www.jped.com.br
ORIGINAL
ARTICLE
Impact
of
malnutrition
on
cardiac
autonomic
modulation
in
children
夽
,
夽夽
Gláucia
Siqueira
Carvalho
Barreto
a,∗,
Franciele
Marques
Vanderlei
b,
Luiz
Carlos
Marques
Vanderlei
b,
Álvaro
Jorge
Madeiro
Leite
aaUniversidadeEstadualdoCeará(UECE),Fortaleza,CE,Brazil
bUniversidadeEstadualPaulista(UNESP),DepartamentodeFisioterapia,PresidentePrudente,SP,Brazil
Received24November2015;accepted2March2016 Availableonline25May2016
KEYWORDS
Autonomicnervous system;
Heartrate; Malnutrition;
Heartratevariability; Childhealth
Abstract
Objective: Tocomparetheautonomicbehaviorbetweenmalnourishedchildrenandacontrol groupusinganalysisofheartratevariability(HRV).
Method: Datawereanalyzedfrom70childrenwhoweredividedintotwogroups:malnourished andeutrophic,accordingtotheZ-scorenutritionalstatusforheightandage.Foranalysisof HRVindices,heart ratewas recordedbeattobeatwiththechildinthe supineposition for 20min.Theanalysisoftheseindiceswasperformedusinglinearmethods,analyzedinthetime andfrequencydomains. Student’st-testfor unpaireddataandtheMann---Whitneytestwere usedtocomparevariablesbetweengroups,withasignificancelevelof5%.
Results: Areductioninsystolicanddiastolicbloodpressureandanincreaseinheartratewere foundinmalnourishedchildrencomparedtoeutrophicchildren.TheHRVindicessuggestedthat malnourishedchildrenpresentreductionsinbothsympatheticandparasympatheticautonomic nervoussystemactivity.The SDNN,rMSSD,NN50,pNN50, SD1,SD2, TINN,LF(ms2),andHF
(ms2)indiceswerelowerinmalnourishedchildren.
Conclusion: Malnourishedchildrenpresentchangesincardiacautonomicmodulation, charac-terizedbyreductionsinbothsympatheticandparasympatheticactivity,aswellasincreased heartrateanddecreasedbloodpressure.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
夽
Pleasecitethisarticleas:BarretoGS,VanderleiFM,VanderleiLC,LeiteÁJ.Impactofmalnutritiononcardiacautonomicmodulationin children.JPediatr(RioJ).2016;92:638---44.
夽夽
Institutiontowhichthisworkislinked:UniversidadeEstadualdoCeará,Fortaleza,CE,Brazil.
∗Correspondingauthor.
E-mail:[email protected](G.S.Barreto).
http://dx.doi.org/10.1016/j.jped.2016.03.005
PALAVRAS-CHAVE
Sistemanervoso autônomo;
Frequênciacardíaca; Desnutric¸ão;
Variabilidadeda frequênciacardíaca; Saúdedacrianc¸a
Impactodadesnutric¸ãonamodulac¸ãoautonômicacardíacaemcrianc¸as
Resumo
Objetivo: avaliaramodulac¸ãoautonômicacardíacadecrianc¸asdesnutridaspormeioda vari-abilidadedafrequênciacardíaca(VFC).
Método: foramanalisadas70crianc¸ascommédiadeidadede3.71anos,queforam distribuí-dasem doisgrupos,deacordocomoestadonutricional: desnutridas eeutróficas,seguindo oescoreZ,paraestaturaeidade.ParaanálisedosíndicesdaVFC,afrequênciacardíacafoi captadabatimentoabatimentocomascrianc¸asemdecúbitodorsalpor20minutos.Aanálise dessesíndicesfoirealizadapormeiodemétodoslineares,analisadosnosdomíniosdotempo edafrequência.TestetdeStudentparadadosnãopareadosetestedeMann-Whitneyforam aplicadosparacompararasvariáveisentreosgrupos,comníveldesignificânciade5%. Resultados: Reduc¸ãodapressãoarterialsistólicaediastólicaeaumentonafrequênciacardíaca foramencontrados nascrianc¸as desnutridas quandocomparadaàseutróficas.Os índicesda VFC sugeremque crianc¸as desnutridas apresentamuma reduc¸ão damodulac¸ãosimpáticae parassimpáticadosistemanervosoautônomo.OsíndicesSDNN,rMSSD,NN50,pNN50,SD1,SD2, TINN,BFeAFemms2forammenoresnascrianc¸asdesnutridas.
