w w w . r b o . o r g . b r
Original
article
Functional
result
relating
to
the
positioning
of
the
graft
in
anterior
cruciate
ligament
reconstruction
夽
Otávio
de
Melo
Silva
Júnior,
Bruno
do
Nascimento
Ohashi,
Murilo
Oliveira
de
Almeida
∗,
Murilo
Reis
Gonc¸alves
SobradinhoRegionalHospital,Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1November2013 Accepted7November2013 Availableonline14February2015
Keywords: Knee/surgery
Anteriorcruciateligament Treatmentresult
Traumaamongathletes
a
b
s
t
r
a
c
t
Objective:Toascertainthecoronalanglesforthefemoralandtibialtunnelsthatprovide thebestpostoperativeresultfromanteriorcruciateligament(ACL)reconstructionsurgery, throughassessingthevariablesoftheIKDCandLysholm–Tegnerquestionnairesandthe hoptest.
Methods:SixteenpatientswithasingleunilateralACLinjurywhounderwentthissurgery between24and36monthsearlierwereevaluated.Theyweredividedintofourgroupsin whichthetibialandfemoraltunnelanglesweregreaterthanorlessthan65◦inthecoronal
plane.
Results:Theresultsdemonstratedthatamoreverticalangleforthetibialtunnel(72◦)anda
morehorizontalangleforthefemoraltunnel(60◦
),withvalgusalignmentof12◦
correlated withthebestvaluesforthevariablesstudied.Thismayindicatethatthelong-termresults fromthissurgeryareexcellent.
Conclusion: Amorehorizontalfemoralangleandamoreverticaltibialangleproducedbetter assessmentsintheteststhatwereappliedandinthefunctionalresultsevaluated.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Resultado
funcional
relacionado
ao
posicionamento
do
enxerto
na
reconstruc¸ão
do
ligamento
cruzado
anterior
Palavras-chave: Joelho/cirurgia
Ligamentocruzadoanterior Resultadodetratamento Traumatismosematletas
r
e
s
u
m
o
Objetivo:Averiguarqualaangulac¸ãocoronaldostúneisfemoraletibialqueproporciona omelhorresultadono pós-operatóriode cirurgiade reconstruc¸ãodoLCA.Asvariáveis avaliadasforamosquestionáriosIKDCeLysholm-TegnereoHop-Test.
Métodos:Foramanalisados16pacientescompós-operatórioentre24e36meses,comlesão isoladaunilateraldoLCA.Foramdivididosemquatrogrupos,nosquaisosângulosdostúneis tibialefemoralforammenoresoumaioresdoque65◦noplanocoronal.
夽
WorkdoneattheOrthopedicsandTraumatologyService,SobradinhoRegionalHospital,Brasília,FederalDistrict,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.O.deAlmeida). http://dx.doi.org/10.1016/j.rboe.2015.01.008
Resultados: Aangulac¸ãodotúneltibialmaisverticalizada(72◦
)edotúnelfemoralmais horizontalizada(60◦)comoalinhamentoemvalgode12◦relacionou-secomosmelhores
valoresparaasvariáveisestudadas,oquepodeindicarumresultadoótimoparaacirurgia emlongoprazo.
Conclusão:Aangulac¸ãofemoralmaishorizontalizadaeaangulac¸ãotibialmaisverticalizada têmmelhoresavaliac¸õesnostestesaplicadosenosresultadosfuncionaisavaliados.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Injuriesortearstotheanteriorcruciateligament(ACL)in ath-letesorphysicallyactiveindividualsare seenvery oftenin orthopedicpractice.Epidemiologicalstudieshaveshowedthat theincidenceisapproximately80,000injuriesperyear.1
ThefirstreportsonACLinjuriesappearedintheliterature inthe nineteenthcentury.2 Recordsof surgical
reconstruc-tionfirstappearedatthebeginningofthetwentiethcentury.3
Overthelast30years,manysurgicaltechniqueshavebeen describedforreconstructingthisligament,usingseveral struc-turesasagraft source.Along pathwas followeduntilthe techniquedescribed byCampbell4 in1939,which usedthe
patellarligament,wasreturnedto.Alsointhatyear,Macey5
describedthefirsttechniqueusingtheflexortendonsofthe semitendinosusandgracilis(ST-G).
