SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Epidemiology
of
pelvic
ring
fractures
and
injuries
夽
Gilberto
José
Cac¸ão
Pereira,
Erick
Ribeiro
Damasceno
∗,
Daniel
Innocenti
Dinhane,
Francisco
Marques
Bueno,
Jaqueline
Bartelega
Rodrigues
Leite,
Bruno
da
Costa
Ancheschi
UniversidadeEstadualPaulista(Unesp),FaculdadedeMedicinadeBotucatu(FMB),DepartamentodeCirurgiaeOrtopedia,Grupode CirurgiadoQuadril,Botucatu,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received27May2016 Accepted18July2016 Availableonline19May2017
Keywords:
Bonefractures/epidemiology Pelvicbones/injuries Epidemiologicstudies
a
b
s
t
r
a
c
t
Objective:Thisstudyevaluatedthepelvicringfracturesandinjuriesinpatientsadmittedto andtreatedatthiswardbetweenAugust,2012andJanuary,2014.
Methods:66patientsweresubmittedtotreatmentprotocolsaccordingtotheirage,gender, skincolor,injurymechanism,locationofthetrauma,classificationoftheirinjuries, emer-gencyintervention,associatedinjuries,injuredsideofthebody,treatment,andmortality. Themostrelevantdatawereclassifiedaccordingtostatisticprocedures,suchasGoodman’s associationtest.MeasureswerecomparedwithStudent’st-testandanalysisofvariance associatedwithTukey’smultiplecomparisontest.
Results:Themeanagewas47years;whiteraceandmalegenderweremostcommon.Car ortruckaccidentwasthemostcommoncauseofinjuries,whichoccurredmainlyinurban sites.TypeAinjurieswerethemostfrequent.16.6%ofthecasesweresubmittedto emer-gencysurgery.42.4%displayedassociatedinjuries.Therightsideofthebodywasthemost commonlyaffectedside.Non-invasivetreatmentwasmostcommonlyused.Deathwasthe outcomein3%ofthecases,associatedtohigh-energytrauma.
Conclusions:Pelvicringfracturesandinjuriesaremoreoftenverifiedamongmales.In gen-eralandamongyoungerindividuals,trafficaccidentsarethemostcommoncauseofthe injury,whileamongtheelderly,ordinaryfallsarethemostcommonlyverifiedcause.The majorityofthoseinjuriesaresufferedinurbanareas.TypeAfracturesaremorefrequent. Themajorityofcasesdonotrequireemergencyinterventionnordotheyfeatureassociated injuries.Non-invasivetreatmentismostcommonanddeathoutcomesareassociatedto high-energytraumaswithsevereinjuries.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheUniversidadeEstadualPaulista(Unesp),FaculdadedeMedicinadeBotucatu(FMB),DepartamentodeCirurgia eOrtopedia,GrupodeCirurgiadoQuadril,Botucatu,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](E.R.Damasceno).
http://dx.doi.org/10.1016/j.rboe.2017.05.012
Estudo
epidemiológico
das
fraturas
e
lesões
do
anel
pélvico
Palavras-chave:
Fraturasósseas/epidemiologia Ossospélvicos/lesões Estudosepidemiológicos
r
e
s
u
m
o
Objetivo: Estudodasfraturas/lesõesdoanelpélvicoatendidasetratadasnesteservic¸ode agostode2012ajaneirode2014.
Métodos: Elaborou-seumprotocoloparaos66pacientes,consideraram-seosdados:idade, sexo,cor,mecanismodalesão,localdotrauma,classificac¸ãodaslesões,intervenc¸ãode urgência,lesõesassociadas,ladoacometido,tratamentoeóbito.Paraosdadosdemaior interesseforamusadososprocedimentosestatísticosqueenvolveramotestedeassociac¸ão deGoodmaneastécnicasdecomparac¸õesdemedidaspormeiodotestetdeStudenteda análisedevariânciacomplementadacomascomparac¸õesmúltiplasdeTukey.
Resultados:Aidademédiafoide47anos;pacientesdosexomasculinoebrancosforammais frequentes.Acausamaiscomumdaslesõesfoiacidentecarro/caminhãoeazonaurbana foiolocalondeelasmaisocorreram.FraturastipoAforamasmaisfrequentes.Em16,6% dospacientes,foinecessáriacirurgiadeurgênciae42,4%apresentaramlesãoassociada.O ladodireitofoimaisacometido.Otratamentoincruentofoiomaisusadoeoóbitoocorreu em3%,emcasosdetraumadealtaenergia.
Conclusões: Asfraturas/lesõesdoanelpélvicosãomaisfrequentesnosexomasculino.De modogeraleemjovens,oacidentedetrânsitoéomecanismomaisfrequente,jáemidosos équedabanal.Amaioriadaslesõesocorrenazonaurbana.FraturasdotipoAsãoasmais frequentes.Amaiorianãonecessitadeintervenc¸ãodeurgênciaenãoapresentalesões associadas.Otratamentoincruentoéomaisusadoeosóbitosestãoassociadosatrauma dealtaenergiacomgraveslesõesassociadas.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Fracturesandinjuriesofthepelvicring,whichmayormaynot beassociatedwithseveretrauma,aregenerallynot consid-eredtobefrequent,accountingforonly2–8%ofallfractures. However,inpolytraumatizedpatientstheoccurrenceofthis typeofinjuryismuchhigher,beingobservedin20–25%of cases.1Fracturesofthepelvicringinyoungindividualsmost
oftenoccurasaconsequenceofhigh-energytraumasuchas carandmotorcycleaccidentsandfallsfromgreatheights.In theelderly, they are usuallycausedbylow-energy trauma, mostcommonlyfallfrom own height,mainly dueto bone porosity.1Youngpatientswithpelvicringfracturesorinjuries
due tohigh-energy trauma should beinitially assessed by amultidisciplinaryteam,because theyoftenhavemultiple injuriesandare subjecttomajorbleeding.Bleeding inthis typeofinjuryis moreseverewhen associatedwith unsta-ble pelvic fractures,which, although infrequent,present a highmortalityrateof19–31%.2–4Inturn,elderlypatientswith
fracturesduetominortraumagenerallydonotpresent com-plications.Inrecentyears,aconsiderablenumberofstudies relatedtothe careand immediateor latecomplicationsof thistypeofinjuryhavebeenpublished, whichis undoubt-edlypraiseworthy,sincetheyincreasinglyinformandguide the professionals involved insuch care,characterizing the importanceandseverityoftheinjury,especiallyinpolytrauma
cases.5–9However,amuchsmallerproportionofpublications
are related to epidemiological data, regional or otherwise, aboutfracturesandinjuriesofthepelvicring,whichalsohave veryimportantinformation,especiallyregardingthe charac-terizationandappropriatenessofcareforsuchaninjury.3,10,11
Therefore, this study soughtto analyze and compare vari-ousdata,suchasage,mechanismandsiteofinjury,typeof fracture,emergencyinterventions,anddefinitivetreatment, amongothers,referringtothecasesoffracturesandinjuries ofthepelvicringthatoccurredinthisregionandweretreated inthisservice.
