SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Safety
zone
for
posterosuperior
shoulder
access:
study
on
cadavers
夽
Miguel
Pereira
Costa,
Sandro
Baraldi
Moreira,
Gustavo
Costalonga
Drumond
∗,
Fernanda
de
Marchi
Bosi
Porto,
Fabiano
Rebouc¸as
Ribeiro,
Antonio
Carlos
Tenor
Junior
HospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received21May2014 Accepted30June2014 Availableonline8June2016
Keywords:
Shoulder/anatomyandhistology Shoulder/innervation
Acromioclavicularjoint/surgery Operativesurgicalprocedures
a
b
s
t
r
a
c
t
Objective:Theposterosuperiorshoulderaccessusedinsurgicaltreatmentfor acromioclavic-ulardislocationwasconstructedthroughdissectionof20shouldersfrom10recentlychilled adultcadavers,andthedistancesfromthisroutetothenearbyneurovascularstructures wereanalyzed.
Methods:AKirschnerwirewasintroducedintothetopofthebaseofthecoracoidprocess throughtheposterosuperiorshoulderaccess,intheareaoftheoriginoftheconoidand trapezoidligaments,thusreproducingthepathforinsertingtwoanchorsforanatomical reconstructionofthecoracoclavicularligaments.Thesmallestdistancefromtheinsertion pointoftheKirschnerwiretothesuprascapularnerveandartery/veinwasmeasured. Results:Themeandistancefromthesuprascapularnervetotheoriginofthe coracoclavicu-larligamentsatthetopofthebaseofthecoracoidprocesswas18.10mm(range:13.77–22.80) intherightshoulderand18.19mm(range:12.59–23.75)intheleftshoulder.Themean dis-tancefromthesuprascapularartery/veintotheoriginofthecoracoclavicularligaments was13.10mm(range:9.28–15.44)intherightshoulderand14.11mm(range:8.83–18.89)in theleftshoulder.Comparisonbetweenthecontralateralsidesdidnotshowanystatistical difference.
Conclusion: Theposterosuperiorshoulderaccessrouteforanatomicalreconstructionofthe coracoclavicularligamentsintreatingacromioclaviculardislocationshouldbeperformed respectingtheminimumlimitof8.83mmmedially.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheHospitaldoServidorPúblicoEstadualdeSãoPaulo,Servic¸odeOrtopediaeTraumatologia,GrupodeOmbroe Cotovelo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](G.C.Drumond). http://dx.doi.org/10.1016/j.rboe.2016.06.001
450
rev bras ortop.2016;51(4):449–453Zona
de
seguranc¸a
no
acesso
posterossuperior
do
ombro:
estudo
em
cadáver
Palavras-chave:
Ombro/anatomiaehistologia Ombro/inervac¸ão
Articulac¸ão
acromioclavicular/cirurgia Procedimentoscirúrgicos operatórios
r
e
s
u
m
o
Objetivo: Osautores fizeramoacessoposterossuperiordoombrousadonotratamento cirúrgicodaluxac¸ãoacromioclavicular,apartirdadissecc¸ãode20ombrosde10cadáveres adultosrecém-resfriados,eanalisaramasdistânciasdaviaàsestruturasneurovasculares próximas.
Métodos: Introduziu-seumfiodeKirschnernotopodabasedoprocessocoracoidepelo acessoposterossuperiordoombro,naáreadeorigemdosligamentosconoideetrapezoide, parareproduzirotrajetodainserc¸ãodeduasâncorasparareconstruc¸ãoanatômicados ligamentoscoracoclaviculares.Mediu-seamenordistânciadopontodeinserc¸ãodofiode Kirschneraonervoeàartéria/veiasupraescapular.
Resultados: Amédiadadistânciadonervosupraescapularatéaorigemdosligamentos coracoclavicularesnotopodabasedoprocessocoracoidefoide18,10mm(13,77a22,80) noombrodireitoe18,19mm(12,59a23,75)noombroesquerdo.Amédiadadistânciada artéria/veiasupraescapularatéaorigemdosligamentoscoracoclavicularesfoide13,10mm (09,28a15,44)noombrodireitoe14,11mm(08,83a18,89)noombroesquerdo.Nãohouve diferenc¸aestatísticacomparativaentreosladoscontralaterais.