Conclusão: crianc¸asdesnutridasapresentammodificac¸õesnamodulac¸ãoautonômicacardíaca caracterizadapordepressãonocomponentesimpáticoenoparassimpático,bemcomoaumento nafrequênciacardíacaediminuic¸ãodapressãoarterial.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Malnutritionisconsideredaseriouspublichealthproblem.1 Epidemiological data indicate that it affects about 15.5% of the population worldwide and a third of this is children.2 The consequences of malnutrition in children include, among others: problems in physical develop-ment, such as short height, reduced muscle mass, and a decline in bone calcification; effects on physiologi-cal conditions, providing an inefficient immune system; iron deficiency anemia and frequent bacterial prolifer-ation; and delayed mental development, with learning disabilities.3 Therefore, child malnutrition promotes per-manent damage to health and thus promotes high mortality.3
Furthermore, studies have shown that malnutrition produceschangesinthefunctionoftheautonomicnervous system inchildren.4 Thiscondition ofimbalance may rep-resent an important negative factor, since theautonomic functioncontrolssomeoftheinternalfunctionsofthebody and,accordingly,deservesattention.
One way to evaluate the behavior of the autonomic nervous system is heart rate variability (HRV), a simple andnon-invasivetoolaimedat thedetectionandstudyof cardiac autonomic dysfunction, either in physiological or pathologicalconditions.5
Studies that investigate autonomic modulationin child malnutrition are scarce. Only one study including chil-dren, which evaluated the modulation of the autonomic nervous system in malnutrition using HRV, was found in the literature.4 Sirivastava et al.4 compared the HRV of malnourished children with healthy children matched for sex and age. The authors found that the low frequency
(LF)index in normalizedunits and the LF/high frequency (HF) ratio presented an increase, whereas the HF index in normalized units presented a reduction in the group of malnourished children. In conclusion, the authors sug-gested that cardiac autonomic function characterized by increasedsympatheticmodulation occursin malnourished children.
Otherstudies6,7showincreasedsympatheticmodulation oftheautonomicnervoussystem inmalnutrition.Belchior etal.7analyzedtheeffectofproteinmalnutritioninratsand foundanincreaseinbloodpressure,however,alterationsin vascularreactivitywerenotfound,whereasSawayaetal.6 foundastrongassociationbetweenmalnutritionand hyper-tension.ThesestudiessuggestpossiblechangesinHRV.This correlationcouldbeconsideredanimportanttoolfor deter-miningprognosisandtheneedforspecialattentionandcare toward the autonomic nervous system and cardiovascular functioninmalnourishedchildren.
In thiscontext, understanding malnutrition,the causal factors,andtheconsequencesandrepercussions becomes important, reiterating its status as a public health prob-lem. Malnutrition appears to promote changes in cardiac autonomicbehavior;however, dataontheanalysisofthis behavior are scarce. Considering that growth affects the cardiovascular system8 and has a significant effect on the maturation of the autonomic nervous system and its representations in cardiac modulation,9 this scenario is problematic.
Methods
Population
To conduct this study data were analyzed from 70 chil-dren of both sexes, agedbetween 3 and5 years,divided intotwogroups:malnourishedandeutrophic.Malnourished childrenwereconsideredthosewithaZ-scoreoflessthan
−2 in relation to height for their age, according to the criteriaestablished for age and sexby the World Health Organization,10andeutrophicthosewithZ-scoreshigheror equalto−2andlessthan+3.10
Themalnourishedgroupwascomposedof35children,23 female(65.71%),whiletheeutrophicgroupwascomposedof 35children,20female(57.14%).Thesamplesizecalculation wasperformedconsideringasavariablethesquarerootof themeansquareddifferencesbetweenadjacentnormalRR intervalsinanintervaloftime(rMSSD)index.Themagnitude ofsignificantdifferenceassumedwas7.0ms,consideringa standarddeviationof10.12ms,basedonapilotstudy,with analphariskof5%andbetaof80%,thesamplesizeresulted in33childrenpergroup.
The exclusion criteriawere asfollows: use of medica-tionsthatcouldinfluenceautonomicactivityoftheheart, andthepresenceofinfectionsandknownmetabolicand/or cardiorespiratorydisorders,whichcouldaffectthecardiac autonomiccontrol.
The volunteers andtheir parents were informedabout theproceduresandobjectivesofthisstudy,andafter agree-ing, a parent/guardian signed the informed consent. All procedureswereapprovedby theCommitteeforEthicsin ResearchoftheStateUniversityofCeará(Protocol275.310).
Studydesign
Datacollectionwasperformedina roomwithan ambient temperaturebetween 21and23◦Cand humiditybetween 40%and 60%,in themorning toavoidcircadian variation. To reduce the child’s anxiety during collection, only the researcherandthepersonresponsibleforthechildremained intheroom.
Initially, personal informationonthe children was col-lected,such asname, age,sex, anddata ontheir health status. Following this, a physical examination was per-formedthatincludeddeterminationofweightandheightto calculatetheZ-scoreofheightfor age,andmeasurement ofbloodpressureandheartrate.
Weight and height were recorded using a mechanical anthropometricscale (Balmak®, SP, Brazil),with a
capac-ityof150kg. Heartratewasmeasured usinga heartrate monitor(PolarElectroOy® ---modelRS800CX,Finland)and
blood pressure indirectlyusing a stethoscope (Littmann®,
Lightweight II SE, Littmann, USA) and an aneroid infant sphygmomanometerwithanarmdiameterrangeoffrom10 to18cm (Premium®, China)onthe leftarm of the child,
inaccordancewithcriteriaestablished bytheVIBrazilian HypertensionGuidelines.11Toavoiderrorsinthe determina-tionofbloodpressurevalues,asingleevaluatorperformed themeasurementsforthisparameterthroughoutthe exper-iment.