Althoughthegreatadvancesinsurgicaltechniqueshave reducedthetimetakenforpatientsundergoingACL recon-structionto returnto theiractivities,6 wedidnot findany
studiesintheliteraturecorrelatingtheanglesofthetunnels withthepostoperativeresults.
Thereisno consensusregardingthe various techniques forACLreconstructionthathavebeendescribed,inrelation tocomparisonsbetweenthepostoperativeresults.There is thereforeaneedforbetterexaminationofthepossiblevariable thatmightcorrelatewithabetterfinalresult.
Currently, tibial tunnels are constructed using prefabri-catedguidesthatareadjustableaccordingtotheanglethat isdesired.
Theobjectiveofthis studywas toascertainthe coronal angleofthe femoraland tibialtunnelsthat wouldprovide thebestpostoperativeresultfromACLreconstructionsurgery, usingthefollowingassessmentcriteria:patient’scomplaints, satisfaction with the result, Lysholm–Tegner questionnaire (Annex1),IKDCquestionnaire(Annex2),clinicalexamination andhoppingononefoot.
Material
The knees of 16 patients were evaluated (Table 1). These patientswere seenatthe kneesurgeryoutpatientclinicof theSobradinhoRegionalHospital,FederalDistrict,Brazil,and had undergoneACL reconstructionperformedbythe same surgeon,whowasaspecialistinkneesurgeon.
Thedemographiccharacteristics(gender,age bodymass index(BMI)anddominantleg)arelistedinTable1.
Table1–Characteristicsofthesample.
n(%)
Gender
Male 13(83.25)
Female 3(17.75)
Age(years)
Upto20 1(6.25)
21–30 9(56.25)
31–40 4(25)
Over40 2(12.5)
Mean=29.7
BMI(kg/m2)
18.5–24.9(Normal) 10(62.5)
25–29.9(Overweight) 6(37.5)
Mean=24.96
Dominantleg
Right 11(68.75)
Left 3(18.75)
Ambidextrous 2(12.5)
The inclusion criteria were as follows: a postoperative period ofbetween24 and 48months; ACL injuryalone, as confirmedbymeansofmagneticresonance imagingbefore theoperation;physiotherapyappliedaftertheoperation;and having been released from rehabilitation (with or without returningtothesameactivitylevelasbeforetheinjury).
The exclusion criteria comprised presenceof any asso-ciated injuriesto the ligaments,menisci or joint cartilage, revision surgery, inflammatory signs, neuromuscular dis-orders, infection, arthrofibrosis, lower-limb fractures, or advancedosteoarthrosisinthefemoropatellarortibiofemoral jointswithevidentdisplacementofthejointaxis.
Table2detailsthefactorscorrelatedwiththetypeofsport practiced, the groundand the conditions under which the injuryandtherehabilitationtookplace.
All the patients underwent the same standard surgical technique, consisting of grafting a single band from the semitendinosusandgracilistendons(ST-G)anduseofa prox-imalcrosspinfixationimplantandanabsorbableinterference screw,withadistalcorticalpost(Fig.1).
Method
Table2–Factorsrelatingtotheinjury.
n(%)
Age(years)atthetimeoftheinjury
Upto20 4(25)
21–30 9(56.25)
31–40 2(12.5)
Over40 1(6.25)
Mean=26.2
Environmentatthetimeoftheinjury
Sportspractice(leisure) 13(81.25)
Others 3(18.75)
Sportpracticedatthetimeoftheinjury
Soccer 10(62.5)
Others 6(37.5)
Groundsurfacingatthetimeoftheinjury
Syntheticgrass 6(37.5)
Naturalgrass 4(25)
Parquetfloor 2(12.5)
Mat 2(12.5)
Others 2(12.5)
Intervalbetweeninjuryandsurgery(months)
<6 8(50)
6–12 2(12.5)
13–24 4(25)
>24 2(12.5)
Mean=13.85
Sideoperated
Right 7(43.75)
Left 9(56.25)
Relationshipbetweendominantandoperatedsides
Ipsilateral 6(37.5)
Contralateral 8(50)
Ambidextrous 2(12.5)
Thepresentstudy wassubmittedtothe researchethics committeeoftheFoundation forHealthSciences Teaching andResearch(FEPECS)andwasapprovedbythisbodyunder reportno.0018/2010andprotocolno.211/2010.
