rev bras ortop.2017;52(5):612–615
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Giant
palmar
lipoma
–
an
unusual
cause
of
carpal
tunnel
syndrome
夽
Gaizka
Ribeiro
∗,
Marta
Salgueiro,
Miguel
Andrade,
Victor
Santos
Fernandes
HospitaldeSantaMaria(CHLN),Servic¸odeCirurgiaPlástica,Lisboa,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14July2016
Accepted16August2016
Availableonline14August2017
Keywords:
Lipoma
Carpaltunnelsyndrome
Hand
Mediannerve
a
b
s
t
r
a
c
t
Lipomaisaquitecommontypeofsoft-tissuetumor,butitisrarelyfoundinthehand.Hand
lipomasaregenerallyasymptomatic;however,whentheybecometoolargeorwhenthey
arepresentinsomespecificlocation,theycancausesymptomsduetocompressionofthe
mediannerve.Thesetumorsmustbecorrectlycharacterizedpreoperativelywithimaging
examsandthepropermanagementisthecompleteremovalofthetumorandreleaseofthe
mediannerve.Theauthorspresentthecaseofafemalepatientwithcarpaltunnelsyndrome
duetocompressionofthemediannervebyagiantpalmarlipoma,successfullytreatedwith
tumorexcisionandnerverelease.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Lipoma
palmar
gigante
–
Uma
causa
pouco
usual
de
síndrome
do
túnel
cárpico
Palavras-chave:
Lipoma
Síndromedotúnelcarpal
Mão
Nervomediano
r
e
s
u
m
o
Olipoma é um tumor frequente dos tecidos moles, mas a sua localizac¸ão na mão é
rara.Oslipomas damão geralmentesãoassintomáticos; contudo,quandoapresentam
umgrandecrescimentoouemdeterminadas localizac¸ões,podemcausarsintomas
dev-idoàcompressãodonervomediano.Essestumoresdevemserdevidamentecaracterizados
pré-operatoriamentecomumexamedeimagemeseucorretotratamentobaseia-sena
suaexcisãocompletaeliberac¸ãodonervomediano.Apresentamosocasoclínicodeuma
pacientecomodiagnósticodesíndromedotúnelcarpalresultantedecompressãodonervo
medianoporumlipomapalmargigante,tratadacomsucessocomlipectomiae
descom-pressãonervosa.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora
Ltda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedatHospitaldeSantaMaria(CHLN),Servic¸odeCirurgiaPlástica,Lisbon,Portugal.
∗ Correspondingauthor.
E-mail:[email protected](G.Ribeiro).
http://dx.doi.org/10.1016/j.rboe.2017.08.001
2255-4971/©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
rev bras ortop.2017;52(5):612–615
613
Introduction
Lipomasareveryfrequentbenignsofttissuetumors,1–8 but
theirincidence inthe handis rare.1–6 Lipomasare
consid-eredgianttumorswhentheyare5cm2,3ormoreindiameter,
and they generally behave as asymptomatic tumefactions,
ofslowandprogressivegrowth5,8;however,sometimesthey
canleadtosymptomatologyduetocompressionofadjacent
structures.1–3,5,8,9 Peripheric nerve compression bylipomas
is very uncommon. Few cases of carpal tunnel syndrome
resultingfrom mediannerve compression byalipoma are
describedintheliterature.4,6Theanatomicparticularitiesof
thehandrequirespecialcareinthediagnosticandtherapeutic
approachtothesetumors.3Inthisarticlewedescribea
clini-calcaseofaseventy-year-oldfemalepatientwithadiagnosis
ofgiantpalmarlipomathatleadstocarpaltunnelsyndrome,
successfullytreatedwithalipectomyandreleaseofthe
ante-riorannularligamentofthecarpus.
Clinical
case
Aseventy-year-oldfemale,leucodermicpatient,wasreferred
toaplasticsurgeryconsultationbytheattendingphysician
dueto swelling on the palmar side ofthe left hand
(non-dominanthand),withprogressivegrowthoverthelastyear,
andcomplaintsofparesthesiaandpaininthefirstthree
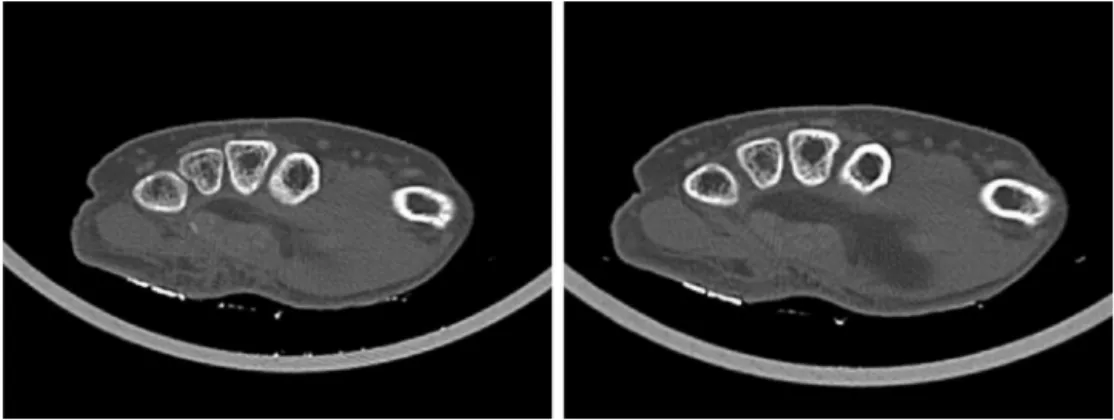
fin-gersofthelefthand.Thepatientunderwentacomputedaxial
tomographyofthehandandwristrequiredbyherphysician,
whichrevealedaformationofadiposedensitywithsomefine
internalseptations,withwell-definedcontours,
intramuscu-larlocationwithextensiontothedeep spacesofthehand
andwithabout6.5cmofcross-sectionalaxisand6.5of
longi-tudinalaxis,findingssuggestingthediagnosisofgiantpalmar
lipoma(Fig.1)
Onexamination,thepatienthadapalpable,movablemass
atthelevelofthethenareminence,ofsoftandpainless
consis-tency(Fig.2).Thepercussionofthemasstriggeredcomplaints
ofparesthesiaofthefirstthreefingersofthelefthand
(posi-tiveTinel’ssign).Thepatienthadnomotorcomplaintsofthe
hand,withpreservationofstrengthanddigitalpincer
func-tion.Axillaryadenopathieswerenotpalpable.
