w w w . r b o . o r g . b r
Original
Article
Overdiagnosing
of
femoroacetabular
impingement:
correlation
between
clinical
presentation
and
computed
tomography
in
symptomatic
patients
夽
Richard
Prazeres
Canella
a,∗,
Guilherme
Pradi
Adam
b,
Roberto
André
Ulhôa
de
Castillo
c,
Daniel
Codonho
a,
Gerson
Gandhi
Ganev
d,
Luiz
Fernando
de
Vicenzi
aaImperialHospitaldeCaridade,Florianópolis,SC,Brazil
bClínicaImagem,Florianópolis,SC,Brazil
cHospitalGovernorCelsoRamos,Florianópolis,SC,Brazil
dCentrodePesquisasOncológicas(CEPON),Florianópolis,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24March2015 Accepted12May2015
Availableonline16February2016
Keywords:
Hip
Femoroacetabularimpingement X-raycomputedtomography
a
b
s
t
r
a
c
t
Objective:Tocorrelatetheanglesbetweentheacetabulumandtheproximalfemurin symp-tomaticpatientswithfemoroacetabularimpingement(FAI),usingcomputedtomography (CT).
Methods:Weretrospectivelyevaluated103hipsfrom103patients,usingmultisliceCTto measuretheacetabularage,acetabularversion(initssupraequatorialportionandinits middlethird),femoralneckversion,cervical-diaphysealandalphaanglesandtheacetabular depth.Forthestatisticalanalysis,weusedthePearsoncorrelationcoefficient.
Results:Therewereinversecorrelationsbetweenthefollowingangles:(1)acetabular cov-erageversusalphaangle(p=0.019);(2)acetabularversion(supraequatorial)versusalpha angle(p=0.049).Forpatientswithfemoralanteversionlowerthan15degrees:(1)acetabular version(supraequatorial)versusalphaangle(p=0.026);(2)acetabularversion(middlethird) versusalphaangle(p=0.02).Forpatientswithacetabularversion(supraequatorial)lower than10degrees:(1)acetabularversion(supraequatorial)versusalphaangle(p=0.004);(2) acetabularversion(middlethird)versusalphaangle(p=0.009).
Conclusion:Therewasastatisticallysignificantinversecorrelationbetweentheacetabular versionandalphaangles(thesmallertheacetabularanteversionanglewas,thelargerthe alphaanglewas)insymptomaticpatients,thussupportingthehypothesisthatFAIoccurs whencamandpincerfindingsduetoacetabularretroversionareseensimultaneously,and thatthelatteralonedoesnotcauseFAI,whichleadstooverdiagnosisinthesecases.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedintheImperialHospitaldeCaridade,Florianópolis,SC,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.P.Canella).
http://dx.doi.org/10.1016/j.rboe.2016.02.001
Sobrediagnóstico
do
impacto
femoroacetabular:
correlac¸ão
entre
a
clínica
e
a
tomografia
computadorizada
em
pacientes
sintomáticos
Palavras-chave:
Quadril
Impactofemoroacetabular Tomografiacomputadorizada porraiosX
r
e
s
u
m
o
Objetivo:Correlacionar,portomografiacomputadorizada(TC),osângulosentreoacetábulo eofêmurproximalempacientessintomáticoscomimpactofemoroacetabular(IFA).
Métodos: Avaliamos,retrospectivamente,103quadris(103pacientes)emedimosporTC
multisliceosângulosdecoberturaacetabular,deversãoacetabular(emsuaporc¸ão suprae-quatoriale noseu terc¸omédio),de versãodocolofemoral,cervicodiafisário,alfae de profundidadeacetabular.Paraanáliseestatística,usamosocoeficientedecorrelac¸ãode Pearson.
Resultados:Houvecorrelac¸ãoinversaentreosângulos:1)coberturaacetabularversusângulo alfa(p=0,019);2)versãoacetabular(supraequatorial) versusânguloalfa(p=0,049).Para pacientescomanteversãofemoralmenordoque15◦:1)versãoacetabular(supraequatorial) versusânguloalfa(p=0,026);2)versãoacetabular(terc¸omédio)versusânguloalfa(p=0,02). Parapacientescomversãoacetabular(supraequatorial)menordoque10◦:1)versão
acetab-ular(supraequatorial)versusânguloalfa(p=0,004);2)versãoacetabular(terc¸omédio)versus
ânguloalfa(p=0,009).