Aftertheseprocedures,theelectrode ofcapture strap wasmoistenedwithwaterandthenwasplacedonthechild’s chest,overtheregionoftheprecordium,andtheheartrate monitorinhis/herfist;thisequipmenthadbeenpreviously validated for capture of heart rate beat to beat and the subsequent useof datafor analysis ofHRV.12 After place-ment of the strap and monitor, the child was positioned in theFowlersupine positionat30◦ andremained atrest
for20minbreathingspontaneously.Followingthiscollection periodthechildwasreleased.
AnalysisofHRV
ForHRVanalysis,heartratewasrecordedbeattobeat dur-ingtheentireprotocolwithasamplingrateof1000Hz.For dataanalysis,1000consecutiveRRintervalswereusedafter digitalfilteringinthesoftwarePolarPrecisionPerformance SW(Polar®,version4.01.029,USA),complementedby
man-ual elimination of prematureectopic beatsand artifacts. Onlyserieswithmorethan95% sinusbeatswereincluded inthestudy.5Theabsenceofectopicbeatsorartifactsthat couldinterfereintheanalysisofHRVwasverifiedthrough visualanalysisofthetimeseries.
HRVanalysiswasperformedusinglinearmethods, ana-lyzingthe timeandfrequency domains,and bygeometric methods. In the time domain the following indices were used: rMSSD, SDNN (standard deviation of all normal RR intervals),pNN50(percentageofadjacentRRintervalswith difference of duration longer than 50ms), and the RR intervals.5
In the frequency domain, the spectral components of LF and HF in milliseconds squared (ms2) and in normal-izedunits,andtherelationshipbetweenthem(LF/HF)were used.Thefrequencybandsusedforeachcomponentwere: LF=0.04---0.15HzandHF=0.15---0.40Hz.5Thespectral anal-ysis was calculated using a Fast Fourier Transform.5 The normalization of the spectral analysis data was used to minimize theeffects ofchanges inthe VLFband andwas determinedfromthedivisionofpowerratingagiven com-ponent(LForHF)bythetotalpowerspectrum,minusthe verylowfrequencycomponentandmultipliedby100.5
ForHRVanalysisthroughgeometricalmethods,the fol-lowing indices wereused:triangular (calculated fromthe constructionofadensityhistogramofnormalRRintervals, whichshowedthelengthofRRintervalsonthehorizontal axis(x),andthefrequencywithwhicheachoccurredonthe verticalaxis(y),TINN(totalnumberofRRintervalsusedto constructthehistogram divided bythemodal frequency), andtheindicesobtainedfromthePoincaréplot(SD1 [dis-persionofpointsperpendiculartothelineofidentitywhich appearstobeanindexofinstantaneousrecordingof beat-to-beatvariability],SD2[dispersionofthepointsalongthe lineofidentity,representingHRVinlong-termregister]and SD1/SD2ratio[ratiobetweenshortandlongvariationsofRR intervals]).5 AllHRVindiceswereobtainedthroughKubios HRV,version2.0software(Kubiossoftware,Finland).5
Statisticalanalysis
asmean,standarddeviation,median,minimum,maximum, andpercentagevalues.
Forcomparison ofgroups, initially,data normalitywas determined(Shapiro---Wilktest),andwhenthenormal dis-tributionwasaccepted,Student’st-testfor unpaireddata wasapplied.Insituationswherethenormaldistributionwas notaccepted,theMann---Whitneytestwasapplied. Differ-encesinthesetestswereconsideredstatisticallysignificant whenthep-valuewaslessthan0.05.
Results
The anthropometric characteristics, Z-score, and cardio-vascular parameters of the study groups can be seen in Table 1. There was no statistically significant differ-ence between groups with respect to age (p=0.057). However, lower values of the following variables were observed: weight, height, Z-score, and systolic(SBP) and diastolic (DBP) blood pressure for malnourished children,
whereas the heart rate values were higher in these children.
