members o f the same family is higher than that among unrelated members; extra familial infection foci have a higher probability o f influence when the frequency is higher ( > 1%). However, in the latter case, when the affected members are not evenly distributed within the families, we can assune the existence o f genetic factors exerting influences in susceptibility to the disease (Beiguelman 1 9 8 3 )1 as observed in our results and in those of K lõetzel13, and C onceição and Coura8.
Intrafamilial environmental factors are influen tial. However, if these alone were preponderant, or the only relevant ones, the distribution o f the H S forms would be uniform among families. The highly signi
ficant concentration o f H S cases between children of the same nuclear fam ily favors the hypothesis o f the contribution o f a genetic factor in the predisposition to the serious forms. This hypothesis is reinforced by the existence o f concentration among parents and chil dren, and by the fact that a concentration among the parents themselves was not observed.
A very interesting verification was that o f a higher concentration o f H S children, when the mother was the one affected by the same clinical form o f the disease. In Taquarandi-Bahia, Prata, Bina, Satumino and Tavares-N eto (umpublished data) have also observed this maternal effect. There is no reported research focusing on this maternal effect.
In man this effect, as in mammals in general, has been studied with emphasis on its quantitative characteristics1^.
The pre and post-natal influences would be the basis for the maternal effect, and they certainly would involve several factors. Camus e col3., for example, verified that children, not affected by S c h is to s o m a m a n s o n i,but whose mothers were infected, responded more significantly to the intradermic delayed test with adult worm antigen. This seems to be due to intra uterine sensibilisation to schistosomal antigens or through the milk3. Later on, Camus et al4, and Ohta et al1’?, noted that these immunological characteristics were related to the hepatosplenic form o f the disease. Perhaps, due to this, the H S mothers showed a higher incidence o f H S children. However, Sobral et al23., verified experimentally that m ice, bom o f infected females, showed a higher resistence to infection induced after weaning.
However factors involved in the susceptibility and in the resistence to schistosom al infection, and to the H S o f the disease, should be distinguished. For this purpose, when investigating the factors predis posing to infection and to H S disease, one must take into account items such as environmental and pre and post-natal factors, besides those an exclusive envi ronmental nature.
R E S U M O
A s f o r m a s c lín ic a s d a e s q u is to s s o m o s e m a n -sô n ic a , a n te rio re s a o tr a ta m e n to c o m o x a m n iq u in e ,
fo r a m e s tu d a d a s n o s m e m b r o s d e 2 6 5 f a m ília s , co m s e is a n o s ou m a is d e id a d e . A p r o b a b ilid a d e d a oc o rrê n cia d e d o is ou m a is c a s o s, n a m e sm a f a m ília , d a h e p a to s p le n o m e g a lia e s q u is to s s o m ó tic a ( H E ) é
T a v a r e s- N e to J , P ra ta A . F a m i l y o c c u rren c e o f s c h is to s o m a l h e p a to sp le n o m e g a ly a n d m a te r n a l e ffe c t R e v is ta d a S o c ie d a d e B r a s ile ir a d e M e d ic in a T r o p ic a l 2 2 : 1 3 -1 8 , j a n - m a r , 1 9 89 .
m ã e s e f i lh o s e p a i s e filh o s . N ã o s e n d o sig n ific a n te a co n c e n tr a ç ã o e n c o n tr a d a n o c a s a l en tre m a r id o e m u lh er. E s ta s o b s e r v a ç õ e s re for ça m a e v id ê n c ia d o
efe ito d o c o m p o n e n te g e n é tic o d a ' s u s c e p tib ilid a d e p a r a a f o r m a H E . T a m b é m , q u a n d o a m ã e era
h e p a to sp lê n ic a (H E ) a p r e v a lê n c ia d e s ta f o r m a n o s f i lh o s f o i m aior ; o risc o re la tiv o f o i cin c o v e z e s
s u p e r io r (e fe ito m a te rn o ), c o m p a r a d o a o e n c o n tr a d o
q u a n d o e ra o p a i h e p a to sp lê n ic o . Q u a n d o a m b o s o s
g e n ito r e s e ra m h e p a to in te s tin a l o s r isc o s r e la tiv o s d a f o r m a H E , n os filh o s , f o i se m e lh a n te a o d a p o p u la ç ão g e r a l. A ss im , p r o v a v e lm e n te f a to r e s p r é e p ó s
-n a ta is ta m b é m e s ta r ã o e -n v o lv id o s -n a p r e d is p o s iç ã o d a f o r m a h e p a to sp lê n ic a .
Palavras-chaves: Esquistossomose. Recorrên cia familial. Efeito materno.
REFERENCES
1. Beiguelmann 8 . Leprosy and genetics: a review. Revista Brasileira Genética 6: 109-172, 1983.
2. Bina JC, Prata A. Regressão da hepatosplenomegalia pelo tratamento especifico da esquistossomose. Revista da Sociedade Brasileira de M edicina Tropical 16:213-218,1983.