Conclusão: Hácorrelac¸ãoinversaestatisticamentesignificativaentreosângulosdeversão acetabulareoânguloalfa(quantomenoroângulodeanteversãoacetabular,maioroângulo alfafemoral)empacientessintomáticos.Issoreforc¸aahipótesedequeoIFAocorrequando hásimultaneamenteosachadosdecamepincerporretroversãoacetabularequeessenão causaoIFAisoladamente,oquelevaasobrediagnósticonessescasos.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Recentadvancesinunderstandingtheanatomyand biome-chanicsofthecoxofemoraljointhaveshownthat morpholog-icalalterationstothehiporactivitieswithexcessiverange ofmotionthatleadtorepetitivecontactbetweenthefemoral neckandtheacetabularrimmayleadtoaprogressive degen-erativeprocessandearlyosteoarthrosisofthehip.1
Reinhold Ganz2,3 was the main author responsible for
describingfemoroacetabularimpingement(FAI)anditstwo subtypes:camandpincer.Cam-likeimpingementiscausedby aboneprominenceatthecervicocapitaljunction,whichleads tolossofthenormalsphericityofthefemoralhead. Pincer-likeimpingementiscausedbyexcessiveacetabularrooforby acetabularretroversion.AccordingtoBecketal.,4both
sub-typesarepresentin86%ofthepatientsdiagnosedwithFAI. Sofar,littleisknownaboutthecauseandnaturalhistory oftheseanatomicalalterations.5Itisunderstoodthatthere
isa dynamic interaction between the proximalfemur and theacetabulum,6,7whichbeginsattheembryonicstage8with
endochondralossificationregulatedbyintrauterinepressure andcontinuesuntiladulthood.Thejointremodelingdepends onthemechanicalstresstowhichthehipisexposed.9Thus,
variationsintheacetabularangle10,11and/ortheangleofthe
proximalfemur12,13wouldleadtoearlyjointdamage.
However,ithasrecentlybeensuggestedthatpincer-likeFAI isdiagnosedexcessively.14,15 Inastudyinwhichthe
angu-larrelationshipbetweentheacetabulumandproximalfemur wascorrelated amongasymptomaticpatients,thepresence ofposterior angling of the acetabulum was thought to be
presentduetocompensationofthefemoralanatomyduring hipdevelopment.15Inananalysisonhipspresentingthecam
andpincertypes,itwasobservedthattherewasnosignificant differenceinacetabularversionincomparisonwithnormal hips.Thissuggeststhatacetabularretroversionwouldnotbe theonlycauseofFAI.14
Ourstudyhadtheaimofusingmultislicecomputed tomo-graphy(CT)tocorrelatetheanglesbetweentheacetabulum andtheproximalfemur,insymptomaticpatientswithFAI.
Methods
Ourstudywasanalyzedandapprovedbytheresearchethics committeeofourinstitution.Weselected103patientswho underwent multisliceCT ontheir hipsbetweenMarch and December2010,becauseofclinicalsuspicionof femoroacetab-ularimpingement.Allofthesepatientspresentedcomplaints ofpaininthehipjointandtestedpositiveforanteriorimpact inphysicalexaminationmaneuversat90degreesofflexion combinedwithadductionandinternalrotation.
Dataonthesepatients’acetabularandfemoralangleswere gatheredand subjectedtostatisticalanalysis.Noexclusion criteriawereused.Thepatients’meanagewas37years(range: 16–68);21weremenand82werewomen.