Non-sequentialnumberswereattributedtoeachkneethat underwentsurgery.
Theclinicalassessmentwasmadefirstlyinaconsultation office,wherethepatients’historiesrelatingtothe postopera-tiveperiodwere takenand the questions ofthesubjective InternationalKneeDocumentationCommitteequestionnaire (IKDC, 2000) and the Tegner–Lysholm Knee Scoring Scale wereappliedandscoreswereattributed.Thelatterscalehas beenvalidatedforthePortugueselanguage.7Clinical
exam-inationswereperformedinordertofindoutwhether there wasanypresenceofjointeffusion,crepitation,painor lax-ity(Lachman,pivot-shiftandanteriordrawertests),andknee goniometrywasperformed.Allthesedatawererecordedona specificform(Annex3).
Thepatientsperformedahoptest,from whicha lower-limbsymmetryindexwasobtained.Thiscomprisedtheratio ofmeasurementsofthedistancejumpedbymeansofa one-leghoponthesidethatunderwentsurgeryincomparisonwith thenon-operatedside.
Lower-limb symmetry index=(distance with operated limb/distancewithcontralaterallimb)× 100
Fig.1–Radiographonkneethatunderwentthestandard technique.
Thepatients thenunderwent radiography (X-ray) ofthe operated knee in anteroposterior (AP) view, in an upright standing position withweight-bearingin paralleland with parallelrays.Thejointlinetangentialtothecondylesandthe axesofthetunnelsthathadbeenconstructedforthegrafts tobeinsertedweretracedoutontheseradiographs,andin thecoronalplane,andtheanglesindegreesweremeasured (Fig.2).
Meanvalueswere calculatedfrom theseanglesand the patientswerethengroupedintocategories,accordingtothe anglesofthefemoralandtibialtunnelsontheAPknee radio-graphs(Table3).
Thepostoperativeresultsintermsofthefollowing vari-ableswereevaluatedforeachgroup,inrelationtothetunnel data:
• Patients’subjectivesatisfactionwiththesurgicalresult;
Fig.2–A=femoralcoronalangle/B=tibialcoronalangle.
• Limbsymmetryindex,withregardtotheone-foothoptest.
Results
Themeanangleofthetibialtunnelsinthecoronalplane(TTC) was64.81◦andthatofthefemoraltunnels(FTC)was67.68◦. Thevaluesmeasuredatbothsiteswerebetween61and70◦ formostofthepatients.Thedifferenceinalignmentbetween thetibialandfemoraltunnels(TTC–FTC)isshowninTable4. Thefactorsrelating tothepostoperative periodandthe evaluationsaccordingtothetestsappliedareshowninTable5.
Group
I
(femoral
tunnels
≤
65
◦and
tibial
tunnels
in
the
coronal
plane
≤
65
◦)
Therewerefiveindividualsinthisgroup(fourmenandone woman).Theirmeanagewas29.6years;theyoungestwas22 yearsofageandtheoldestwas46.
Thisgroupincludedthepatientswithtibialandfemoral anglesthatwere the mosthorizontalinthecoronal plane.
Table3–Distributionofpatientsintogroupsaccording toanteroposteriorradiography(coronalplane).
TTC≤65◦ TTC>65◦
FTC≤65◦ GROUPI GROUPII
FTC>65◦ GROUPIII GROUPIV
Table4–Tunnelangles.
n(%)
Coronalangleofthetibialtunnel(TTC)
≤60◦ 4(25)
61–70◦ 9(56.25)
>70◦ 3(18.75)
Mean=64.81◦
Coronalangleofthefemoraltunnel(FTC)
≤60◦ 2(12.5)
61–70◦ 11(68.75)
>70◦ 3(18.75)
Mean=67.68◦
TTC-FTC(◦)
<−10◦(varus) 1(6.25)
−10to−1◦(varus) 11(68.75)
1a10◦(valgus) 3(18.75)
>10◦(valgus) 1(6.25)
Mean=−2.87◦(varus)
Both thefemoraltunnelsand thetibialtunnelshadangles ofbetween55◦and64◦,withameanof61.2◦forthefemoral tunnelsand61◦forthetibialtunnels.Thedifferencebetween theanglesofthetibialandfemoralaxesrangedfromvarusof 9◦tovalgusof9◦.