Material
and
methods
Thestudyincluded66patientswithpelvicringfracturesand injuriestreatedatthisservicefrom August2012toJanuary 2014,whoagreedtoparticipateinthestudy.
anteriorexternalfixator(two),nointervention(three), laparo-tomy(four). Associatedinjuries:no associatedinjury(one), urethral/bladder injury(two),paraplegia (three),other frac-tures/dislocations (four), abdominal organ injuries/cranial trauma (five). Affected ring side: right (one), left (two), both (three), pubic symphysis diastasis (four). Pelvic ring fracture/injuryclassification(Tileclassification):typeA,12type
B,typeC,andtheirsubdivisions.Definitivetreatment: non-surgical(one),iliosacralscrew(two),iliosacralscrewandplate (three),iliosacralscrewandexternalfixator(four),plates(five), platesandexternalfixator(six),externalfixator(seven). Occur-renceofdeath:no(one),yes(one).
Inthestatisticalanalysisofthepresentstudy,the associa-tionamongthevariablesofinterestwasassessedthroughthe Goodman13testforcontrastsamongandwithinmultinomial
populations.When thecontingencytablepresentedalarge numberofnullcells,theresultswereonlydescriptive.Inthe caseoftheGoodmantest,resultswere presentedregarding theirsignificance(p<0.05)bylowercaseletters(comparison ofrows bycolumn) and uppercase letters (comparison of columnsbyrow).Thesedatashouldbeinterpretedasfollows: tworesponseswiththesameletter donotdifferfromeach other.
Regarding the association of age and sex, injury mech-anism, and classification of the pelvic ring fracture/injury mechanism(Tile),Student’st-testwasusedforsex,and mul-tivariateanalysisofvariancesupplementedbytheTukeytest wasusedforthevariablesinjurymechanismandpelvicring fracture/injuryclassification(Tile).
ThestudywasapprovedbytheInstitutionalReviewBoard ofthisservice(CEP4296/2012).
Results
Theresultswerepresentedinadescriptivemanner,aswell asintableswithacomparisonofsomedatathattheauthors consideredimportant.
Theageofthe individualsanalyzedrangedfrom3to86 years(meanof47).Meanageinrelationtosexwas55.3years forfemales and41.9years formales.Asforsex,therewas predominanceofmales(57.5%ofthesample).Regarding eth-nicity,thehighestpercentage(69.6%)waswhite,followedby blacks(16.6%).
The following injury mechanisms were observed:
Car/truckaccident 17(25.7%)
Motorcycleaccident 13(19.6%) Fallfromownheight 17(25.7%) Fallfromheight>1m 4(6%) Horsefall/saddletrauma 5(7.5%)
Tractoraccident 2(3%)
Beingrunover(8.8%) 8(12%)
Observation:Inthemechanismfallfromownheight,81% oftheindividualswerefemale.
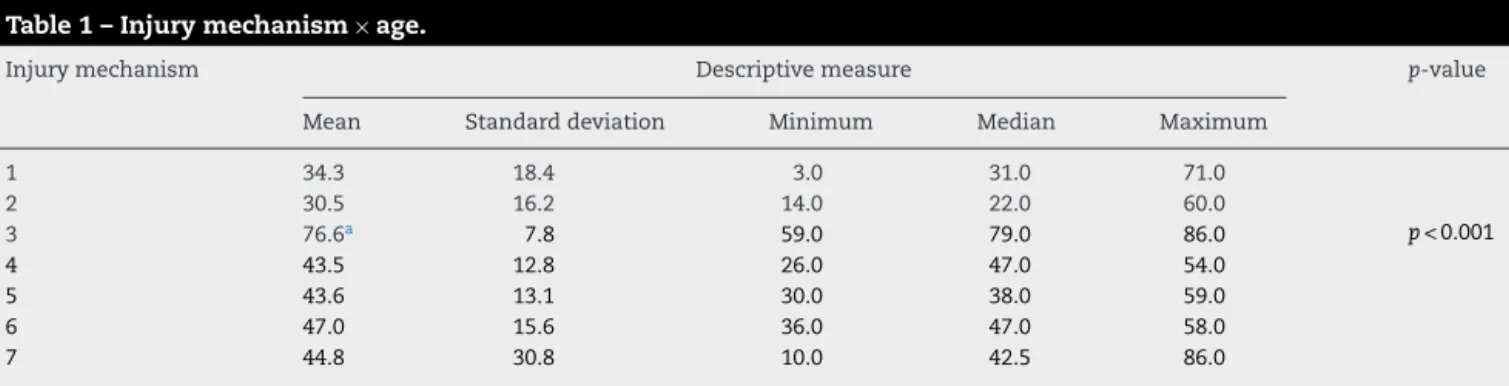
Theinjurymechanismwascomparedwiththeageofthe patients(Table1).
Injuriesoccurredinthefollowingplaces:
Urbanarea 22(33.3%)
Highway 19(28.7%)
Ruralarea 8(12.1%)
Home/organization 17(25.7%)
Table2showsanassociationbetweentheplaceof occur-renceoftraumaandinjurymechanism.
Regardingtheclassificationofpelvicringfractures/injuries (Tile),thefollowingwereobserved:
TypeA(stable) 36(54.5%)
(themostfrequenttypewasA2.3,observedin61%ofcases).
TypeB(rotationally unstableandvertically stable)
19(28.7%)
TypeC(rotationallyand verticallyunstable)
11(16.6%)
Table 3 presents a comparison between the clas-sification of fractures/injuries (Tile) and age of patients.