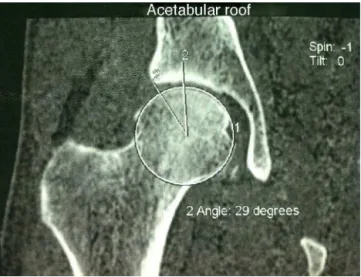
Fig.1–Tomographicmeasurementoftheacetabularroof angleusingChen’smethod.
ofgadotericacid.Followingthis,magneticresonance imag-ing(MRI) wasalsoperformed,using aGEInfinitymachine. AxialT1sequenceswithfatsaturationinthefemoralneck, sagittaland coronalsequencesofthickness0.3cm, coronal STIRsequencesofthickness0.5cmandaxialprotondensity sequenceswithfatsaturationwereproduced.Thefollowing angles were measured: acetabular roofangle using Chen’s method (Fig. 1); acetabular version angle in its cranial or supraequatorialportion(Fig.2)andinitsmiddlethird(Fig.3); alphaangleofthecervicocapitaljunctionofthefemur(Fig.4); cervicodiaphysealangle(Fig.5);acetabulardepth(Fig.6);and femoralneckversionangle(Fig.7).
Themeasurements were made on the multislice tomo-graphyimages,inanADW4.3workstation.Thealphaangle ofthecervicocapitaljunctionofthefemurwasevaluatedby meansofanoblique axialplanethat crossedthe centerof thefemoralneck,usingcoronalreformattingasthereference. Measurementsofthealphaangleandthemiddlethirdofthe acetabularversion werethenmadeonthe imageobtained, inaccordancewiththestudybyKamathetal.16However,we
Fig.2–Tomographicmeasurementoftheversionanglein thecranialorsupraequatorialportionoftheacetabulum.
Fig.3–Tomographicmeasurementoftheversionanglein themiddlethirdoftheacetabulum.
alsoincludedmeasurementsoftheangleofversionofthe cra-nialportionoftheacetabulum,becauseoftheimportanceof thislocationinthegenesisoftheimpactandfor differenti-ationoftheoverallretroversionoftheacetabulumfromthe retroversionofitscranialportionalone.
Tomeasuretheacetabularanteversion,imagesintheaxial planewereused,withcorrectionofpossiblepelvictilt,and linestangentialtotheanteriorandposteriorbordersofthe acetabulumweretracedoutatthelevelsofthecenterofthe femoral head and the top ofthe femoralhead. Theangle betweentheselinesandthesagittalplanewasmeasured.
To measure the acetabular roof angle, the technique describedbyChenetal.wasused.17Thisinvolvedusingan
image in the coronal plane that crossed the acetabula, in which the fundus ofthe acetabulum took on a“teardrop” appearance.Onthisimage,twolinesmeetingatthecenter ofthefemoralheadweretracedout:oneoriginatingatthe borderoftheacetabulumandtheotherparalleltotheaxial axisofthepelvis.
Fig.5–Tomographicmeasurementofthe cervicodiaphysealangle.
Theangleoffemoralneckversionwasmeasuredbymeans of3Dreconstructionofthefemur.Viewingfromabove,two linesweretracedout:onecrossingthecenterofthefemoral neckandtheother,tangentialtotheposteriorportionofthe femoralcondyles.Thecervicodiaphysealanglewasmeasured onthe3Dreconstructionusingananteriorview.Inamanner similartomeasurementsonradiographs,onelinewastraced outalongtheaxisofthefemoraldiaphysisandanotheralong theaxisofthefemoralneck,andtheanglebetweenthemwas measured.
Toanalyzethedataobtainedbymeansofdescriptive statis-tics,weusedPearson’scorrelationcoefficient,takingp<0.05 assignificant.
Results
Table1presentstheanalysisonallthepatientsstudied.From
this,astatisticallyinversecorrelation(p<0.05)wasobserved
Fig.6–Tomographicmeasurementoftheacetabulardepth.
Fig.7–Three-dimensionalreconstructionofthefemur, withsubtractionoftheremainderofthebonestructuresin ordertomeasurethefemoralneckversion.
through cross-correlatingthe values ofthe acetabularroof angle versus the alpha angle and angle of version of the cranialorsupraequatorialportionoftheacetabulumversus thealphaangle.Nostatisticalcorrelationwasobservedupon cross-correlatingtheremainingvalues.
InTable2,onlythepatientswithfemoralanteversionless
than 15 degrees were selected. Once again, a statistically significant inverse correlation (p<0.05) was observed upon cross-correlatingthevaluesoftheangleofversionofthe cra-nialorsupraequatorialportionoftheacetabulumversusthe alphaangle.Inthisevaluation,therewasalsoaninverse cross-correlationbetweentheangleofversionofthemiddlethird oftheacetabulumandthealphaangle.Theother numbers evaluateddidnotpresentstatisticalvalue.