All ofthesepatientshadsuffered injurieswhile practic-ingsports,eachonadifferenttypeofgroundsurfacing.One ofthemsaidthathehadnotreturnedtosportsactivityand declared that he was dissatisfied with the resultfrom the surgery.
ThemeanIKDCscorewas86.4(range:72–96)andthemean Lysholmscorewas94.4(range:85–100).
Table5–Factorsrelatingtopostoperativeperiod.
n(%)
Lengthoftimesinceoperation(months)
24–36 10(62.5)
36–48 6(37.5)
Mean=34.5
IKDC
95–100(Excellent) 5(31.25)
84–94(Good) 9(56.25)
65–83(Fair) 2(12.5)
Mean=89.94
Lysholm–Tegner
<91 4(25)
91–99 5(31.25)
100 7(43.75)
Mean=95.5
Hoptest(limbsymmetryindex)
<0.9 2(12.5)
0.91–0.99 6(37.5)
1.00 7(43.75)
>1.00 1(6.25)
Mean=0.968
Satisfactionwiththeresultfromthesurgery
Yes 14(87.5)
Duringthephysicalexamination,twopatientspresented positiveLachmantests.
Inthehoptest,thevaluesrangedfrom0.87to1andthe meanlimbsymmetryindexwas0.95.
Group
II
(femoral
tunnels
≤
65
◦and
tibial
tunnels
in
the
coronal
plane
>
65
◦)
Theinclusioncriteriaforthisgroupwerefulfilledbyonlyone individual:a25-year-oldmale.
Thispatientpresentedatibialanglethatwasmorevertical andafemoralanglethatwasmorehorizontal,i.e.inprinciple similartowhatisseeninthetechniqueforconstructingan arthroscopictransportalfemoraltunnel.
Thediaphysis-tunnelangleinthefemurwas60◦andinthe tibia,72◦.Thedifferencebetweentheanglesofthetibialand femoralaxeswasavalgusangleof12◦.
ThispatientpresentedmaximumscoresintheIKDCand Lysholm–Tegner questionnaires(100and 97 points, respec-tively) and had negative Lachman, anterior drawer and pivot-shifttestsinthephysicalexamination.Hislimb sym-metryindexwas1inthehoptest.Thispatientdidnotpresent any spontaneouscomplaintswhenasked duringthe study period.Hedeclaredthathewassatisfiedwiththeresultfrom thesurgeryandhereturnedtophysicalactivityeightweeks aftertheoperation.
Group
III
(femoral
tunnels
>
65
◦and
tibial
tunnels
in
the
coronal
plane
≤
65
◦)
Therewerefiveindividualsinthisgroup(fourmenandone woman. The mean age of this group was 30.4 years: the youngestwas23yearsofageandtheoldestwas40.
Thisgroupincludedpatientswithtibialanglesthatwere morehorizontalandfemoralanglesthatweremorevertical inthecoronalplane.
Theanglesformedbytheaxesofthediaphysesandtunnels were,forthefemur,between68◦and70◦(mean:69.2◦)and,for thetibia,between60◦ and64◦ (mean:61.8◦).Thedifference
betweentheanglesofthefemoralandtibialaxesvariedfrom −10◦to−4◦,i.e.alwaysinvarus.
Allofthepatientsinthisgrouphadsufferedinjurieswhile practicingsports:threeonsyntheticgrassandtwoonmats.
ThescoresfromtheIKDCquestionnairerangedfrom85to 97,withameanvalueof91.2,andthescoresfromtheLysholm questionnairewerefrom88to100,withameanof93.4.
During the physicalexamination,onepatientpresented positiveLachmanandpivot-shifttests.Oneindividualstated thathehadnotreturnedtosportsactivity,butheconsidered himselfsatisfiedwiththeresultsfromthesurgery.