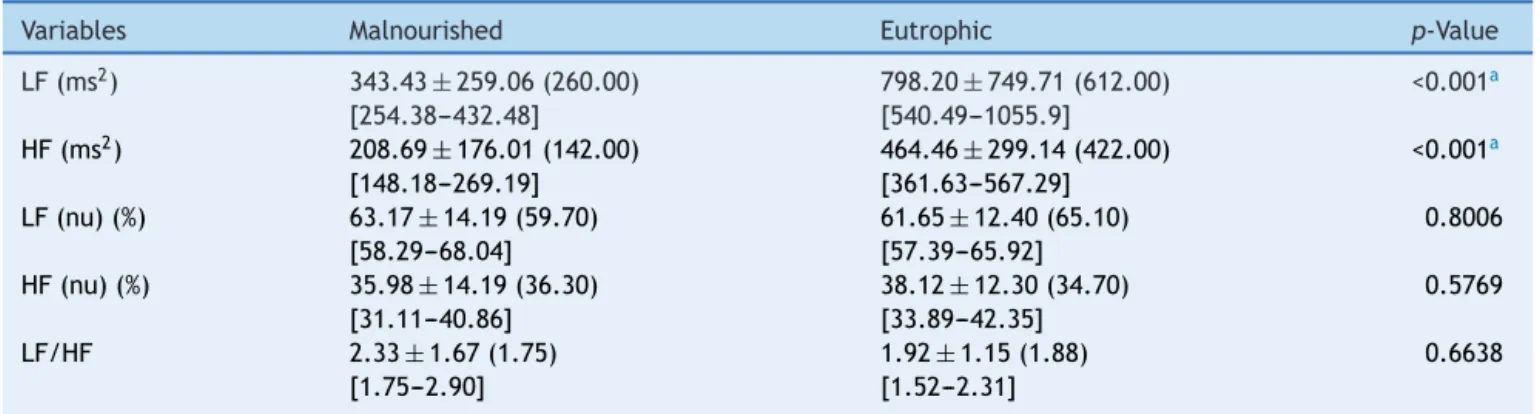
Table2presentsthevaluesobtainedfortheLFandHF indices,innormalizedunitsandms2,andtheLF/HFratioof themalnourishedandeutrophicgroups.Thestudyrevealed significantlylowervaluesforthemalnourishedgroup com-paredwiththeeutrophicgroupfortheLFandHFindicesin ms2,whereasthevaluesof LFandHFin normalizedunits andtheLF/HFratioshowedthattherewerenostatistically significantdifferenceswhencomparingthetwogroups.
Table 3 shows the values of the HRV indices obtained in the time domain. Statistically significant differences betweengroupswereobservedfortheRRintervalandthe SDNN,rMSSD,NN50,andpNN50indices,withlowervalues forthemalnourishedgroup.
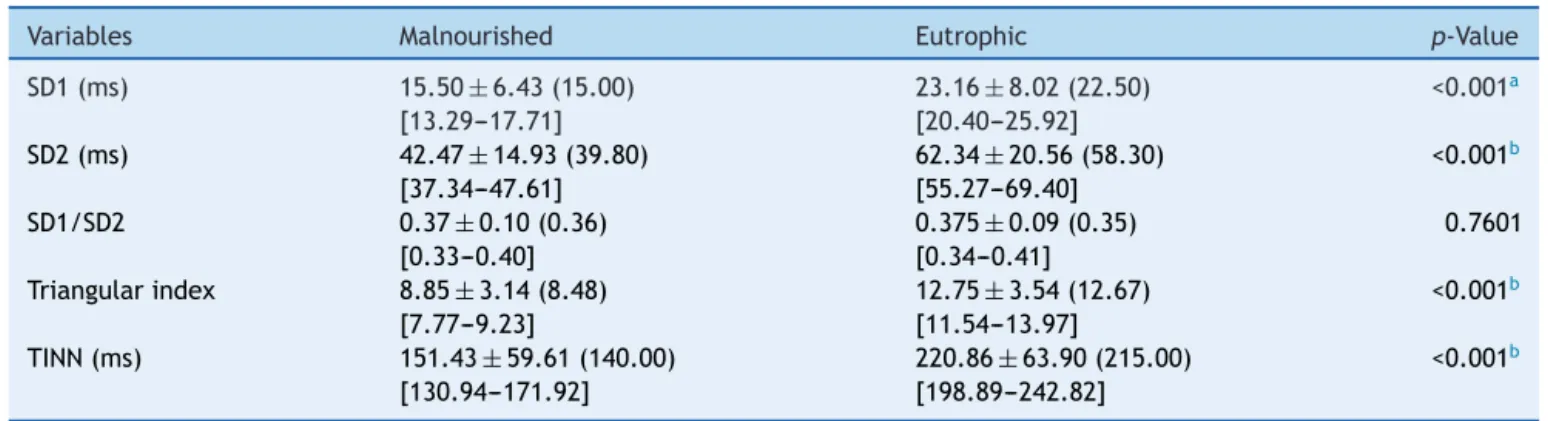
ThevaluesofSD1,SD2,SD1/SD2ratio,triangularindex, andTINNcanbeseeninTable4.Significantreductionswere observedinSD1,SD2,thetriangularindex,andtheTINNin themalnourishedgroup.FortheSD1/SD2ratio,therewas nodifferencebetweengroups.
Table1 Meanvaluesfollowedbystandarddeviations,medians,and95%confidenceintervalsfortheanthropometricvariables, Z-score,andcardiovascularparametersoftheanalyzedgroups.