InTable3,onlythepatientswithversionoflessthan10
degreesinthecranialorsupraequatorialportionofthe acetab-ulum were selected. In relationto Table 2, we observed a strongerstatisticallyinversecorrelation(p<0.005)upon cross-correlatingthevaluesoftheangleofversionofthecranialor supraequatorialportionoftheacetabulumversusthealpha angleandangleofversionofthemiddlethirdofthe acetabu-lumversusthealphaangle.Theothernumbersevaluateddid notpresentstatisticalvalue.
Fig.8showsthestatisticallysignificantinversecorrelation betweenthesupraequatorialacetabularversionandthealpha angleamongthepatientsselectedinTable3,ingraphform.In otherwords,thesmallertheangleofacetabularanteversion was,thelargerthefemoralalphaanglewas,insymptomatic patients.
Discussion
Moynihan et al.18 warned about the potential for
Table1–Statisticalanalysison103patients,inwhichn=numberofpatientsanalyzedandp<0.05suggestsstatistical significance.
Center-edge angle(Chen)
Acetabular depth
Cranial acetabular
version
Middle-third acetabular
version
Cervicodiaphyseal angle
Alphaangle Femoral versionangle
Center-edgeangle(Chen)
Pearson’scorrelation 1 −0.159 0.45 0.097 −0.046 −0.231 −0.029
p 0.109 0 0.328 0.646 0.019 0.775
n 103 103 103 103 103 103 103
Acetabulardepth
Pearson’scorrelation −0.159 1 −0.352 −0.377 0.274 0.14 0.025
p 0.109 0 0 0.005 0.159 0.8
n 103 103 103 103 103 103 103
Cranialacetabularversion
Pearson’scorrelation 0.45 −0.352 1 0.493 −0.103 −0.194 −0.001
p 0 0 0 0.302 0.049 0.989
n 103 103 103 103 103 103 103
Middle-thirdacetabularversion
Pearson’scorrelation 0.097 −0.377 0.493 1 0.06 −0.183 0.089
p 0.328 0 0 0.547 0.065 0.372
n 103 103 103 103 103 103 103
Cervicodiaphysealangle
Pearson’scorrelation −0.046 0.274 −0.103 0.06 1 0.099 −0.019
p 0.646 0.005 0.302 0.547 0.318 0.846
n 103 103 103 103 103 103 103
Alphaangle
Pearson’scorrelation −0.231 0.14 −0.194 −0.183 0.099 1 0.104
p 0.019 0.159 0.049 0.065 0.318 0.294
n 103 103 103 103 103 103 103
Femoralversionangle
Pearson’scorrelation −0.029 0.025 −0.001 0.089 −0.019 0.104 1
p 0.775 0.8 0.989 0.372 0.846 0.294
n 103 103 103 103 103 103 103
10.00
5.00
.00
–5.00
–10.00
–15.00
30.00 40.00 50.00 60.00 70.00 80.00
Alpha angle
Cranial acetabular angle
Observed
r=–0.477 p=0.004 n=35
Linear R2 Linear=0.228
Fig.8–Correlationbetweensupraequatorialacetabular versionandalphaangleintheselectedpatientsofTable3.
Thereisafundamentalaimtodiscriminatebetterbetween benign“abnormalities”andthosethatwillprogressandcause harm.Likeinthespine,thereishighprevalenceof “abnormal-ities”inthehipregion.MRImayshowalterationsthatarenot clinicallyimportant,thusalsoleadingtooverdiagnosis.19
Most cases of femoroacetabular impingement (FAI) are considered tobeprimary, i.e.ofunknowncause.Hipswith symptomaticFAIdifferfrom“normal”hipsduetoa combina-tionoffactorssuchasmorphology,vulnerabilityofthelabrum andcartilageanddemandsplacedonthehips,inrelationto activitylevelandrangeofmotion.19
Cam-like FAIisrecognizedas afactor thatcauses early osteoarthrosis ofthe hip,through injury tothe joint carti-lageandlabrum,whichleadstofunctionalincapacityinyoung adultpatientswithanactivelifestyle.20
Abnormalities at the head-neck junction in skeletally matureindividualshavebeencorrelatedwithhip osteoarthro-sis. This has been demonstrated in cases of proximal epiphyseal slippage of the femur and in cases of fractur-ingofthefemoralneckwithconsolidationpresentingslight rotationaldeformity.12,21 Theorigin ofthesemorphological
alterations remains unknown,19 but somestudies15,22 have
Table2–Statisticalanalysiswithselectionofthepatientswithfemoralanteversionoflessthan15degrees.