Table 4 describes the association between
pelvic ring fracture/injury mechanism and patients’ gender.
Regardingthepresenceorabsenceofassociated (concomi-tant)injuries,thefollowingwasobserved:
Table1–Injurymechanism×age.
Injurymechanism Descriptivemeasure p-value
Mean Standarddeviation Minimum Median Maximum
1 34.3 18.4 3.0 31.0 71.0
2 30.5 16.2 14.0 22.0 60.0
3 76.6a 7.8 59.0 79.0 86.0 p<0.001
4 43.5 12.8 26.0 47.0 54.0
5 43.6 13.1 30.0 38.0 59.0
6 47.0 15.6 36.0 47.0 58.0
7 44.8 30.8 10.0 42.5 86.0
Table2–Placeoftrauma×injurymechanism.
Injurymechanism Place Total
Urbanarea Ruralarea Highway Home/organization
1 3(17.7) 1(5.9) 13(76.4) 0(0.0) 17
2 9(69.2) 0(0.0) 4(30.8) 0(0.0) 13
3 0(0.0) 0(0.0) 0(0.0) 17(100.0) 17
4 4(100.0) 0(0.0) 0(0.0) 0(0.0) 4
5 0(0.0) 5(100.0) 0(0.0) 0(0.0) 5
6 0(0.0) 2(100.0) 0(0.0) 0(0.0) 2
7 6(75.0) 0(0.0) 2(25.0) 0(0.0) 8
Table3–Tileclassification×age.
Classification Descriptivemeasure p-value
Mean Standarddeviation Minimum Median Maximum
A 55.6a 27.3 3.0 65.5 86.0 p<0.01
B 43.4 16.8 10.0 41.0 71.0
C 27.4 8.4 15.0 27.0 40.0
a (p<0.05)classificationAversusclassificationC.
Table4–Injurymechanism×sex.
Sex Mechanism Total
1 2 3 4 5 6 7
F 6(22.2)aAB 5(18.5)aAB 12(44.5)bB 0(0.0)aA 0(0.0)aA 0,(00)aA 4(14.8)aAB 27
M 11(28.2)aA 8(20.5)aA 5(12.8)aA 4(10.3)aA 5(12.8)aA 2(5.1)aA 4(10.3)aA 39
Table5–Associatedinjuries×sex.
Sex Associatedinjuries Total
1 2 3 4 5
F 16(59.3)aB 1(3.7)aA 0(0.0)aA 10(37.0)aB 0(0.0)aA 27
M 22(56.5)aB 2(5.1)aA 2(5.1)aA 11(28.2)aAB 2(5.1)aA 39
Noassociatedinjury 38(57.5%) Associatedinjury 28(42.4%)
Observation: Fractures/dislocations (single or multiple) werethemostfrequentlyassociatedinjuries,presentin75% ofthecaseswithassociatedinjuries.
Theotherassociatedinjuriesobservedwerethoseofthe urethra/bladder,abdominalorgans,andcranialtrauma.
Table5presentstheassociationbetweenthepresenceor absenceofassociated(concomitant)injurytothepelvicring injuryandthepatients’sex.
Regardingtheneedforemergencyintervention,the follow-ingwasobserved:
Noemergencyintervention 55(83.3%) Emergencyintervention 11(16.6%)
Typeofintervention:
- Anteriorexternalfixator–six. - C-clamp–five.
- Laparotomy(associatedwithclamp)–one.
Table6–Urgencyinterventionstatus(typeof fixation)×injurymechanism.
Mechanism Interventions Total
Clamp Fixator No
1 2(11.8)aA 4(23.5)aAB 11(64.7)bB 17
2 0(0.0)aA 2(15.4)aA 11(84.6)bB 13
3 0(0.0)aA 0(0.0)aA 17(100.0)bB 17
4 1(25.0)aAB 0(0.0)aA 3(75.0)bB 4
5 0(0.0)aA 0(0.0)aA 5(100.0)bB 5
6 2(100.0)bB 0(0.0)aA 0(0.0)aA 2
7 0(0.0)aA 0(0.0)aA 8(100.0)bB 8
- Reductionofhipdislocation(associatedwithringfixator)– one.
- Linearexternalfixator(associatedwithringclamp/fixator) –three.
- Bladder/urethraintervention(associatedwithringfixator)– two.
Table7–Classificationoftheinjury×trauma mechanism.
Mechanism Classification Total
A B C
1 7(41.2)aA 5(29.4)abA 5(29.4)aA 17
2 6(46.2)aA 4(30.8)abA 3(23.0)aA 13
3 17(100.0)bB 0(0.0)aA 0(0.0)aA 17
4 1(25.0)aAB 3(75.0)bB 0(0.0)aA 4
5 1(20.0)aAB 4(80.0)bB 0(0.0)aA 5
6 0(0.0)aA 1(50.0)abA 1(50.0)aA 2
7 4(50.0)abA 2(25.0)abA 2(25.0)aA 8
Table7showstherelationshipbetweenthepelvicring frac-tures/injuriesclassification(Tile)andtraumamechanism.
Table8presents acomparisonbetween themechanism ofpelvicringfractures/injuries withpresenceorabsenceof associatedinjury.
Regardingsideoftheringthatwasaffected(local),the fol-lowingwasobserved:
Right 30(45.4%)
Left 23(34.8%)
Both 9(13.6%)
Pubicsymphysisdiastasis 4(6%)
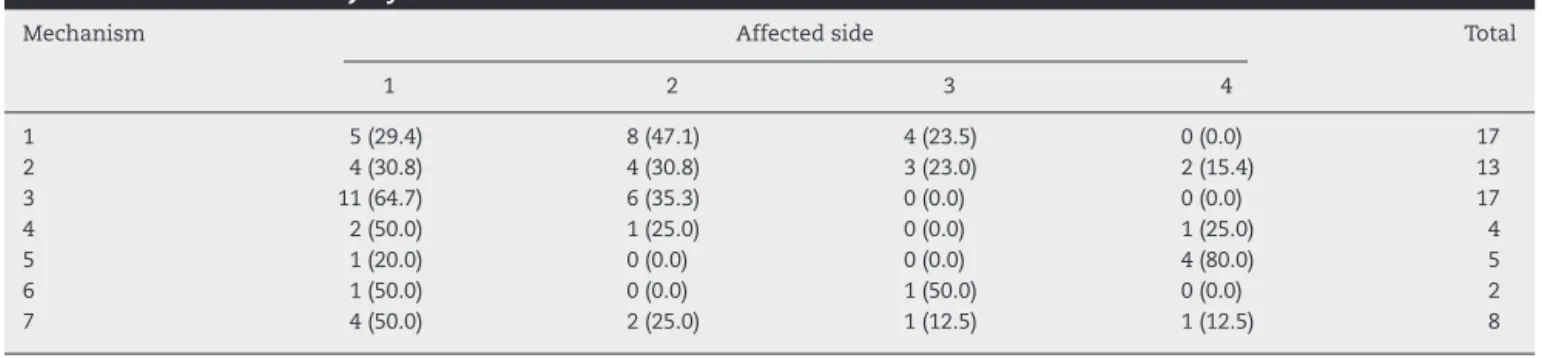
Table9showsanassociationbetweenaffected sideand injurymechanism.