Variables Malnourished Eutrophic p-Value
Age(years) 3.71±0.75(4.00) [3.46to3.97]
4.09±0.85(4.00) [3.79to4.38]
0.057
Weight(kg) 13.02±1.71(12.90) [12.43to13.61]
17.89±3.04(17.50) [16.85to18.94]
<0.001a
Height(cm) 91.53±5.47(91.00) [89.65to93.41]
106.83±8.15(108.00) [104.03to109.63]
<0.001a
Z-score −2.80±0.588(−2.79) [−3.00to−2.60]
0.191±1.28(0.00) [−0.25to0.63]
<0.001a
SBP(mmHg) 102.14±6.56(100.00) [99.89to104.40]
107.14±8.60(110.00) [104.19to110.10]
0.008a
DBP(mmHg) 63.43±6.84(60.00) [61.08to65.78]
68.00±8.68(70.00) [65.02to70.98]
0.0256b
HR(bpm) 113.46±14.132(111.00) [108.60to118.32]
104.66±10.55(105.00) [101.03to108.28]
0.0054b
bpm,beatsperminute;SBP,systolicbloodpressure;DBP,diastolicbloodpressure;HR,heartrate.
a Significantdifferencebetweenthemalnourishedgroupandtheeutrophicgroup(Student’st-testforunpaireddata). b Significantdifferencebetweenthemalnourishedgroupandtheeutrophicgroup(Mann---Whitney).
Table2 Meanvaluesfollowedbystandarddeviations,medians,and95%confidenceintervalsforLF(ms2),HF(ms2),LF(nu),
HF(nu),andtheLF/HFratioobtainedinmalnourishedandeutrophicchildren.
Variables Malnourished Eutrophic p-Value
LF(ms2) 343.43±259.06(260.00)
[254.38---432.48]
798.20±749.71(612.00) [540.49---1055.9]
<0.001a
HF(ms2) 208.69±176.01(142.00) [148.18---269.19]
464.46±299.14(422.00) [361.63---567.29]
<0.001a
LF(nu)(%) 63.17±14.19(59.70) [58.29---68.04]
61.65±12.40(65.10) [57.39---65.92]
0.8006
HF(nu)(%) 35.98±14.19(36.30) [31.11---40.86]
38.12±12.30(34.70) [33.89---42.35]
0.5769
LF/HF 2.33±1.67(1.75) [1.75---2.90]
1.92±1.15(1.88) [1.52---2.31]
0.6638
LF,lowfrequency;HF,highfrequency;nu,normalizedunits;LF/HF,relationshipbetweenlowandhighfrequency.
Table3 Meanvaluesfollowedbystandarddeviations,medians,and95%confidenceintervalsfortheRRinterval,SDNN,rMSSD, NN50,andpNN50obtainedfrommalnourishedandeutrophicchildren.
Variables Malnourished Eutrophic p-Value
RRinterval(ms) 537.59±49.92(521.50) [520.43---554.75]
591.20±57.56(577.60) [571.41---610.98]
0.0001a
SDNN(ms) 32.09±11.16(29.90) [28.25---35.92]
47.16±15.22(44.90) [41.93---52.39]
<0.001a
rMSSD(ms) 21.54±9.48(21.20) [18.28---24.79]
32.75±11.35(31.90) [28.85---36.66]
<0.001b
NN50(ms) 53.91±65.94(31.00) [31.25---76.58]
140.46±109.92(118.00) [102.67---178.24]
0.0001a
pNN50(%) 5.35±6.62(3.10) [3.08---7.63]
13.88±10.72(11.80) [10.20---17.56]
0.0001a
SDNN,standarddeviationfrom themeanofallnormal RRintervals;rMSSD,square rootofthemean squareddifferencesbetween adjacentnormalRRintervals;NN50,numberofsuccessiveRRintervalswhichdifferbymorethan50ms;pNN50,percentageofpairsof consecutiveRRintervalswhosedifferenceisgreaterorequalto50ms.
aSignificantdifferencebetweengroups(Mann---Whitney).
b Significantdifferencebetweengroups(Student’st-testforunpaireddata).
Table4 Meanvaluesfollowedbystandarddeviations,medians,and95%confidenceintervalsfor SD1,SD2,SD1/SD2ratio, triangularindex,andTINNobtainedfrommalnourishedandeutrophicchildren.
Variables Malnourished Eutrophic p-Value
SD1(ms) 15.50±6.43(15.00) [13.29---17.71]
23.16±8.02(22.50) [20.40---25.92]
<0.001a
SD2(ms) 42.47±14.93(39.80) [37.34---47.61]
62.34±20.56(58.30) [55.27---69.40]
<0.001b
SD1/SD2 0.37±0.10(0.36) [0.33---0.40]
0.375±0.09(0.35) [0.34---0.41]
0.7601
Triangularindex 8.85±3.14(8.48) [7.77---9.23]
12.75±3.54(12.67) [11.54---13.97]
<0.001b
TINN(ms) 151.43±59.61(140.00) [130.94---171.92]
220.86±63.90(215.00) [198.89---242.82]
<0.001b
SD1,standarddeviationoftheinstantaneousvariabilityofbeat-to-beat;SD2,standarddeviationoflong-termcontinuousRRintervals; TINN,triangularinterpolationofRRintervals.
aSignificantdifferencebetweengroups(Student’st-testforunpaireddata). b Significantdifferencebetweengroups(Mann---Whitney).