Center-edge angle(Chen)
Acetabular depth
Cranial acetabular
version
Middle-third acetabular
version
Cervicodiaphyseal angle
Alphaangle Femoral versionangle
Center-edgeangle(Chen)
Pearson’scorrelation 1 −0.187 0.333 0.067 0.054 −0.176 −0.212
p 0.219 0.025 0.661 0.727 0.248 0.161
n 45 45 45 45 45 45 45
Acetabulardepth
Pearson’scorrelation −0.187 1 −0.443 −0.409 0.164 0.238 0.017
p 0.219 0.002 0.005 0.282 0.116 0.911
n 45 45 45 45 45 45 45
Cranialacetabularversion
Pearson’scorrelation 0.333 −0.443 1 0.49 −0.003 −0.331 0.018
p 0.025 0.002 0.001 0.983 0.026 0.906
n 45 45 45 45 45 45 45
Middle-thirdacetabularversion
Pearson’scorrelation 0.067 −0.409 0.49 1 −0.003 −0.346 0.04
p 0.661 0.005 0.001 0.984 0.02 0.794
n 45 45 45 45 45 45 45
Cervicodiaphysealangle
Pearson’scorrelation 0.054 0.164 −0.003 −0.003 1 −0.009 −0.034
p 0.727 0.282 0.983 0.984 0.954 0.827
n 45 45 45 45 45 45 45
Alphaangle
Pearson’scorrelation −0.176 0.238 −0.331 −0.346 −0.009 1 0.002
p 0.248 0.116 0.026 0.02 0.954 0.992
n 45 45 45 45 45 45 45
Femoralversionangle
Pearson’scorrelation −0.212 0.017 0.018 0.04 −0.034 0.002 1
p 0.161 0.911 0.906 0.794 0.827 0.992
n 45 45 45 45 45 45 45
n,numberofpatientsanalyzed. p<0.05suggestsstatisticalsignificance.
Hogervorst21suggestedthatthesealterationsoccurredatthe
endofgrowth.
ComputedtomographyisusefulforevaluatingFAIbecause it enables measurement of angles with clear anatomical referencesandreducestheinterobserverdiscrepancies. Mea-surementoffemoralversionisdonemoreeasilyandprecisely throughtomographythanthroughconventionalradiography. Tomographyalsoenablescorrelationofpositioningerrors dur-ing thepost-processing. Another advantageoftomography isthe3Dreconstructionsthat canbemade,whichprovide detailedmodelsthatareveryusefulforpreoperativeplanning. Themainprobleminmakingevaluationsusingtomography isthefactthatpatientsareevaluatedinthedecubitus posi-tionandtheremaybechangestopelvictiltinrelationtothe uprightstandingposition.23,24
Inourstudy,wereproducedourdailypracticeregarding investigationofFAI.CTisrequestedandthefollowingare rou-tinelymeasured:acetabularroofangleusingChen’smethod; angleofversionofthecranialorsupraequatorialportionof theacetabulumandinthemiddlethird;alphaangleofthe cervicocapitaljunctionofthefemur;cervicodiaphysealangle; acetabulardepth;andangleofversionofthefemoralneck.