Conclusão: Aviadeacessoposterossuperiordoombroparareconstruc¸ãoanatômicados ligamentoscoracoclavicularesnotratamentodasluxac¸õesacromioclavicularesdeveser feitacomrespeitoaolimitede08,83mmmedialmente.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Acromioclaviculardislocationisacommoninjuryin ortho-pedicpractice.1 Themostcommon mechanismofinjury is falling on the adductedshoulder, with force being applied directlytotheacromion.2Thisinjuryoccursmorefrequently amongyoungindividualsandisassociatedwithimpactsports andhighspeedvehiclesaccidents.3,4Rockwood,apudLemos2 andMouhsineetal.,5classifiedacromioclaviculardislocations insix types: typesI and II, considered as mild, with
non-operativetreatment;typesIV,V,andVI,severe,withsurgical
treatment6;andtypeIII,moderate,whichhascontroversial
treatment,dependentonfactorssuchasage,sportsactivity, anddeformity.
There are over 75 described techniques for the surgi-cal treatment of acromioclavicular dislocations, but none is considered to be the gold standard.7 The techniques includethe following: acromioclavicularjoint fixation with wire or plate8,9; coracoacromial ligament transfer10; cora-coacromial interval fixation with screw; use of anchors at the topofthe baseofthe coracoidprocess or subcoracoid suture loop11,12; and tendon reconstruction with autograft fromthecoracoclavicularandacromioclavicularligaments.13 The modifications of the techniques that secure the clav-icle to the coracoid process range from the use of screws (orsubcoracoid loops) tothe use ofanchorsand materials suchastheEndobuttonTM (flip-buttonTM).Thesetechniques
canbedone throughopen,minimallyinvasive,14 or arthro-scopicsurgery.15,16 Theadvantageinthe use ofanchors is itsplacement closertotheanatomical insertionsiteofthe coracoclavicularligaments.17
Theposterosuperiorshoulderapproachforthetreatment ofacromioclaviculardislocationswas presentedduringthe 34th Brazilian Congress of Orthopedics and Traumatology (2002) and received the Professor Orlando Pinto de Souza Award forCreativity.Developedbythe ShoulderandElbow Groupofourdepartment,thisapproachaimstofacilitatethe accesstothetopofthebaseofthecoracoidprocess;more anatomicallyreducetheacromioclavicularjoint;andpreserve theanteriorportionofthedeltoidmuscle,allowingforabetter functionalrecoveryoftheshoulder.
Thisstudyaimedtoreproducetheposterosuperior shoul-der access for the surgical treatment of acromioclavicular dislocationsincadaversandtoevaluatetheriskof neurovas-cularinjury.
Methods
Thestudydissected20shouldersin10recently-chilledadult cadavers(threewomenandsevenmen),meanageof61years (43–79),withnocongenitalabnormalities,signsoftrauma,or previoussurgeryontheshoulder.Dataonheight,gender,and agewerecollected.Thesamegroupofresearcherswas respon-sible foralldissections. Apilotstudy (usingtwoshoulders fromtwocadavers)wasmadeinadvancebeforethestartof datacollection,forbetterunderstandingandassessmentof thelocalanatomy.
Fig.1–Markingofboneprotusionsofthedistalclavicle,the coracoidprocess,theacromioclavicularjoint,theacromion, thescapularspine,andposterosuperiorshoulderapproach.
and for marking the posterosuperior shoulder approach (Fig.1).
Then,theskinincisionwasmadeandthesuperficialplane was dissected, exposing the deltotrapezial fascia. The fas-ciawasdetachedfromthedistalclavicleandscapularspine, makingitpossibletoexposethedeepplane,comprisingthe supraspinatusmusclebellyinferiorly,theacromioclavicular jointlaterally,andthetopofthebaseofthecoracoidprocess anteriorly.Followingtheexposureofthisareaandgood visi-bilityofthebaseofthecoracoidprocess,thecoracoclavicular andacromioclavicularligamentsaswellastheclaviclecould beidentifiedanddetached.Withtheclaviclestillreducedto theacromion,aKirschnerwirewasintroducedintothetopof thebaseofthecoracoidprocess,posteriorlytotheclavicle,to simulatetheintroductionofanchorsintheinsertionspotof thecoracoclavicularligaments(Fig.2).
After anterior dislocation of the distal clavicle, dissec-tioncontinuedfromthebaseofthecoracoidprocesstothe scapularnotch,identifyingthesuprascapularartery/vein,the suprascapularligamentandthesuprascapularnerve(Fig.3). Thestructuresweremarkedwithcoloredmarkersandthe dis-tancesfromthemtotheKirschnerwireweremeasured.The measurementsweremadewithaKingtools®150mmdigital caliper.