Regarding definitive treatment, the following was observed:
Non-surgical 42(63.6%)
Surgical 24(36.4%)
Materialsused
- Plate(publicsymphysis/iliosacral)–13. - Iliosacralscrew+plate(pubicsymphysis)–five. - Iliosacralscrew–three.
- Anteriorexternalfixator–two. - Anteriorexternalfixator+plate–one.
Regardingtheoccurrenceornotofdeath,thefollowingwas observed:
No 64(96.9%)
Yes 2(3%)
Observation: Deaths occurred in cases of high-energy trauma(trafficaccident)withtypeBorCpelvicringinjuries, inadditiontosevereassociatedinjuries.
Discussion
The data on age (mean 41.9 years), sex (more frequently males),andethnicity(predominantlywhites)observedinthe presentsample,ingeneral,wereveryclosetothosepresented intheliterature.Kobbeetal.14reportedameanageof47.3
yearsintheircasesofpelvicringinjury.JezekandDzupa,15in
anepidemiologicalstudyonageandmechanismofpelvicring
injury,reportedaslightlyhighermeanage(51years); strati-fiedbysex,meanageoffemalepatientswas53whilemale patientswas49.Gansslenetal.,3inasimilarepidemiological
study,alsoreportedahigherincidenceofpelvicringinjuries inmales,inaproportion(56.7%)veryclosetothatobservedin thepresentsample(57.5%).Chueireetal.,9inan
epidemiolog-icalstudy,reportedalargernumberofmaleswithringinjuries (67%); white subjects alsorepresented a higherpercentage oftheirsample.Onlythemeanageoftheircases(37years) waslowerthanthatobservedinthepresentstudy.Devarinos etal.11reportedtheirexperienceinpelvicringinjuriesin
Ire-land,havingalsoobservedamuchhigherpercentageofmales (76%),withameanageof36.5years.
Itwasobservedthat,generallyspeaking,theliteraturealso presentsahigherincidenceofmalesexinthistypeoftrauma, exceptinspecificcases,asreportedbyAlnaibet al.,16 who
assessedonlypelvicringinjuriesduetolow-energytrauma (osteoporoticbones)andfoundahigherincidenceinfemales. In relationshiptomean age, the authorsconsider that the valueobservedinthepresentstudywasslightlyhigherthan thoseobservedinsomeotherstudies,asthepresentsample includednumerouselderlyindividuals.
Regarding themechanismofthepelvicringinjuries,we observedthat,ingeneral,accidentsinvolvingtransportation vehicles(cars/trucksandmotorcycles)werethemostfrequent causes ofinjuries,accounting for45.3%ofthe total. When includingthemechanism“beingrunover”(alsocausedbythe sametypeofvehicle),totalofinjuriescausedbytraffic acci-dentswas57.5%,whichreinforcesthefactthattheseinjuries werecaused,forthemostpart,bymotorvehicles.Devarinos etal.,11 inalongfollow-upofpelvicringinjuries(10years),
indicatedthatthemostfrequentinjurymechanismwastraffic accidents(74%).Freitasetal.,10inaliteraturereviewof
stud-iesonpelvicringfracturesinrecentdecades,observedthat themostprevalenttraumamechanismswerethoserelatedto traffic.Chueireetal.9 reportedavery similarpercentageto
thatobservedinthepresentstudy;intheirstudy,pelvicring injurieswerecausedbycaraccidentsin23%ofcases(25.7%in thepresentstudy)andbymotorcycleaccidentsin19%(19.6% inthepresentstudy).
In thecomparisonofthemechanism ofinjury withthe age ofthepatients, anexpectedbut importantfinding was observed:thesignificantpredominanceoftheelderlyincases in whichthe injury was causedby afallfrom ownheight (mechanism 3).Furthermore,itwas alsoobservedthat the maintraumamechanisminadolescentsoryoungadultswas trafficaccidents(mechanisms1and2),withindividualsinside thevehicle.JezekandDzupa,15intheirstudyontheinfluence
ofageonthemechanismofringfractures,reportedthat com-monfallwasthemostfrequentcauseofthistypeofinjury intheelderlyand,ofthose,femaleswerethemostaffected, aresultsimilartothatobservedinthepresentstudy,Those authorsalsonotedthatmenweresignificantlymoreinvolved infracturesresultingfrommotorcycleaccidentsandfallsfrom stairs.Krappinger et al.,4 in theirstudy onpelvic fractures
Table8–Injurymechanism×associatedinjury.
Mechanism Associatedinjury,n(%) Total
1 2 3 4 5
1 9(52.9) 0(0.0) 2(11.8) 6(35.3) 0(0.0) 17
2 5(38.4) 2(15.4) 0(0.0) 6(46.2) 0(0.0) 13
3 13(76.5) 0(0.0) 0(0.0) 4(23.5) 0(0.0) 17
4 3(75.0) 1(25.0) 0(0.0) 0(0.0) 0(0.0) 4
5 5(100.0) 0(0.0) 0(0.0) 0(0.0) 0(0.0) 5
6 0(0.0) 0(0.0) 0(0.0) 1(50.0) 1(50.0) 2
7 3(37.5) 0(0.0) 0(0.0) 4(50.0) 1(12.5) 8
Table9–Affectedside×injurymechanism.