Buller et al.15 evaluated 230 hips of 115 asymptomatic
patientsbymeansof3Dreconstructionsoftware.Theangle ofversionofthefemoralneck,cervicodiaphysealangle,angle of version and inclination of the acetabulum and center-edgeangle were measured.They showedthat therewas a positivecorrelationbetweentheanglesoffemoraland acetab-ularversionandconcludedthatcompensationbetweenthe femurandacetabulumoccurredduringjointformation.The present study suggests that in some patients in whom it was believed thatpathological retroversion ofthe acetabu-lum(pinceraction)wasoccurring,theproximalfemurwould compensateforthis.Thesepatientswerethuswronglybeing diagnosedwithFAI.ThedifferencebetweenBuller’sstudyand oursisthatweevaluatedasymptomaticpopulation,i.e.all ofour patientshad undergoneexaminationdue toclinical suspicionofFAI.
Tönnis and Heinecke22 demonstrated the relationship
Table3–Statisticalanalysiswithselectionofthepatientswithversionofthecranialorsupraequatorialacetabulumof lessthan10degrees.
Center-edge angle(Chen)
Acetabular depth
Cranial acetabular
version
Middle-third acetabular
version
Cervicodiaphyseal angle
Alphaangle Femoral versionangle
Center-edgeangle(Chen)
Pearson’scorrelation 1 −0.236 0.25 0.14 0.043 −0.151 −0.334
p 0.172 0.148 0.423 0.807 0.387 0.05
n 35 35 35 35 35 35 35
Acetabulardepth
Pearson’scorrelation −0.236 1 −0.305 −0.266 0.146 0.227 0.051
p 0.172 0.074 0.122 0.402 0.189 0.769
n 35 35 35 35 35 35 35
Cranialacetabularversion
Pearson’scorrelation 0.25 −0.305 1 0.146 −0.043 −0.477 −0.175
p 0.148 0.074 0.402 0.807 0.004 0.314
n 35 35 35 35 35 35 35
Middle-thirdacetabularversion
Pearson’scorrelation 0.14 −0.266 0.146 1 0.038 −0.434 −0.007
p 0.423 0.122 0.402 0.828 0.009 0.967
n 35 35 35 35 35 35 35
Cervicodiaphysealangle
Pearson’scorrelation 0.043 0.146 −0.043 0.038 1 0.053 −0.135
p 0.807 0.402 0.807 0.828 0.764 0.439
n 35 35 35 35 35 35 35
Alphaangle
Pearson’scorrelation −0.151 0.227 −0.477 −0.434 0.053 1 0.045
p 0.387 0.189 0.004 0.009 0.764 0.799
n 35 35 35 35 35 35 35
Femoralversionangle
Pearson’scorrelation −0.334 0.051 −0.175 −0.007 −0.135 0.045 1
p 0.05 0.769 0.314 0.967 0.439 0.799
n 35 35 35 35 35 35 35
n,numberofpatientsanalyzed. p<0.05suggestsstatisticalsignificance.
acetabulum.Inaddition,theynotedthatnormalorincreased femoralanteversionwasgenerallycompensatedfor,through diminishedacetabularversion,andviceversa.
Neppleetal.25observedthatthegeneralprevalenceofcoxa
profundawas55%amonghipsinfourgroups(dysplastichips, hipswithresidualdeformitiesfromLegg-Calvé-Perthes dis-ease,hipswithFAIandasymptomatichips)and concluded thatcoxaprofundawasanonspecificradiologicalfindingand thatit couldbeconsideredtobeanormalfinding,atleast amongwomen.
In2008,Ganzetal.2questionedthenotionthatallpatients
with morphological abnormalities indicative of FAI would developarthrosisandcontraindicatedtreatmentfor asymp-tomatic patients. A study by Hartofilakidis et al.26 showed
thatmost(82.3%)ofthepatientswithradiological evidence ofFAI remained asymptomatic and freefrom osteoarthro-sisfor amean of18.5 years, and that the onlysignificant predictor ofosteoarthrosis was the presenceof idiopathic osteoarthrosisinthecontralateralhip.Thissuggeststhat sys-temicpathological factorsmay havegreaterinfluencethan minimalmorphologicalalterationsandwouldcontraindicate surgical treatment for asymptomatic patients with radio-graphicevidenceofFAI.
Arthroscopictreatmentofcam-likeimpacthasshowngood results, especiallyamongpatients placinghighdemandon thejoints.JavedandO’Donnell27evaluatedtheresultsfrom
treatingcam-likeFAIbymeansofarthroscopicfemoral osteo-chondroplasty in patients over the age of 60 years. They reportedahighsatisfactionrate(75%),withoutanycasesof complicationsandwithevaluationtototalhiparthroplastyin 17%ofthecases.