Foreachshoulder,twomeasuresweremadeandrecorded (Table1).Thefirstcorrespondedtothesmallestdistancefrom theKirschnerwiretothesuprascapularnerveandthesecond, tothedistancefromthewiretothesuprascapularartery/vein. StatisticalanalysiswasperformedusingthepairedWilcoxon test.Thesignificancelevelwassetat5%,andSASsoftware, version9.2,wasused.
Fig.2–Markingofthedistalthirdoftheclavicle.Pink marker:suprascapularnerve;bluemarker:trapezoid ligament;purplemarker:bordersoftheacromioclavicular joint.Thepincerindicatesthedirectionandtheinsertionof theKirschnerwireintothecoracoidprocess.
Results
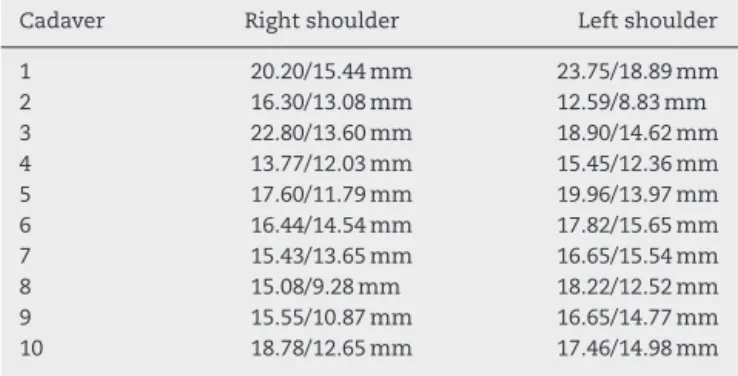
ThemeandistancefromtheKirschnerwiretothe suprascapu-larnervewas18.10mmintherightshoulderand18.19mmin theleftshoulder.ThemeandistancefromtheKirschnerwire tothe suprascapularartery/veinwas13.10mminthe right shoulderand14.11mmintheleftshoulder(Table1).
In all dissected shoulders, no anatomic variationswere observedregardingthelocationandrouteofthe neurovascu-larstructuresrelativetothesuperiortransverseligamentof
Fig.3–Markingofshouldersuperolateralstructureswith theclavicleposteriorlydislocated.Pinkmarker:
452
rev bras ortop.2016;51(4):449–453Table1–ShortestdistancefromtheKirschnerwireto thesuprascapularnerve(firstvalue)andthedistance fromtheKirschnerwiretothesuprascapularartery/vein (secondvalue).
Cadaver Rightshoulder Leftshoulder
1 20.20/15.44mm 23.75/18.89mm
2 16.30/13.08mm 12.59/8.83mm
3 22.80/13.60mm 18.90/14.62mm
4 13.77/12.03mm 15.45/12.36mm
5 17.60/11.79mm 19.96/13.97mm
6 16.44/14.54mm 17.82/15.65mm
7 15.43/13.65mm 16.65/15.54mm
8 15.08/9.28mm 18.22/12.52mm
9 15.55/10.87mm 16.65/14.77mm
10 18.78/12.65mm 17.46/14.98mm
MeasurestakenwithaKingtools®150mmdigitalcaliper.
thescapula:thesuprascapularnervewasundertheligament andthesuprascapularartery/vein,aboveit.