3. Camus D, Carlier Y, Bina JC, Borojevic R, Prata A, Capron A. Sensibilization to Schistosoma mansoni an tigen in a infected children bom to infected mothers.
Journal o f Infectious D iseases 134: 405-408, 1976. 4. Camus D, Carlier Y, Capron M, Bina JC, Figueiredo
JFN, Prata AR, Capron A. Immunological studies in human schistosomosis III. Immunoglobulin levels, antibo dies and delayed hipersensitivity. American Journal o f Tropical M edicine an d Hygiene 26: 482-490, 1977. 5. Cardoso W. A esquistossomose mansônica no negro.
M edicina, Cirurgia e Farm ácia 202/203:89-95,1953. 6. Cheever AW. A review. Schistosoma japonicum: The pathology of experimental infection. Experimental Parasitology 59: 1-11, 1985.
7. Cheever AW, Dunn MA, Dean DA, Duvall R. Diffe rences in hepatic fibrosis in ICR, C3H, and C57 8L/6 mice infected 3 with Schistosoma mansoni. American Journal o f Tropical M edicine and Hygiene 32:
1364-1369, 1983.
8. Conceição MJ, Coura JR. Ocorrência familiar de esple-nomegalia esquistossomática em uma área rural de Minas Gerais. Revista da Sociedade Brasileira de M edicina Tropical 13: 17-20, 1980.
9. Dietze R, Prata A. Rate of reversion of hepatosplenic schistosomiasis after specific therapy. R evista da Socie dade Brasileira de M edicina Tropical 19:69-73,1986. 10. Falconer DS. Introdución a la genética quantitativa.
Ed. Co. Continental, 1971.
11. Fanning MM, Kazura JW. Genetic-linked variation in susceptibility of mice to schistosomiasis mansoni. P ara site Im m un ology6: 95-103, 1984.
12. Fanning MM, Peters PA, Davis RS, Kazura JW
Mahmoud AAF. Immunopathology of murine infection with Schistosoma mansoni: Relationship of genetic background to hepatosplenic disease and modulation. Journal o f Infectious D ise ase s 144: 148-153,1981. 13. Klõetzel K. A síndrome hepatosplênica na esquistos
somose mansônica. Considerações sobre a incidência familial. R evista B rasileira de M edicin a 15: 263-265, 1958.
14. Klõetzel K. Splenomegaly in schistosomiasis mansoni. A m erican Journal o f T ropical M edicin e a n d H ygiene
11: 472-476, 1962.
15. Mahomoud AAF. Genetic of schistosomiasis. In: Michal F (Ed.) M o d e m gen etic concepts a n d techniques in th e stu d y o f parasites. Co. Ag. Basel, p. 302-303,
1981.
16. Oliveira L E G , Porcaro RM , Araújo TCN. O lu g a r d o
n e gro n a f o r ç a d e tra b a lh o . Instituto Brasileiro de Geografia e Estatística (IBGE), Rio de Janeiro, 88p., 1981.
17. Ohta N , Nishimura YK, Iuchi M, Sasazuki T. Immuno- genetic analysis of patients with post-schistosomal liver
cirrhosis in man. C lin ic a l E x p e r i m e n t a l I m m u n o l o g y
49: 493-499, 1982.
18. Prata A. Como caracterizar a forma hepatosplênica da esquistossomose. In: Prata A, Aboim E. (ed.), I I S im p ó sio sobre E squ istossom ose, Salvador, Bahia, p.
179-184, 1970.
19. Prata A, Bina JC. Development of the hepatosplenic
form os schistosomiasis. G a ze ta M é d ic a d a B a h i a . 68:
49-60, 1968.
20. Prata A. Schroeder S.A comparison of whites and
negroes infected with S c h is to s o m a m a n s o n i in hyper
endemic areas. G azeta M éd ica da B ah ia 67: 93-98, 1967.
21. Siegel S. E sta tístic a não-param étrica, McGraw-Hill, p. 350, 1975.
22. Silva NV. Cor e o processo de realização sócio-econô-mica. R ev ista de C iências S o ciais24: 391-409, 1981. 23. Sobral ACL, Lenzi JA, Lenzi HL. Influência de fatores congênitos e do aleitamento na evolução da infecção esquistossomótica. R e vista da S ocieda de B rasileira de M edicin a T ropical 10 (supl.): 64,1987.
24. Tavares-Neto J. Recorrência familial e composição racial na esquistossomose mansônica. Tese de Mestrado, Universidade de Brasília, 256p., 1987.
25. Tavares-Neto J. A raça branca e a forma hepatosplênica da esquistossomose. R e vista d e S aú d e P ú blica21: 342-347,1987.