Mechanism Affectedside Total
1 2 3 4
1 5(29.4) 8(47.1) 4(23.5) 0(0.0) 17
2 4(30.8) 4(30.8) 3(23.0) 2(15.4) 13
3 11(64.7) 6(35.3) 0(0.0) 0(0.0) 17
4 2(50.0) 1(25.0) 0(0.0) 1(25.0) 4
5 1(20.0) 0(0.0) 0(0.0) 4(80.0) 5
6 1(50.0) 0(0.0) 1(50.0) 0(0.0) 2
7 4(50.0) 2(25.0) 1(12.5) 1(12.5) 8
fracturesduetocommontraumasincreaseswithage;the inci-denceinthegeneralpopulationis2–37/100,000individuals, increasingto92/100,000inindividualsagedover60yearsand to446/100,000inthoseagedover85years.Baloghetal.,17inan
epidemiologicalstudyonthesametypeofinjury,reportedthat low-energytraumafracturemechanismwasfallfromheight oflessthan1minallcases.
Aspreviouslymentioned,arelationshipbetween adoles-cents/youngadultsandtrafficaccidentswasalsoobservedin thepresentstudy(Table1).Freitasetal.,10inananalysisof
theliteratureonthesubject,commentedthattrafficaccidents aregenerallyamongthemostfrequentcausesandpresenta higherriskintheyoungmalepopulation.Devarinosetal.11
alsomentionedtrafficaccidentsinpelvicringinjuries;intheir work,thetypicalpatientwasmaleandagedaround30years. In relationship to the place where the injuries of the pelvicringoccurred,theurbanzonewasthemostfrequent placeinthe present study.In the comparisonoftheplace ofoccurrencewiththeinjurymechanism(Table2), motorcy-cleaccidents(mechanism2)intheurbanareastoodout.The sameTablealsoindicatesthatmechanisms5and6,accidents withanimals(horses)andtractors,standoutintheruralarea, car/truckandmotorcycleaccidents(mechanisms1and2)on thehighway;athomes/institutions,100%ofthecaseswereof fallfromownheight(mechanism3).Theauthorsbelievethat theseresultsarecompatiblewithtypeoftraumaandplace ofoccurrence. Nonetheless, no references in the literature regardingtheseparameterswereretrieved.
Regarding the classification of pelvic ring injuries, the authors emphasize that in the present study, of all frac-tures/injuries, type A (stable) was the most frequent and, amongthese,subtypeA2.3 (isolatedfractureoftheanterior
region of the ring – one or four branches) was the most
common.ThesewerefollowedbytypesB(rotationally unsta-ble and vertically stable) and C (rotationallyand vertically unstable). Table3(classificationbyage)presentsa predom-inanceoftypeA(stable)fracturesintheelderlyandoftype C(rotationallyandverticallyunstable)inyoungerindividuals, i.e.,thelatterhadthemostsevereinjuries.Grotzetal.18also
associatedtheseverityofringinjurieswithageandreported thatthemostseriousinjuries(includingboneexposure) usu-allyaffectyoungadultmalesasaresultoftrafficaccidents. Gansslen et al.,3 in epidemiological study on pelvic ring
injurieswithalargesample,alsofoundthattypeAfractures (stable)werethemostfrequent,accountingfor54.8%ofthe cases(includinghigherinvolvementoftheischiopubicbones). Moreover,intheirstudytheorderwassimilartothatobserved inthepresentstudy:typeB(rotationallyunstableand verti-callystable)wasthesecondmostcommon,followedbytypeC (rotationallyandverticallyunstable).Chueireetal.9reported
that type A injuries were the most common,occurring in 55%ofthesample,andwerealsorelatedtotheelderly,with involvementofischiopubicbranches;inthatstudy,the sub-typeA2.2wasthemostcommon.Thoseauthorsalsoobserved
typeB(30%)asthesecondmostcommon,followedbytype C(15%).Itwasobservedthatregardingtheorderandthe fre-quencyoffracturetypes,aswellaspercentageandtheplace ofinvolvement,theresultswereveryclosetothoseobserved inthepresentstudy.Freitasetal.,10inaliteraturereviewfrom
indexeddatabases,soughttoanalyzetheevolutionofpelvic ringfracturesinthepastdecades;theseauthorsalsoobserved typeAasthemostfrequent,followedbytypesBandC.
offemales.Thus,inmales,thedistributionofmechanismof injurywashomogeneous,whereasinfemales,fallfromown heightwasnoteworthy.JazekandDzupa15commentedonthe
mechanismofpelvicringinjuriesandalsoreportedthat frac-turesduetosimpletraumaweresignificantlymorecommon inolderwomen;thewomeninthisagegroupwereeightyears olderthanthemen.Alnaibetal.,16inastudyonpelvicring
fractures inthe elderly caused by-low energytrauma, also reportedamuchhigherpercentageofinvolvementinfemales, 80.4%ofthecases.