Intheorthopedicliterature,severaltreatmentsfor pincer-like FAI have been described, including periacetabular osteotomy1,2andrimtrimmingwithlabralrepair.28However,
therearenorandomizedprospectivestudieswith measure-ment of objective data, for example regarding the result from physiotherapeutic treatmentforpatientswith pincer-likeFAIalone.Thecamandpincercomponentsrarelyoccur separately,1,4butithasstillnotbeeninvestigatedwhetherit
isnecessarytodealwithcamandpincerdeformitiesinthe samehip,orjustononesideofthejoint.19
Siebenrock et al.24 warned that in hips with coxa
reconstructionfortreatingFAImight,inreality,betheresult fromconcomitantlydealingwithlabralorchondrallesions.29
ArthroscopictreatmentforthefemoralcomponentofFAI (cam),withfemoralosteochondroplastyandconsequent cor-rection of the alpha angle, followed by repair ofchondral andlabrallesions,hasshownexcellentclinicalresults.20We
believethatthis technique, whichisnotgreatly aggressive towardthe acetabularroof,could beindicatedforthe vast majorityofpatientswithrealindicationsfororthopedic sur-gicaltreatment.
Conclusion
Ourfindings,supportedbythepresenceofastatistically sig-nificantinverse correlationbetweentheangleofacetabular versionandthe alphaangleinsymptomaticpatients, rein-force the hypothesis that pincer action due to acetabular retroversionisnotthesolecauseofFAI,giventhatin asymp-tomaticindividuals,thereis acetabularretroversionthat is compensatedbythefemur.Insymptomaticpatients,this cor-relationisinverse,i.e.thesmallertheacetabularanteversion is,thelargerthealphaangleofthefemuris.
Thismayaidorthopedistsinmakingtherapeuticdecisions regardingthevariousclinical presentationsofFAIand also provideawarningtothemregardingtheexistenceof over-diagnosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. CrawfordJR,VillarRN.Currentconceptsinthemanagement
offemoroacetabularimpingement.JBoneJointSurgBr.
2005;87(11):1459–62.
2. GanzR,LeunigM,Leunig-GanzK,HarrisWH.Theetiologyof
osteoarthritisofthehip:anintegratedmechanicalconcept.
ClinOrthopRelatRes.2008;466(2):264–72.
3. GanzR,ParviziJ,BeckM,LeunigM,NötzliH,SiebenrockKA.
Femoroacetabularimpingement:acauseforosteoarthritisof
thehip.ClinOrthopRelatRes.2003;417:112–20.
4. BeckM,KalhorM,LeunigM,GanzR.Hipmorphology
influencesthepatternofdamagetotheacetabularcartilage:
femoroacetabularimpingementasacauseofearly
osteoarthritisofthehip.JBoneJointSurgBr.
2005;87(7):1012–8.
5. HavivB,BurgA,VelkesS,SalaiM,DudkiewiczI.Trendsin
femoroacetabularimpingementresearchover11years.
Orthopedics.2011;34(5):353.
6. BeaupreGS,OrrTE,CarterDR.Anapproachfor
time-dependentbonemodelingandremodeling:theoretical
development.JOrthopRes.1990;8(5):651–61.
7. McKibbinB.Anatomicalfactorsinthestabilityofthehipjoint
inthenewborn.JBoneJointSurgBr.1970;52(1):148–59.
8. CarterDR,OrrTE,FyhrieDP,SchurmanDJ.Influencesof
mechanicalstressonprenatalandpostnatalskeletal
development.ClinOrthopRelatRes.1987;(219):237–50.
9. CarterDR.Mechanicalloadinghistoryandskeletalbiology.J
Biochem.1987;20(11–12):1095–109.
10.DoraC,ZurbachJ,HerscheO,GanzR.Pathomorphologic
characteristicsofposttraumaticacetabulardysplasia.J
OrthopTrauma.2000;14(7):483–9.