Discussion
Theresults obtainedby meansof theHRV indicessuggest thatmalnourishedchildrenhavereductionsinboth sympa-thetic and parasympathetic modulation of the autonomic nervoussystem.Furthermore,decreasesinSBPandDBPand anincreaseinheartratewerealsoobservedinmalnourished children.
TheanalysisoftheRRintervalwassignificantlylowerin themalnourishedgroup,thus indicatingincreasesinheart rate. Corroborating the findings of this study, Sirivastava etal.4 studied 35 children (mean age: 6.06
±2.04 years) withmildtomoderatelevelsofmalnutritionandfoundthat thevaluesof RRintervals werereducedin thesechildren comparedwithchildrenconsideredhealthy.
Inthepresentstudy,bothSBPandDBPpresentedreduced valuesinthemalnourishedgroup.Incontrasttothefindings of the present study, Sesso et al.13 conducted a cross-sectional study with172 children over 2 years of age; of these,91wereclassifiedasmalnourishedwithaZ-scoreof
−1in relation to heightand weightfor their age. Of the groupofmalnourishedchildren,29%showedanincreasein SBPandDBPafteradjustmentforage,sex,andheightwhen comparedwith thecontrol children(2%). In addition,the averageDBPpresentedasignificantincreaseinthe malnour-ishedchildren(65.2±0.6mmHg)inrelationtothegroupof healthychildren(61.8±0.8mmHg).
There are several mechanisms reported in the litera-turethatexplaintherelationship betweenmalnutritionin earlylifeandincreasedbloodpressure,suchasactivationof thereninangiotensin14;changesinstructure,function,and vascularlength15;increasedmodulationofthesympathetic autonomicnervoussystem16;increasedinsulinsensitivity17; andhighglucocorticoidplasmaconcentrations.18Thus, mal-nutritionduringchildhoodmayrepresentariskfactorthat shouldbetakenintoconsiderationfor thedevelopmentof hypertensioninthefuture.13
theirbodymassissmaller,19afactthatmayalsoberelated tothe reduced blood pressure valuesobtained, since the childrenwhobelongedtothemalnourishedgroupwereaged between 3and 5 years.As the malnourishedchild grows, bloodpressureincreasesprogressively,asdemonstratedby otherauthors.13,16,18
In relation to heart rate, the findings indicate that the group of malnourished children showed higher val-ues compared to the control group (113.46bpm±14.13 [111.0] vs. 104.66±10.55 [105.0], respectively). Accord-ingCattermole etal.,20 normalchildren at 4yearsofage mustpresentmedianvaluesofheartrateofapproximately 95.4bpm, with a confidence interval between 74.3 and 124.9bpm. Therefore, for both groups studied the heart rate values were within the normal range for that age, and thus the statistically significant difference observed betweenthegroupsapparentlydoesnotindicateanyclinical implications.
In the present study the rMSSD, SD1, pNN50, NN50, and HF (ms2), which reflect parasympathetic modulation of theautonomic nervoussystem,5 showed areductionin themalnourishedgroupcomparedtotheeutrophicgroup, suggestingthatinthesechildrentheparasympathetic mod-ulationisreduced.Srivastavaetal.4didnotobservechanges intherMSSDandpNN50indicesinchildrenwithmildto mod-erate malnutrition; however, the authors concluded that malnutritionmayberelatedtodecreasedvagalmodulation. Furthermore, a decrease in parasympathetic modulation wasalsoobservedinotherconditionsofnutritionaldeficit, such as vitamin D deficiency,21 protein restriction,22 and bulimianervosa.23
Itis noteworthythatreducedvagalmodulationis asso-ciated withan increased risk for morbidity and mortality fromallcauses anddevelopmentofvariousrisk factors24; therefore, the results of this study reinforce the impor-tance of early intervention in malnourished children to prevent damage to cardiovascular and metabolic health, and thus promote a better cardiac autonomic modu-lation response and attenuate possible damage to the body.
The SDNN,SD2,TINN,andtriangularindex,which rep-resent the overall variability, i.e., both sympathetic and parasympathetic modulation, andthe LF index(ms2) that points to the sympathetic modulation,5 as well as the indicespreviouslymentioned,showedadecreaseinthe mal-nourishedgroup comparedtothe eutrophicgroup. Unlike the observations in the present study, the authors found increasedsympatheticmodulationinmalnourishedchildren, characterizedbyelevatedvaluesintheLFindexin normal-izedunitsandtheLF/HFratio.4
Several possible mechanisms have been proposed in attemptstoexplaintheobservedchangesinthesympathetic nervoussystem. Malnutrition during thecritical periodof developmentcanleadtoautonomicimbalancethrough mor-phologicalchangesinseveralareasof thecentralnervous systeminvolvedinthegenerationand/ormodulationof sym-patheticactivity,suchasthehypothalamus.25Moreover,one canalsoobservechangesinthereleaseofneurotransmitters inthecentralnervoussystem.26
Studieshaveshown thatthesympatheticcomponentof theautonomicnervoussystemisassociatedwiththe mobi-lization of energy and participates in the control of the
glucosemetabolismandfat.24,27Perterson etal.28 demon-strated a relationship between increased body fat and hypoactivityofthesympatheticandparasympathetic com-ponentsoftheautonomicnervoussystem;inaddition,the authorsfoundthatlowersympatheticmodulationis associ-atedwithlowerenergyexpenditure.