Discussion
Theneurovascularstructuresclosesttotheshoulder postero-superiorapproachandtotheintroductionofanchorsatthe topofthebaseofthecoracoidprocesswerethesuprascapular nerveandthesuprascapularartery/vein.Thesuprascapular nerve arises from the upper trunk ofthe brachial plexus, passesunderneaththeomohyoidmuscletowardthesuperior notchofthescapula,andthenunderthesuperiortransverse scapular ligament, which connects its two bone edges. At thislevel,itsendsnervemotorbranchestothe supraspina-tusmuscleandfollowstowardthespinoglenoidnotch,where itinnervatestheinfraspinatusmuscle.18
Thesuprascapulararteryoriginatesfrom the thyrocervi-caltrunk,abranchofthesubclavianarteryintheneck,and passesbehindtheclavicletosupplythemusclesofthe pos-terioraspectofthescapula.Thesuprascapulararteryfollows thesuprascapularnerve,butseparatesfromitnearthe supe-riortransverseligamentofthescapulaandpassesabovethe ligament.Itanastomosestothedorsalscapularand circum-flexscapulararteries,formingacollateralcirculationaround thescapula.Therefore,thesuperiortransverseligamentofthe scapulaseparatesthearterysuprascapularfromthe supras-capularnerve.18
Thegoal ofthe surgical treatment of acromioclavicular dislocationis to obtain anatomical reductionto allowsoft tissuehealingandrecoveryofpriorjointfunction. Biomechan-icalstudieshavedemonstratedthattheconoidandtrapezoid ligamentsareimportantstaticstabilizersofthe acromioclav-icularjoint.Theyhavealsoindicatedthat,amongthedifferent reconstruction techniques of these ligaments, anatomical reconstructionhasbiomechanicalpropertiessuperiortothose ofnon-anatomictechniques.19–25Thefixationoftheclavicle tothecoracoidprocesswithsutureanchorshasfacilitatedthe surgicaltechnique.However,theanteriorapproachrequires dissectionoftheanteriorportionofthedeltoidmuscleand maintainsresidualsubluxationoftheclavicle,asitdoesnot restoretheforcevectorofthecoracoclavicularligaments.The shoulderposterosuperiorapproachprovidesadirectaccessto
thetopofthebaseofthecoracoidprocessnotdamagingthe anteriordeltoidmuscle,andcanmaintainthejointreduction moreanatomically,restoringjointstabilitybypositioningthe anchorsintheanatomicallocationofthetorncoracoclavicular ligaments.
Molinetal.26presented84casesofpatientstreatedwith the posterosuperior shoulder approach for placement of sutureanchorsatthebaseofthecoracoidprocess.The tech-niquewasshowntobeeasytolearnandreproduce,yielding resultssimilartothetechniquesdescribedintheliterature, withalowrateofpostoperativecomplications.
DieterKohnet al.14reproducedincadaversaminimally invasiveendoscopictechniquefortheanatomical reconstruc-tionofcoracoclavicularligamentsandanalyzedthepotential riskofneurovascularinjury.Theanchorswerecorrectly pos-itionedatthecenterofthebaseofthecoracoidprocessand thesutureforcevectornearedtheanatomicalposition.The meandistancefromthecoracoidprocesstothe suprascapu-larnervewas1.8cm(1.5–2.2),andfromthecoracoidprocessto thesuprascapulararterywas1.5cm(1.3–1.9).However,those authorsdidnotcomparetothecontralateralside.
In the present study,the mean distancefrom the cora-coid process to the suprascapular nerve reached 1.81cm (1.37–2.28)intherightshoulderand1.81cm(1.25–2.37)inthe leftshoulder.Fromthecoracoidprocesstothesuprascapular artery/vein,themeandistancereached1.31cm(0.92–1.54)in therightshoulderand1.41cm(0.83–1.88)ontheleft shoul-der.Nosignificantdifferencesfromthelefttotherightsides wereobserved.Noneofthetwentyshouldersdissected pre-senteddamagetoneurovascularstructuresandsupraspinatus musclewiththeintroductionoftheKirschnerwire.
Conclusion
Itcanbeconcludedthattheinsertionofanchorsatthebase ofthecoracoidprocessthroughtheposterosuperiorshoulder approach foranatomical reconstruction ofcoracoclavicular ligamentsinthetreatmentofacromioclaviculardislocations shouldrespectthelimitof8.83mm,medially.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BannisterGC,WallaceWA,StableforthPG,HutsonMA.The managementofacuteacromioclaviculardislocation.A randomisedprospectivecontrolledtrial.JBoneJointSurgBr. 1989;71(5):848–50.
2.LemosMJ.Theevaluationandtreatmentoftheinjured cromioclavicularjointinathletes.AmJSportsMed. 1998;26(1):137–44.
3.BishopJY,KaedingC.Treatmentoftheacutetraumatic acromioclavicularseparation.SportsMedArthrosc. 2006;14(4):237–45.
4.MazzoccaAD,ArcieroRA,BicosJ.Evaluationandtreatmentof acromioclavicularjointinjuries.AmJSportsMed.
5. MouhsineE,GarofaloR,CrevoisierX,FarronA.GradeIandII acromioclaviculardislocations:resultsofconservative treatment.JShoulderElbowSurg.2003;12(6):599–602. 6. NissenCW,ChatterjeeA.TypeIIIacromioclavicular
separation:resultsofarecentsurveyonitsmanagement.Am JOrthop(BelleMeadNJ).2007;36(2):89–93.