11.ReynoldsD,LucasJ,KlaueK.Retroversionoftheacetabulum:
acauseofhippain.JBoneJointSurgBr.1999;81(2):281–8.
12.LeunigM,CasillasMM,HamletM,HerscheO,NötzliH,Slongo
T,etal.Slippedcapitalfemoralepiphysis:earlymechanical
damagetotheacetabularcartilagebyaprominentfemoral
metaphysis.ActaOrthopScand.2000;71(4):370–5.
13.ItoK,MinkaMA,LeunigM,WerlenS,GanzR.
Femoroacetabularimpingementandthecam-effect:a
MRI-basedquantitativeanatomicalstudyofthefemoral
head-neckoffset.JBoneJointSurgBr.2001;83(2):171–6.
14.CobbJ,LogishettyK,DavdaK,IranpourF.Camsandpincer
impingementaredistinct,notmixed:theacetabular
pathomorphologyoffemoroacetabularimpingement.Clin
OrthopRelatRes.2010;468(8):2143–51.
15.BullerLT,RosneckJ,MonacoFM,ButlerR,SmithT,Barsoum
WK.Relationshipbetweenproximalfemoralandacetabular
alignmentinnormalhipjointsusing3-dimensional
computedtomography.AmJSportsMed.2012;40(2):367–75.
16.KamathS,NarayanaswamyS.Computedtomography
assessmentofhipjointsinasymptomaticindividualsin
relationtofemoroacetabularimpingement.AmJSportsMed.
2010;38(8):NP1.
17.ChenL,BoonthathipM,CardosoF,CloptonP,ResnickD.
Acetabulumprotrusioandcenteredgeangle:new
MR-imagingmeasurementcriteria–acorrelativestudywith
measurementderivedfromconventionalradiography.
SkeletalRadiol.2009;38(2):123–9.
18.MoynihanR,DoustJ,HenryD.Preventingoverdiagnosis:how
tostopharmingthehealthy.BrMedJ.2012;344:19–23.
19.PollardTC.Aperspectiveonfemoroacetabularimpingement.
SkeletalRadiol.2011;40(7):815–8.
20.ByrdJW,JonesKS.Arthroscopicfemoroplastyinthe
managementofcam-typefemoroacetabularimpingement.
ClinOrthopRelatRes.2008;467(3):739–46.
21.HogervorstT,BoumaH,deBoerSF,deVosJ.Humanhip
impingementmorphology:anevolutionaryexplanation.J
BoneJointSurgBr.2011;93(6):769–76.
22.TönnisD,HeineckeA.Acetabularandfemoralanteversion.
Relationshipwithosteoarthritisofthehip.JBoneJointSurg
Am.1999;81(12):1747–70.
23.KonishiN.Thethree-dimensionalacetabularcoverageandits
positionalchangeduetochangeofpelvictilt.HipJoint.
1993;19:423–7.
24.SiebenrockKA,SchoenigerR,GanzR.Anterior
femoro-acetabularimpingementduetoacetabular
retroversion:treatmentwithperiacetabularosteotomy.JBone
JointSurgAm.2003;85(2):278–86.
25.NeppleJJ,LehmannCL,RossJR,SchoeneckerPL,ClohisyJC.
Coxaprofundaisnotausefulradiographicparameterfor
diagnosingpincer-typefemoroacetabularimpingement.J
BoneJointSurgAm.2013;95(5):417–23.
26.HartofilakidisG,BardakosNV,BabisGC,GeorgiadesG.An
examinationoftheassociationbetweendifferent
morphotypesoffemoroacetabularimpingementin
asymptomaticsubjectsandthedevelopmentofosteoarthritis
ofthehip.JBoneJointSurgBr.2011;93(5):580–6.
27.JavedA,O’DonnellJM.Arthroscopicfemoral
osteochondroplastyforcamfemoroacetabularimpingement
inpatientsover60yearsofage.JBoneJointSurgBr.
2011;93:326–31.
28.PhilipponMJ,SchenkerML.Anewmethodforacetabularrim
trimmingandlabralrepair.ClinSportsMed.2006;25(2):293–7.
29.PalmerWE.Femoroacetabularimpingement:cautionis
warrantedinmakingimaging-basedassumptionsand