Regarding the presence of injuries/fractures associated withpelvicringinjuries,theliteraturepresentsacertain vari-ation.Chueireet al.9reported ahigher percentageofcases
ofotherinjuriesassociatedwithpelvicringfracturesthanof isolatedfractures;54%oftheircasesshowedsometype asso-ciatedinvolvement.Regardingthetypeofconcomitantinjury, theauthorsalsoobserved,asinthepresentstudy,a preva-lenceoffractures/dislocations inother places. Richardand Tornetta,19inastudyontheemergencytreatmentonpelvic
injuriesringwiththeC-clamp,reportedthat37.5%ofcases had other fractures associated with the pelvic ring injury. Sagietal.,20 inastudyofseriousinjuriesofthepelvicring
(verticalinstability),observedconcomitantinjuriesin36.2% ofpatientsandfoundbladderruptureasthemostcommon injuryassociatedwiththistypeofringinjury.Inthepresent study,bladderinjurywasmuchlessfrequent,butitis notewor-thythatalltypesofringfractures/injurieswereincluded,not onlythemoreseverecases.Inturn,Gansslenetal.,3inan
epi-demiologicalstudywithalargesampleofpelvicringinjuries includingalltypes,observedthatmosthadsomekindof asso-ciatedinjury;only30.2%ofthecaseswereisolatedinjuries.In thepresentstudy,injuriesassociatedwiththoseofthepelvic ring,althoughoccurringinaconsiderablepercentage(42.44% –Table9),werenotashighasthoseobservedinthe litera-ture.Theauthorsbelievethattheconsiderablenumberofless severefractures(TypeA)inthissampleandthelesser involve-mentofotherareasororganshasinfluencedthefindingthat the general percentage ofassociated injuries was not ele-vated.Alsoinrelationtoassociatedinjuries,genderofpatients (Table5)were comparedin orderto assess apossible pre-dominance.However,nosignificantcorrelationwasobserved. Regarding the needforemergency interventioninpatients whosufferedpelvicringfracture/injury,itwasobservedthat inthegreatmajority(83.3%)ofcasestherewasnoneedfor urgentintervention.Incaseswheretheseinterventionswere made,orthopedicinterventionswerethemostfrequent,with abalancebetweentheuseofC-clampandanteriorexternal fixator.Theotheremergencyinterventionswererecordedand numbered,butnotconsideredseparately,sincetheywere per-formed(concomitantly)inthesamepatientswhounderwent orthopedicinterventions.Chueireet al.9 reportedan
emer-gencyinterventionrate of32% intheircasesofpelvicring fractures;orthopedicinterventionsandlaparotomywerethe mostfrequent,buttheauthorsdidnotspecifywhetherthe procedures were done separately or in the same patients. Baloghetal.,17 inanepidemiologicalstudy ofringinjuries,
indicatedthat15%ofthecasesofhigh-energytraumarequired emergencyringfixation.Inturn,Pisanisetal.,1 assessinga
large sample of patients with pelvic ring injuries to com-parethestabilizingringmethodsintheemergencytreatment,
indicated that only3.4%ofpatients underwent emergency orthopedicprocedures;ofthese,theC-clampwasoneofthe mostoftenused.
Table 6compares the need for emergency intervention withthemechanismoftheinjury; asignificant association was observed, notably between the mechanisms car/truck and motorcycle accidents, together with tractor accidents (high-energytrauma)and needforemergencyintervention, especially with the anterior external fixator and C-clamp. Pisanis et al.1 alsoreported thatthe pelvicring injuriesin
theirsamplethatrequiredurgentinterventionfor stabiliza-tionresultedfromhigh-energytrauma,andthattheC-clamp wasthemostusedmethod.Abrassartetal.,21inastudyon
emergency treatment inunstable pelvic ring injuries asso-ciatedwithhemodynamicinstability,reportedthatallcases werehigh-energytrauma,suchasmotorvehicleaccidentsor fallsfromgreatheights.Theauthorsemphasizethat,ofthese, thevastmajority(80%)requiredringfixationwithexternal fix-atororC-clamp.Brumetal.,22inastudyonseriousinjuries
to the pelvic ring that included onlypolytrauma patients, reportedthatemergencyringfixation,whetherwithC-clamp oranothermethod,wasnecessaryin35%ofthesample.Grotz etal.,18inastudyonthetreatmentofopenfracturesofthe
ring,didnotdiscusspercentages,butreportedthatincases requiringemergencyinterventiontostabilizethering,theuse ofC-clamporanteriorexternalfixatorisrecommended.
Mechanismoftraumawascomparedwiththe classifica-tionoftheinjuries(Table7).WeobservedthatintypeA(stable fracture) injuries, the mechanism of fall from own height, i.e.,alow-energytrauma,isnoteworthy;intypeB(rotational instabilityandverticalstability),themostprevalent mecha-nismswerefallfrommorethan1mandhorseaccident,which are consideredmoderateorhigh-energytraumas. IntypeC (rotationalandverticalinstability)therewasapredominance ofcar/truckandmotorcycleaccidents,i.e.,onlyhigh-energy traumas. Krappinger et al.4 examined cases of pelvic ring
fracturesinosteoporoticbonesandreportedthatthetypical fracturesofthissegmentarestableandthatthemechanism ofinjuryistrivialtrauma,suchasfallfromownheight.Loon et al.,23 ina study on the treatment of typeB pelvic ring
injuries,observedthatthemostcommonmechanisminthis typeofinjurywasfallingfromaheightgreaterthanordinary, aswellastrafficaccidents;JezekandDzupa,15inastudyon
themechanismofringfracture/injuryandtheageofpatients, reported that simplefractures (AO typeA)are common in elderly individualsand those consideredmoresevere (type C)arepredominantinyoungmales.Theauthorsalsopoint outthatthemostseriousfracturesarerelatedtohigh-energy traumas,withsignificantinvolvementofmotorcycleaccidents andfallsfromgreatheights.Baloghetal.17observedthatTile
typeBandCfracturesresultedfromhigh-energytraumawith apredominanceofaccidentswithcarsandmotorcycles.
accidentsandmotorcyclesitems1and2–mechanism)were noteworthy.Baloghet al.,17 inanepidemiologicalstudy on
pelvic ring injuries, compared the injuries caused by low-andhigh-energytrauma,havingalsoreportedamuchhigher andmoresevereincidenceofconcomitantinjuriesincasesof high-energytrauma.
We observed that the right side of the ring was the mostaffected,but noelements tojustifythis finding were found.Comparingthemechanismofinjurywithaffectedside (Table9),weobservedthatontherightside(item1)the mech-anismfallfromownheight(item3–mechanism)wasmore prevalent.Onthe leftside(item2) andonbothsides(item 3),car/truckandmotorcycle accidentmechanisms(items1 and2 –mechanism)stood out.Inthe casesofpubic sym-physisdiastasis(item4–affectedside),themainmechanism was horse accident (fallor trauma in the saddle – item 5 ofthe mechanism). Inrelation to these parameters, pubic symphysis diastasis was only associatedwith the mecha-nismof injury “direct trauma inthe saddle ofthe horse.” Itwasnotpossibletoassociateinjurysidewithmechanism oftrauma;furthermore,noreferencesintheliteraturewere retrieved.
Regarding the definitive treatment used, most of the present cases (63.6%) underwent non-surgical treatment. Gansslenetal.,3inastudyofpelvicringinjuries,alsoreported
ahighpercentageofcases(78%)treatednon-surgically.Inthe presentstudy,theauthorsbelievethatthehighpercentageof typeAfractures(54.5%)inthesampleinfluencedthisresult, sincethesearestableinjuriesandalmostallare treatedin anon-invasivemanner.Amongthecasessubmittedto surgi-caltreatment,theplate(pubicsymphisis/iliosacral)wasthe mostused materialinthe present study (isolated or asso-ciated),followed byiliosacralscrew(isolatedorassociated). DimitriouandGiannoudis24alsohighlightedtheuseofplate
inthe pubic symphysisassociated withiliosacral screwor iliosacralfixation with plates (anterioror posterior). These authorsalsocommentedontherecenttrendofincreaseduse ofpercutaneousfixationwithiliosacralscrewincasesofring injury.