Anelectromyographyofthewristwasdone,which
identi-fiedaspectsconsistentwithmarkedleftmediannervelesion.
Fig.2–Swellingofthethenareminence.
Withthediagnosisobtained,surgicaltreatmentwas
pro-posed to the patient. In a supine position, under brachial
plexus anesthesia and controlled ischemia of the upper
limbwithapneumatictourniquet,tumorexcisionwas
per-formed. Through apalmar incision, thepalmar fascia was
opened and the tumorwas dissected and excised (Fig. 3).
Themediannerveanditsbranchesweredulyidentifiedand
preserved(Fig.4).Theanteriorannularcarpalligamentwas
sectioned.Afterrevisionofthehemostasis,theincisionwas
closedinasingleplanewithnon-absorbablesuturesunder
passive drainage. The procedure lasted for about 2h and
therewerenocomplications.Thepatientwasdischargedon
the same dayand wasfollowedup atanoutpatientclinic.
Theanatomopathologicalresultconfirmedthe diagnosisof
lipoma.
Afterfive months,there wasreversionofcomplaintsof
paresthesiaand painofthe firstthree fingersofthehand.
Duringthisperiod,noclinicalsignsoftumorrecurrencewere
identified,andtherewasgoodwoundhealing(Fig.5).
Discussion
Lipomas are the most frequent tumors in the human
body1–8;however,theirlocationinthehandisrare,1–6which
is a challenge in terms of a diagnostic and therapeutic
approach.3
614
rev bras ortop.2017;52(5):612–615Fig.3–Intraoperativephotoofpalmarlipoma.
Fig.4–Intraoperativephotowherethemediannerveand
branchescanbeseen.
Fig.5–Postoperativephotoafterfivemonths.
Handlipomahasahigherincidenceinindividualsbetween
50 and 60 years and is generally asymptomatic, revealing
itselfasamobileandpainless massofprogressivegrowth.
Sometimes, when it becomes massive or in certain
loca-tions, it can cause symptoms resulting from nervous
compression.1–4,6,8,9Intramuscularorsubfascialgiantlipomas
ofthehand(>5cmofdiameter)canbethecauseofcarpal
tun-nelsyndrome;therearefewcasesdescribedintheliterature.6
Whencarpaltunnelsyndromesecondarytogiantlipoma
is suspected, hand imaging (ideally a computed axial
tomography or magnetic resonance imaging) is essential,
allowingabettercharacterizationofthesizeandlocationof
thetumor,aswellasitsrelationwiththeneighboringvascular
andnervestructures.1–4,6,8,9Theseexamsarealsoimportant
toestablishthedifferentialdiagnosiswithmalignanttumors,
becausethesehandtumorsofmorethan5cmofdiameterare
highlysuggestiveofmalignancy.2,3,6,7Awristelectromyogram
isequallyindispensablefordocumentingthenervelesion.3,6
Thetreatmentofthesepatientsinvolvestumorexcision
andmediannervereleaseinthecarpaltunnel.Amonoblock
excision ofthelipomashouldbeideallydone, withcareful
dissectionthatallowstheidentificationandpreservationofall
vascularandnervestructuresadjacenttothetumor,toreduce
theriskofiatrogenicinjury.1,3,6,8,9
Although hand lipomas are rare, they should not be
neglectedasapossiblecaseofmediannervecompressionin
thecarpaltunnel.Itscorrecttreatmentreliesontheadequate
tumortopographiccharacterization,onasurgicalapproach
that preserves the anatomic structuresinvolved, and on a
completeexcision,reducingtheriskofrecurrence.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MohanL,SemoesJ.Thenarintramuscularlipoma:anunusual
case.InternetJSurg.2007;17:1–3.Availablefrom:
http://print.ispub.com/api/0/ispub-article/9785.
2.YildiranG,AkdagO,KarameseM,SelimogluM,TosunZ.Giant lipomasofthehand.HandMicrosurg.2015;4(1):8–11.
3.FazilleauF,WilliamsT,RichouJ,SauleauV,NenD.Median
nervecompressionincarpaltunnelcausedbyagiantlipoma.
CaseRepOrthop.2014;2014:1–5.Availablefrom:
http://www.hindawi.com/journals/crior/2014/654934/. 4.AzwaN,ShalimarA,JamariS.Apalmarlipomawithmedian
andulnarnervecompressivesymptoms.MalaysOrthopJ. 2007;1:33–5.
rev bras ortop.2017;52(5):612–615
615
6.SbaiMA,BenzartiS,MsekH,BoussenM,KhorbiA.Carpal tunnelsyndromecausedbylipoma:acasereport.PanAfrMed J.2015;22:51.
7.MoralesC,LópezJ,GargolloC,JiménezY.Handlipoma, surgicalenclinicallynaunderstimatedtumor.CirPlást Iberolatinoam.2011;37:349–53.
8.NadarMM,BartoliCR,KasdanML.Lipomasofthehand:a reviewand13patientcaseseries.Eplasty.2010;10:e66.