Inthehoptest,themeanvalueofthelimbsymmetryindex was0.94,withaminimumof0.85andamaximumof1.
Allofthesepatientsstatedthattheyweresatisfiedwiththe postoperativeresults,althoughthereweresomespontaneous complaintssuchaspainwhilesquatting,snapsandinsecurity inperformingjumpsusingtheoperatedleg.
Group
IV
(femoral
tunnels
>
65
◦and
tibial
tunnels
in
the
coronal
plane
>
65
◦)
Therewerefiveindividualsinthisgroup(fourmenandone woman).Theirmeanagewas30years:theyoungestwas20 yearsofageandtheoldestwas45.
Theanglesformedbetweentheaxesofthediaphysesand tunnelsamongthepatientsinthisgroupwerethemost verti-calinthecoronalplane.Inthefemur,thevaluesrangedfrom 70◦to82◦ (mean:74.2◦),whileinthetibiatheyrangedfrom 66◦to73◦(mean:70.2◦).Thedifferencebetweentheanglesof thefemoralandtibialtunnelsvariedfrom−12◦to+3◦,witha meanof−4◦(varus).
Allofthepatientsinthisgrouphadsufferedinjurieswhile practicingsports:threeonnaturalgrass,oneonaparquetfloor andoneonsyntheticgrass.
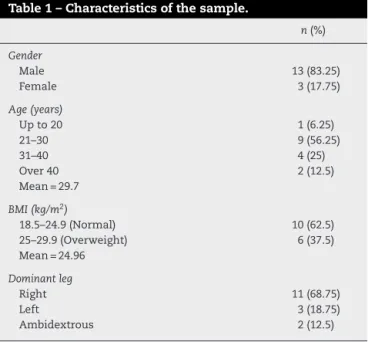
ThescoresfromtheIKDCquestionnairerangedfrom89to 96,withameanof92.2,andthescoresfromtheLysholm ques-tionnairerangedfrom95to100,withameanof97.8(Fig.3).
Duringthephysicalexamination,twopatientspresented positiveLachmanandpivot-shift signs.Oneindividualsaid
Group I Group II Group III Group IV Mean
86.4 97 91.2 92.2 90.375
95.5 97.8 93.4 100 94.4 105 100 95 90 85 80 75 IKDC Lysholm Scores Questionnaires
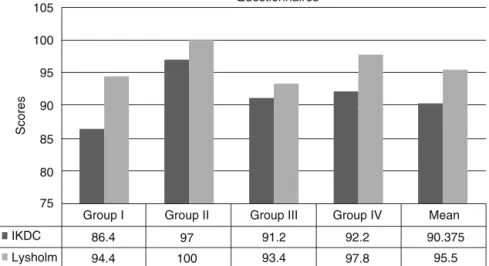
Group I Group II Group III Group IV Mean 1.01 1 0.99 0.98 0.97 0.96 0.95 0.94 0.93 0.92 0.91
Limb symmetry index (hop test)
LSI
Fig.4–Limbsymmetryindexfromthehoptest.
thathehadnotreturnedtosportsactivity,butheconsidered himselfsatisfiedwiththeresultfromthesurgery.
Inthehoptest,themeanvalueofthelimbsymmetryindex was0.99withaminimumof0.92andmaximumof1.07(Fig.4). There were spontaneous complaints with regard to increasedflexibilityandparesthesiaonthelateralfaceofthe legoperated.
Themeansobtainedfromevaluatingthestudyvariables arepresentedinTable6.
Discussion
Thepresent studywasconductedwiththeaimof correlat-ing the angles ofthe bone tunnels withthe postoperative resultsfrom ACLreconstruction. Someremarksneedtobe maderegardingthecriteriathatledtochoosingthistopicand inrelationtothemethodologyused.
Studies onpatients withACLreconstructions that com-paredtwotypesofgraft,i.e.ST-Gandthepatellartendon(PT), usingthesamefixationtechnique,haveshownthatthereis nosignificantdifference inanteriorizationofthetibia. The choicebetweengraftsthereforecontinuestobeatthe sur-geon’sdiscretion.8Thisstudydidnotaimtocomparegraft
sources.Thus,onlypatientswho underwentthe technique withST-Ggraftswereselectedinthepresentstudy.