Regardingthetypeoffixationusedinthepresentstudy, internal fixation was much more frequent (87.5%); exter-nalfixation(singleorassociated) accountedforonly12.5% of the cases. Chueire et al.,9 in their series of pelvic ring
injuries,presentedaslightlysmallerpercentageofpatients whounderwentsurgicaltreatment(29%)whencomparedwith the present study; however, the type offixation used was quitedifferent,asthoseauthorsusedexternalfixationin75% oftheir cases and internal fixation in25%. In the present study,iliosacralfixation(isolatedorassociated)wasused.The authors believethat thereis atrend ofgreater use ofthis methodinthisservice,sinceitisconsideredefficientinthe reductionandstabilizationoftheiliosacraljoint,aswell as lessinvasive.Tosounidisetal.,25assessingdatafromGerman
centersoftreatmentofpelvicringinjuries,alsoreportedan increasetendencyofiliosacralscrewuseinthetreatmentof thistypeoftrauma.Strobl etal.,26inarecentstudyonthe
treatmentofunstableinjuriesoftheposteriorregionofthe pelvicring,reportedthatinmanycenterstheiliosacralscrew isalreadyestablishedasthemostusedtreatmentinposterior fixationofthering.Inturn,TrikhaandGupta27reporttheuse
ofiliosacralscrewinpelvicinjuries,butalsorecommend tran-siliacplatesintheposteriorregionofthering.Mulleretal.,28
inastudyonunstableringinjuries(typeC)recommenda com-bination oftypesofsyntheses,i.e.,anterior internalfixator (subcutaneous)andposteriorstabilization(iliosacralscrewor spinopelvicandiliolumbarsupport);theseauthorsremarked uponthewidevarietyoftechnicaloptionsforfixationinring injuries.Itwasobservedthatalthoughthereisatendencyin theliteratureforlessinvasiveinternalfixations,avarietyof ringosteosynthesismaterialsarestilladvocated.
Inrelationtomortalityinpelvicringinjuries,the litera-turepresents indexeswithwide variation,andthe authors always emphasizethe association oftheserates with con-comitantinjuriesandtheseverityoftheringinjuryitself.1,29,30
Inthepresent study,thisassociation wasalsoobserved,as thecasesofdeathwereringinjuriestypesBorCwithsevere associated injuries. Gansslenet al.,3 inan epidemiological
study on this typeof injury, reported an overall mortality rateof13.4%,butindicatedthatthisratewasdirectly asso-ciated with extrapelvic trauma. Mortality observed in the literature17,21,22,29,30 ranges from 2% to 46%, and the
per-centageisalways dependentonseverity ofthe ring injury, on whether trauma was ofhigh energy, and on the pres-ence ofassociated injuries.Pohlemann et al.,29 in astudy
onpredictors ofmortalityinringinjuries,commentedthat in recent years the rate stillremains high when consider-ingonlycasesofcomplexinjuriesofthering,butwhenall typesofringfractures/injuriesareincluded,ageneraltrend towarda decreaseinthe mortalityrateisobserved(5%,in thesecases).Thefactisattributedtotheinclusionofless seri-ousinjuriesandimprovedtreatmentbothinthepre-hospital phaseandintheemergencycare.Chueireetal.,9intheirstudy
ofpelvicring fractures,reported a7%mortalityrate; these authorsalsohighlightedthesignificantrelationshipwiththis extrapelvic trauma. Richard and Tornetta,19 in a study on
serious injuriesofthepelvicring,reportedamortalityrate of6.8%.
Theauthorsconsideredthatthemostimportantfactorin thelowmortalityrateobservedinthepresentstudy(3%)was thehighnumber oftypeAcases,whichareusually associ-ated withlow-energy traumas and donot haveassociated injuriesorcomplications.Furthermore,thesmallpercentage ofseveretypeCinjuries(16.6%)alsoinfluencedthisrate,as theseareduetomuchmoreseveretrauma.Theauthors high-lightthatthetwocasesofdeathinthepresentstudywere unstable injuries and had serious and multipleassociated lesions.Inadditiontothesefactors,itisalsonoteworthythat inrecentyearstherehasbeenanimprovementintheoverall careforpolytraumapatientsinthisservice,aswellasgreater trainingandexperienceoftheorthopedicstaff,bothin emer-gencyproceduresandinthedefinitivetreatmentofpelvicring injuries; the authors believethat these elementsalso con-tributed to the low mortality rate observed inthe present work.
Conclusions
- Theyaremorefrequentinmales.
- In general, mostcommon mechanism ofinjury istraffic accident.
- In theelderly,the mostcommon mechanismofinjuryis low-energytrauma(fallfromownheight),thereisa preva-lence ofthe female sex,and the mostcommonplace of injuryisathome/institution.
- Inadolescents/youngadults,themostcommonmechanism ofinjury ishigh-energytrauma(traffic accident)andthe mostcommonplaceofinjuryistheurbanareaandhighway. - Ingeneral,typeAfracturesarethemostfrequent,followed
bytypesBandC.
- TypeAfracturesarethemostcommonintheelderlyand typeC,inadolescents/youngadults.
- Most injuries do not need emergency intervention and, whennecessary,orthopedicinterventionsarethemost fre-quent.
- Emergency interventionsareassociatedwithhigh-energy trauma.
- Amongassociatedinjuries,fractures/dislocationsinother sitesarethemostcommonandareassociatedwith high-energytrauma.
- Non-surgical treatment is the most common; in cases treatedsurgically,externalfixationisthemostusedmethod. - Deaths occur inunstable fractures andsevere associated
injuries.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. PizanisA,PohlemannT,BurkhardtM,AghayevE,HolsteinJH. Emergencystabilizationofthepelvicring:clinical
comparisonbetweenthreedifferenttechniques.Injury. 2013;44(12):1760–4.
2. ParreiraJG,CoimbraR,RasslanS,OliveiraA,FregonezeM, MercadanteM.Theroleofassociatedinjuriesonoutcomeof blunttraumapatientssustainingpelvicfractures.Injury. 2000;31(9):677–82.