The reduction in sympathetic modulation in malnour-ishedchildren indicates an importantclinical condition in ordertosaveenergyandconsequently,promoteapossible positiveenergy balance.Vanderlei etal.29 described that inobesechildrenthereisadecreaseinthissystem,which results in an imbalance between supply and consumption andculminatesinbodyweightgain.Therefore,itis hypothe-sizedthatthereductioninsympatheticmodulationobserved inmalnourishedchildrenfavorstheenergybalanceandmay reducetheeffectsofmalnutrition.
TheLFandHFindicesinnormalizedunitsshowedno dif-ferencesinthemalnourishedgroupcomparedtothecontrol. Theseresultswereexpected,sinceadecreaseintheir val-uesinmalnourishedchildrenwasobservedwhenanalyzed inms2.ConsideringthattheLFandHFindicesinnormalized unitsarecalculatedfromthe areaof thepowerspectrum and a reduction in the spectrum occurs in malnourished children, changes in the values calculated in normalized units were not observed. Moreover, the decrease in both thesympatheticcomponentandtheparasympathetic com-ponent of the autonomic nervous system justifies the absenceofsignificantdifferencesintheSD1/SD2andLF/HF ratios of malnourished children compared to the control group.
Conceptually,malnutritioncanbedefinedasthe relation-shipbetweenthereductioninweightandheightassociated withadeficiencyofessentialvitaminsandminerals.4 Sev-eral studies have shown that micronutrient deficiency is correlatedwithchangesinHRV.Singhetal.30 related vita-minDandvitaminEdeficiencywithmodificationsinHRVand Mannetal.21associatedvitaminDwithchangesinautonomic modulationinhumans.Thus,itcanalsobeinferredthatthe reductioninnutrientsinmalnourishedchildrenshouldbea factortobetakenintoaccounttoexplainthealterationsin cardiacautonomicmodulation.
As a limitation of this study, the lack of stratifica-tion of the degree of malnutrition in the children can be cited, which could further enrich the discussion of the study. Furthermore, the respiratory rate values were not collected, which could have contributed to a better understanding of the spectral analysis of HRV. However the analysis of autonomic modulation in malnourished children through HRV proved to be an effective method for quick and easy application and, therefore, consider-ing that the tool was able to reflect important aspects of the autonomic nervous system, the importance of its inclusionasaroutinemeasureofcontrolandanalysisof car-diac modulation of these children should beemphasized, as well as in effective interventions to eradicate infant malnutrition.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Monteiro CA, Conde WL, Konno SC. Análise do inquérito ChamadaNutricional2005realizadopeloMinistériodo Desen-volvimento Social eCombateàFome eMinistério daSaúde. Núcleode Pesquisas Epidemiológicasem Nutric¸ãoeSaúde e DepartamentodeNutric¸ãodaFaculdadedeSaúdePúblicada UniversidadedeSãoPaulo;2006.
2.UnitedNations.Themillenniumdevelopmentgoalsreport2012. NewYork:UnitedNations;2012.
3.Bittencourt AS, Niquini RP, Reis AC, Leal MC. Assistência a crianc¸asdesnutridas:análisededadosdosistemadeinformac¸ão hospitalar doSistemaÚnico deSaúde.RevBrasSaudeMater Infant.2009;9:263---73.
4.SrivastavaD,SinghK,MisraR,PrakashA.Comparisonofcardiac autonomicactivitybetweenmalnourishedandhealthychildren. IndianJPhysiolPharmacol.2012;56:222---8.
5.Vanderlei LC, Pastre CM, HoshiRA, CarvalhoTD, Godoy MF. Noc¸õesbásicasdevariabilidadedafrequênciacardíacaesua aplicabilidadeclínica.RevBrasCirCardiovasc.2009;24:205---17.
6.SawayaAL, SessoR,FlorêncioTM,FernandesMT,MartinsPA. Associationbetweenchronicundernutritionandhypertension. MaternChildNutr.2005;1:155---63.
7.BelchiorAC,AngeliJK,FariaTO,SimonFD,SilveiraEA,Meira EF,et al.Post-weaningproteinmalnutritionincreases blood, pressureandinducesendothelialdysfunctionsinrats.PLoSONE. 2012;7:e34876.