Withregardtograftfixation,comparisonbetweendifferent fixationmethodswasnotourobjective.Thepersonal prefer-enceofthesurgeoninvolvedinthisstudy,whohashadgreat experienceinsuchprocedures,istouseaproximalcrosspin
withanabsorbableinterferencescrewandadistalpostwith ametalscrewandwasher.
Theinclusionandexclusioncriteriahadtheobjectiveof limitingtheindividualsstudiedtothosewhosolelypresented aunilateralACLinjury,therebyeliminatingthebiasrelating toassociatedinjuries.However,amongthe300patientswho underwentthissurgeryoverthethree-yearstudyperiod,only 26fulfilledallthecriteriaand,ofthese,only16returnedtothe clinicforassessmentsforthepresentstudy.
Themeasurementsofthetunnelangleswereallmadeby thesameresearcher,bymeansofsimpleradiographs.Thisis aninexpensiveandwidelyavailabletechnique,butitgivesrise tothepossibilityofvariationoftheanglemeasured accord-ingtotheincidenceoftherays.Newstudiesusingmagnetic resonanceimagingmightreduceoreveneliminatethisbias.
The patients were divided into groups according to the meanvaluesfortheanglesofthetunnelsconstructed.Thus, onlyonepatientcouldbeincludedinGroupII.Itwasprecisely
this individualwho presentedthe bestvaluesforthe post-operativeresults,amongthevariablesstudied.Inthefuture, morepatientscouldbeincludedinnewstudies,inorderto obtainalargersampleandascertainwhetherthesefindings wouldbemaintained,andalsowhethersignificancewouldbe reachedwithamoresubstantialnumberofindividuals stud-ied.
Biomechanicalstudiesoncadavershaveshownthat con-structingthefemoraltunnelatanangleof60◦inthecoronal planeminimizes theimpactofthegraft againstthe poste-riorcruciateligament(PCL)andreducesthetensiononthe graftunderflexion.Thesestudieshavealsoshownthatthe lossofflexionandanteriorlaxityaregreaterwhenthetibial tunnelisdrilledatanangle≥75◦ inthecoronalplane,and thatifthefemoraltunnelisconstructedmoreverticallyvia antranstibial route(between70◦ and 80◦), therewillbean impactagainstthePCL.These tunnelsincreasethetension onthegraftunderflexion,whichexplainsthelimitationon flexionthatisobservedclinically.ThisimpactagainstthePCL stretches the graft,whichmay explainthegreater anterior laxity.9
Ithasbeensuggestedfrominvitrostudiesthat,inorder toreducethetensionunderflexion,thetibialtunnelshould bepositionedat60◦ inthecoronalplane,becausetheangle ofthefemoraltunnelandthetensiononthegraftwouldbe controlledbythisangleandthiswouldimprovetheflexion anddiminishtheanteriorlaxity.10
Thus,theenthusiasmforconductingnewstudieswiththe aimoffindingtheidealangleforthetibialandfemoraltunnels isjustified.
Table6–Meanvaluesforthevariablesanalyzed,pergroup.
Group FTC(◦) TTC(◦)
Coronal(◦) IKDC Lysholm LSI
I 61.2 61 −0.2 86.4 94.4 0.956
II 60 72 12 97 100 1.00
III 69.2 61.8 −7.4 89.8 93.4 0.946
IV 74.2 70.2 −4 92.2 97.8 0.996
In the present study, it was observed that the groups analyzed presented differences in the outcome variables accordingtothetunnelangles.GroupI,inwhichthetunnels weremosthorizontal(meanvalueforthetibialtunnel=61◦ andforthefemoraltunnel,61.2◦),had thelowestscorefor theIKDCquestionnaire(mean:86.4)and thesecondlowest scorefortheLysholmquestionnaire(mean=94.4)andforthe limbsymmetry(mean:0.956).GroupII,inwhichthetibial tun-nelwasmorevertical(72◦)whilethefemoraltunnelremained morehorizontal(60◦),showedthebestresultsandthevalues werethemaximumpossiblefortheIKDC,Lysholmandlimb symmetryindexvariables.GroupIII,inwhichthefemoral
tun-nelwasmorevertical(mean:69.2◦)whilethetibialtunnelwas morehorizontal(61.8◦),had thesecond worstIKDC(mean: 91.2)andtheworstvaluesfortheLysholmvariables(93.4)and forthelimbsymmetryindex(0.946).GroupIV,inwhichthe
tibialtunnel(70.2◦)andfemoraltunnel(64.2◦)werethemost vertical,showedthesecondbestresultsforthethreevariables: Lysholm(97.8),IKDC(92.2)andlimbsymmetryindex(0.996).