3. GänsslenA,PohlemannT,PaulCh,LobenhofferPh,Tscherne H.Epidemiologyofpelvicringinjuries.Injury.1996;27Suppl 1.S-A13-20.
4. KrappingerD,KammerlanderC,DavidJH,BlauthM. Low-energyosteoporoticpelvicfractures.ArchOrthop TraumaSurg.2010;130(9):1167–75.
5. ZwingmannJ,HauschildO,BodeG,SüdkampNP,SchmalH. Malpositionandrevisionratesofdifferentimagingfor percutaneousiliosacralscrewfixationfollowingpelvic fractures:asystematicreviewandmeta-analysis.Arch OrthopTraumaSurg.2013;133(9):1257–65.
6. VaidyaR,ColenR,VigdorchikJ.Treatmentofunstablepelvic ringinjurieswithaninternalanteriorfixatorandposterior fixation:initialclinicalseries.JOrthopTrauma.2012;26(1): 1–8.
7. ColePA,GaugerEM,AnavianJ,ThuanV,MorganRA, HeddingsAA.Anteriorpelvicexternalfixatorversus subcutaneousinternalfixatorinthetreatmentofanterior ringpelvicfractures.JOrthopTrauma.2012;26(5): 269–77.
8.JoshuaRL,BurgessAR,LiporaceFA,HaidukewychGJ.Pelvic fractures:Part2.Contemporaryindicationsandtechniques fordefinitivesurgicalmanagement.JAmAcadOrthopSurg. 2013;21(8):458–68.
9.ChueireAG,FilhoGC,SantosAF,PocketKP.Fraturasdoanel pélvico:estudoepidemiológico.ActaOrtopBras.
2004;12(1):1–10.
10.FreitasCD,GarottiJER,NietoJ,GuimarãesRP,OnoNK,Honda E,etal.Houvemudanc¸asnaincidênciaenaepidemiologia dasfraturasdoanelpélviconasúltimasdécadas?RevBras Ortop.2013;48(6):475–81.
11.DevarinosN,EllantiP,MorrisS,McElwainJP.Epidemiologyof pelvicandacetabulartraumainaDublintertiaryhospital:a 10-yearexperience.IrJMedSci.2012;181(2):243–6.
12.TileM.Pelvicringfractures:shouldtheybefixed.JBoneJoint SurgBr.1988;70(1):1–12.
13.GoodmanLA.Onsimultaneousconfidenceintervalsfor multinominalproportions.Technometrics.1965;7:247–54.
14.KobbeP,HockertzI,SelleiRM,ReilmannH,HockertzT. Minimallyinvasivestabilizationofposteriorpelvicring instabilitieswithatransiliaclockedcompressionplate.Int Orthop.2012;36(1):159–64.
15.JezekM,DzupaV.Theinfluenceofpatientageand mechanismofinjuryonthetypeofpelvicfracture: epidemiologicalstudy.ActaChirOrthopTraumatolCech. 2012;79(1):65–8.
16.AlnaibM,WatersS,ShanshalY,CaplanN,JonesS,GibsonA, etal.Combinedpubicramiandsacralosteoporoticfractures: aprospectivestudy.JOrthopTraumatol.2012;13(2):
97–103.
17.BaloghZ,KingKL,MackayP,McDougallD,MackenzieS,Evans JA,etal.Theepidemiologyofpelvicringfractures:a
population-basedstudy.Injury.2007;63(5):1066–73.
18.GrotzMRW,AllamiMK,HarwoodPapeHC,KrettekC, GiannoudisPV.Openpelvicfractures:epidemiology,current conceptsofmanagementandoutcome.Injury.
2005;36(1):1–13.
19.RicardMJ,TornettaP.EmergentmanagementofAPC-2pelvic ringinjurieswithananteriorlyplacedC-clamp.JOrthop Trauma.2009;23(5):322–6.
20.SagiHC,MilatanoU,CaronT,LindvallE.Acomprehensive analysiswithminimum1-yearfollow-upofvertically unstabletransforaminalsacralfracturestreatedwith triangularosteosynthesis.JOrthopTrauma.2009;23(5): 313–21.
21.AbrassartS,SternR,PeterR.Unstablepelvicringinjurywith hemodynamicinstability:whatseemsthebestprocedure choiceandsequenceintheinitialmanagement?Orthop TraumatolSurgRes.2013;99(2):175–82.
22.BrunJ,GuillotS,BouzatP,BrouxC,ThonyF,GentyC,etal. Detectingactivepelvicarterialhemorrhageonadmission followingseriouspelvicfractureinmultipletraumapatients. Injury.2013;45(1):101–6.
23.LoonPV,SebastianK,HoffmannA,HessmannMH,Rommens PM.Radiologicalanalysisoperativemanagementand functionaloutcomeofopenbookpelviclesions:a13-year cohortstudy.Injury.2011;42(10):1012–49.
24.DimitriouR,GiannoudisPV.Pelvicfractures.Surgery. 2012;30(7):339–46.
25.TosounidisG,HolsteinJH,CulemanU,HolmenschlagerF, StubyF,PohlemannT.Changesinepidemiologyand
treatmentofpelvicfracturesinGermany:ananalysisondata ofGermanpelvicmulticenterstudygroupsIandIII(DGU/AO). ActaChirOrthoTraumatolCech.2010;77(6):450–6.
26.StroblFF,HaeusslerSM,PaprottkaPM,HoffmannRT,PieskeO, ReiserMF,etal.Technicalandclinicaloutcomeof
27.TrikhaV,GuptaH.Currentmanagementofpelvicfractures.J ClinOrthopTrauma.2011;2(1):12–8.
28.MüllerFJ,StosiekW,ZelinerM,NeugebauerR,FüchtmeierB. Theanteriorsubcutaneousinternalfixator(ASIF)forinstable pelvicringfractures.Clinicalandradiologicalmid-term results.IntOrthop.2013;37(11):2239–45.
29.PohlemannT,StengelD,TosoundisG,ReilmannH,StubyF, StöchleU,etal.Survivaltrendsandpredictorsofmortalityin
severepelvictrauma:estimatesfromtheGermanpelvic traumaregistryinitiative.Injury.2011;42(10):997–1002.