8.SilvettiMS,DragoF,RagoneseP.Heartratevariabilityinhealthy childrenandadolescentsispartiallyrelatedtoageandgender. IntJCardiol.2001;81:169---74.
9.CysarzD,LinhardM,EdelhauserF,LanglerA,VanLeeuwenP, HenzeG,etal.Unexpectedcourseofnonlinearcardiac inter-beatintervaldynamicsduringchildhoodandadolescence.PLoS ONE.2011;6:e19400.
10.Childgrowthstandardsandtheidentificationofsevereacute malnutritionininfantsandchildren:aJointStatementbythe WorldHealth Organizationand theUnitedNationsChildren’s Fund.Geneva:WorldHealthOrganization(WHO);2009.
11.Sociedade Brasileira de Cardiologia/Sociedade Brasileira de Hipertensão/SociedadeBrasileira de Nefrologia.VI diretrizes brasileirasdeHipertensão.ArqBrasCardiol.2010;95:1---51.
12.deRezendeBarbosaMP,SilvaNT,deAzevedoFM,PastreCM, VanderleiLC.ComparisonofPolar®RS800G3TMheartrate mon-itorwithPolar® S810iTMandelectrocardiogram toobtainthe seriesofRRintervalsandanalysisofheartratevariabilityat rest.ClinPhysiolFunctImaging.2016;36:112---7.
13.SessoR,BarretoGP,NevesJ,SawayaAL.Malnutritionis associ-atedwithincreasedbloodpressureinchildhood.NephronClin Pract.2004;97:c61---6.
14.GodardCM,Munoz M,Sanchez MA,Vallotton MB,RiondelA. Astudyoftherenin-angiotensin-aldosteronesysteminsevere infantilemalnutrition.IntJPediatrNephrol.1986;7:39---44.
15.ZureikM,Bonithon-KoppC,LecomteE,SiestG,DucimetiereP. Weightsatbirthandinearlyinfancy,systolicpressure,andleft ventricularstructureinsubjectsaged8---24years.Hypertension. 1996;27:339---45.
16.Leon-Quinto T, Magnan C, Portha B. Alteredactivity of the autonomousnervoussystemasadeterminantoftheimpaired -cellsecretoryresponseafterprotein-energyrestrictioninthe rat.Endocrinology.1998;139:3382---9.
17.SomovaLI,MoodleyK.Theeffectofproteinenergy malnutri-tionondevelopmentofhypertension,glucosemetabolismand insulinsensitivityingeneticallyhypertensiverats.NutrMetab CardiovascDis.2000;10:188---94.
18.JacobsonL, Zurakowski D,Majzoub JA. Protein malnutrition increases plasma adrenocorticotropin and anterior pituitary propiomelanocortin messenger ribonucleic acid in the rat. Endocrinology.1997;138:1048---57.
19.Skrzypczyk P, Roszkowska-Blaim M, Daniel M. Hypertensive crisis in children and adolescents. Pol Merkur Lekarski. 2013;35:379---84.
20.CattermoleGN,LeungPY,MakPS,ChanSS,GrahamCA,Rainer TH.Thenormalrangesofcardiovascularparametersinchildren measuredusingtheultrasoniccardiacoutputmonitor.CritCare Med.2010;38:1875---81.
21.MannMC,ExnerDV,HemmelgarnBR,SolaDY,TurinTC,EllisL, etal.VitaminDlevelsareassociatedwithcardiacautonomic activityinhealthyhumans.Nutrients.2013;5:2114---27.
22.MartinsCD,ChiancaDA,FernandesLG.Cardiacautonomic bal-anceinratssubmittedtoproteinrestrictionafterweaning.Clin ExpPharmacolPhysiol.2011;38:89---93.
23.Vogele C, Hilbert A, Tuschen-Caffier B. Dietary restriction, cardiacautonomicregulationand stress reactivityinbulimic women.PhysiolBehav.2009;98:229---34.
24.Thayer JF, Lane RD. The role of vagal function in the risk for cardiovascular disease and mortality. Biol Psychol. 2007;74:224---42.
25.PlagemannA,HarderT,RakeA,MelchiorK,RohdeW,Dorner G.Hypothalamicnucleiaremalformedinweanlingoffspringof lowproteinmalnourishedratdams.JNutr.2000;130:2582---9.
26.KimSW,YuBP,SanderfordM,HerlihyJT.Dietaryrestriction mod-ulatesthenorepinephrinecontentanduptakeoftheheartand cardiacsynaptosomes.ProcSocExpBiolMed.1994;207:43---7.
27.NonogakikK.Newinsightintosympatheticregulationofglucose andfatmetabolism.Diabetologia.2000;43:533---49.
28.PetersonHR,RothschildM,WeinbergCR,FellRD,McLeishKR, PfeiferMA.Bodyfatandtheactivityoftheautonomicnervous system.NEnglJMed.1988;318:1077---83.
29.VanderleiLC,PastreCM,JuniorIFF,GodoyMF.Analysisof car-diacautonomic modulation inobese and eutrophic children. Clinics.2010;65:789---992.