Conclusion
Fromthedataobtainedinthepresentstudy,itcanbe con-cludedthattheresultsfromgroupsIIandIVweresuperior tothosefromgroupsIandIII.Thetwogroupswiththebest
indicesweretheoneswiththetibialtunnelmorevertical.The highestscoresfromthe IKDC,Lysholm andlimbsymmetry indexwereobtainedfromapatientinwhomtheangles con-structedwere60◦forthefemoraltunneland72◦forthetibial tunnel,whichgaverisetoavarusalignmentforthetunnels. Theworstresultsforthevariablesstudiedwerefoundinthe groupinwhichthetibialtunnelwasmosthorizontalandthe alignmentofthetunnelswasmostdisplacedtowardvalgus. Nonetheless,furtherstudiesareneededinordertoconfirm thesefindings.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Annex
1.
Lysholm
questionnaire.
Limping(5points) Pain(25points)
Never=5 None=25
Slightorperiodic=3 Occasionalorslightduring heavyexercise=20
Annex1(Continued)
Severeorconstant=0 Limpingduringheavy exercise=15
Considerableduringorafter walkingformorethan 2km=10
Support(5points) Considerableduringorafter walkingforlessthan2km=5
Never=5 Constant=0
Stickorcrutch=2
Impossible=0 Swelling(10points)
None=10
Locking(15points) Withheavyexercise=6 Nolockingorfeelingof
locking=10
Withordinaryexercise=2
Thereisafeeling,but withoutlocking=10
Constant=0
Occasionallocking=6
Frequent=2 Goingupstairs(10point)
Jointlockedduring examination=0
Noproblem=10
Slightlyimpaired=6
Instability(25points) Onestepatatime=2 Neverunstable=25 Impossible=0 Rarely,duringathletic
activitiesandother heavyexercises=20
Squatting(5points)
Frequentlyduring athleticactivitiesand otherheavyexercises (orincapableof participation)=15
Noproblem=5
Slightlyimpaired=4 Occasionallyduring
dailyactivities=10
Notbeyond90degrees=2
Frequentlyduringdaily activities=5
Impossible=0
Ateachstep=0
Totalscore:
r
e
f
e
r
e
n
c
e
s
1. ShimokochiY,ShultzSJ.Mechanismsofnoncontactanterior cruciateligamentinjury.JAthlTrain.2008;43(4):396–408. 2. StarkJ.Twocasesofrupturedligamentsofthekneejoint.
EdinbMedSurg.1850;74:267–71.
3. Hey-GrovesEW.Operationfortherepairofthecrucial ligaments.Lancet.1917;2:674–5.
4. CampbellWC.Reconstructionoftheligamentsoftheknee. AmJSurg.1939;43:473–80.
5. MaceyBH.Anewoperativeprocedureforrepairofruptured cruciateligamentsofthekneejoint.SurgGynecolObstet. 1939;69:108–9.
6. BollenS.Advancesinthemanagementofanteriorcruciate ligamentinjury.CurrOrthop.2000;14:325–8.
7.PeccinMS,CiconelliR,CohenM.Questionárioespecíficopara sintomasdojoelhoLysholmKneeScoringScale’:traduc¸ãoe validac¸ãoparaalínguaportuguesa.ActaOrtopBras. 2006;14(5):268–72.
8.AbdallaRJ,MonteiroDA,DiasL,CorreiaDM,CohenM,Forgas A.Comparac¸ãoentreosresultadosobtidosnareconstruc¸ão doligamentocruzadoanteriordojoelhoutilizandodoistipos deenxertosautólogos:tendãopatelarversussemitendíneoe grácil.RevBrasOrtop.2009;44(3):204–7.