7. JohansenJA,GrutterPW,McFarlandEG,PetersenSA. Acromioclavicularjointinjuries:indicationsfortreatment andtreatmentoptions.JShoulderElbowSurg.2011;20Suppl. 2:S70–82.
8. PhemisterPB.Thetreatmentofdislocationofthe
acromioclavicularjointbyopenreductionandthreadedwire fixation.JBoneJointSurg.1942;24:166–8.
9. SimE,SchwarzN,HöckerK,BerzlanovichA.Repairof completeacromioclavicularseparationsusingthe acromioclavicular-hookplate.ClinOrthopRelatRes. 1995;(314):134–42.
10.WeaverJK,DunnHK.Treatmentofacromioclavicularinjuries, especiallycompleteacromioclavicularseparation.JBoneJoint SurgAm.1972;54(6):1187–94.
11.BosworthBM.Acromioclavicularseparation:newmethodof repair.SurgGynecolObstet.1941;73:866–71.
12.BreslowMJ,JazrawiLM,BernsteinAD,KummerFJ,RokitoAS. Treatmentofacromioclavicularjointseparation:sutureor sutureanchors?JShoulderElbowSurg.2002;11(3):225–9. 13.CarofinoBC,MazzoccaAD.Theanatomiccoracoclavicular
ligamentreconstruction:surgicaltechniqueandindications.J ShoulderElbowSurg.2010;19Suppl.2:37–46.
14.OstiM,SeilR,BachelierF,KohnD.Minimallyinvasive endoscopicreconstructiontechniqueofacuteAC-joint dislocations:acadaverstudy.KneeSurgSportsTraumatol Arthrosc.2006;14:686–91.
15.SimoniM,BrandãoBL,TumoloLH.Tratamentodaluxac¸ão acromioclavicularcomamarrilhoscoracoclavicularespor meiodeduasmini-incisões.RevBrasOrtop.2005;40(8):483–9. 16.VieiraLAG,ViscoA,FernandesLFD,CorderoNGG.Tratamento
artroscópicodaluxac¸ãoacromioclavicularpelométodoTight Rope(Arthrex®).RevBrasOrtop.2009;44(1):52–6.
17.WellmannM,ZantopT,WeimannA,RaschkeMJ,PetersenW. Biomechanicalevaluationofminimallyinvasiverepairsfor completecromioclavicularjointdislocation.AmJSportsMed. 2007;35(6):955–61.
18.CaetanoEB.Basesanatômicasefuncionaisdascirurgiasdo membrosuperior.RiodeJaneiro:Medbook;2010.
19.CosticRS,LabriolaJE,RodoskyMW,DebskiRE.Biomechanical rationalefordevelopmentofanatomicalreconstructionsof coracoclavicularligamentsaftercompleteacromioclavicular jointdislocations.AmJSportsMed.2004;32(8):1929–36. 20.DebskiRE,ParsonsIM4th,WooSL,FuFH.Effectofcapsular
injuryonacromioclavicularjointmechanics.JBoneJointSurg Am.2001;83-A(9):1344–51.
21.FukudaK,CraigEV,AnKN,CofieldRH,ChaoEY. Biomechanicalstudyoftheligamentoussystemofthe acromioclavicularjoint.JBoneJointSurgAm. 1986;68(3):434–40.
22.GrutterPW,PetersenSA.Anatomicalacromioclavicular ligamentreconstruction:abiomechanicalcomparisonof reconstructivetechniquesoftheacromioclavicularjoint.Am JSportsMed.2005;33(11):1723–8.
23.LeeKW,DebskiRE,ChenCH,WooSL,FuFH.Functional evaluationoftheligamentsattheacromioclavicularjoint duringanteroposteriorandsuperoinferiortranslation.AmJ SportsMed.1997;25(6):858–62.
24.MazzoccaAD,ConwayJ,JohnsonS,RiosC,DumonskiM, SantangeloS,etal.Theanatomiccoracoclavicularligament reconstruction.OperTechSportsMed.2004;12(1):56–61. 25.ThomasK,LitskyA,JonesG,BishopJY.Biomechanical
comparisonofcoracoclavicularreconstructivetechniques. AmJSportsMed.2011;39(4):804–10.