RevBrasAnestesiol.2016;66(5):529---532
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
MISCELLANEOUS
Correlation
of
computed
tomography,
magnetic
resonance
imaging
and
clinical
outcome
in
acute
carbon
monoxide
poisoning
Namik
Ozcan
a,∗,
Giray
Ozcam
a,
Pinar
Kosar
b,
Ayse
Ozcan
a,
Hulya
Basar
a,
Cetin
Kaymak
aaDepartmentofAnesthesiologyandReanimation,IntensiveCareUnit,AnkaraTrainingandResearchHospital,Ankara,Turkey bDepartmentofRadiology,AnkaraTrainingandResearchHospital,Ankara,Turkey
Received18February2014;accepted5May2014
Availableonline2June2014
KEYWORDS
Intensivecare; Carbonmonoxide; Imaging;
Poisoning
Abstract
Backgroundandobjectives: Carbonmonoxideisatoxicgasforhumansandisstillasilentkiller inbothdevelopedanddevelopingcountries.Theaimofthiscaseserieswastoevaluateearly radiologicalimagesasapredictorofsubsequentneuropsychologicalsequelae,followingcarbon monoxidepoisoning.
Case1: Aftercarbonmonoxideexposure,earlycomputedtomographyscansandmagnetic res-onanceimagingfindingsofa52-year-oldwomanshowedbilaterallesionsintheglobuspallidus. This patient was discharged and followed for 90 days. The patient recovered withoutany neurologicalsequela.
Case2: Ina58-year-oldwomanexposedtocarbonmonoxide,computedtomographyshowed lesionsinbilateralglobuspallidusandperiventricularwhitematter.Earlymagneticresonance imagingrevealedchangessimilartothatlikeinearlytomographyimages.Thepatientrecovered andwasdischargedfromhospital.Onthe27thdayofexposure,thepatientdeveloped disorien-tationandmemoryimpairment.Latemagneticresonanceimagingshoweddiffusehyperintensity inthecerebralwhitematter.
Conclusion: Whitematter lesions which progressto demyelinationand endup in neuropsy-chologicalsequelaecannotalwaysbediagnosedbyearlycomputedtomographyandmagnetic resonanceimagingincarbonmonoxidepoisoning.
©2014SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mails:[email protected],[email protected](N.Ozcan). http://dx.doi.org/10.1016/j.bjane.2014.05.006
530 N.Ozcanetal.
PALAVRAS-CHAVE
Tratamentointensivo; Monóxidodecarbono; Imagem;
Intoxicac¸ão
Correlac¸ãodetomografiacomputadorizada,ressonânciamagnéticaeresultados
clínicosemintoxicac¸ãoagudapormonóxidodecarbono
Resumo
Justificativaeobjetivos: Monóxidodecarbonoéumgástóxicoparaossereshumanos,além deserumassassinosilenciosoempaísestanto desenvolvidosquantoemdesenvolvimento.O objetivodestasériedecasosfoiavaliarasimagensradiológicasiniciaiscomoumpreditivode sequelasneuropsicológicassubsequentesapósintoxicac¸ãopormonóxidodecarbono.
Caso1: Apósexposic¸ãoaomonóxidodecarbono,osachadosiniciaisemtomografias computa-dorizadaseressonânciasmagnéticasdeumamulherde52anosdeidademostraramlesõesem globopálidobilateralmente.Apacienterecebeualtaefoiacompanhadapor90dias.Apaciente serecuperousemsequelasneurológicas.
Caso2: Pacientedosexofeminino,58anosdeidade,expostaaomonóxidodecarbono.A tomo-grafiacomputadorizadamostroulesõesemglobopálido,bilateralmente,esubstânciabranca periventricular.A ressonância magnética inicial reveloualterac¸ões semelhantes àquelas em tomografias precoces. A paciente se recuperou erecebeu alta. No vigésimo sétimo dia de exposic¸ão,apacienteevoluiucomdesorientac¸ãoeperdadememória.Ressonânciamagnética posteriormostrouhiperintensidadedifusadasubstânciabrancacerebral.
Conclusão:Aslesõesdasubstânciabrancaqueprogridemparadesmielinizac¸ãoeresultamem sequelasneuropsicológicasnemsemprepodemserdiagnosticadasemtomografiase ressonân-ciasiniciaisemcasosdeintoxicac¸ãopormonóxidodecarbono.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Carbonmonoxide(CO)isawell-known,colorlessand odor-less gas that is toxic to all kinds of human tissues.1,2
FollowingexposuretoCO,morphologicchangesareseenin regionsofthebrainwithinhours.3---5Bilateraldemyelination
ofthe cerebral whitematter, hyperintensities of centrum semiovale,andhemorrhagicnecrosisoftheglobuspallidus are some of the neuropathologic findings seen after CO poisoning.4,6
Theaimsofthisstudyweretoevaluatetheintegrityof brainwhitematterandbasalganglionswithmagnetic reso-nanceimaging(MRI)andcomputedtomography(CT)inthe acutephaseofCOexposure,andtoevaluateearly radiolog-icalimagesasapredictorofsubsequentneuropsychological sequelae,followingCOpoisoning.
Case
1
A52-year-oldwomanwasfound unconsciousat homeand referredtohospitalwithpossible COpoisoning.Her heart ratewas95beatsmin−1,respiratoryratewas25min−1and
bloodpressuremeasuredwas90/60mmHg.Resultsof arte-rialbloodgasanalysiswerepH:7.38,pO2:25mmHg,pCO2: 40mmHg,HCO3:20.9mEqL−1,COHb:46.4%,BE:
−12.7,and
lactate:7mEqL−1 (<1.5).Laboratoryfindingsshowed
Myo-globin:488ngmL−1(0---38.5),CK:147UL−1(0---145),CK-MB:
16.11ngmL−1 (0---5.6), andtroponin-I:0.048
gL−1 (<0.1).
Inneurologicalexamination,thepatientwascomatosewith aGlasgowComaScale(GCS)scoreof9/15andpupilswere mydriatic.
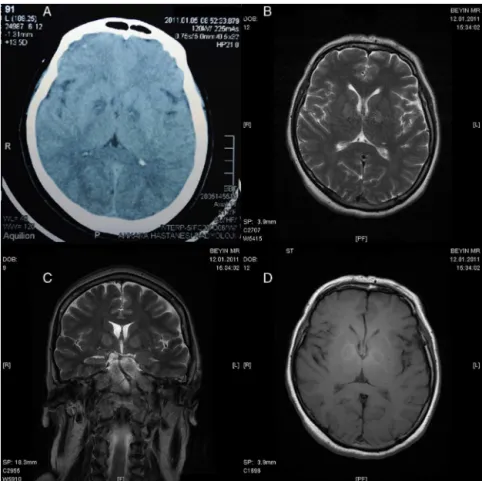
AxialCTscansshowedbilateralhypodensityintheglobus palliduswithinfirst24h(Fig.1A).MRI findingsonthe7th dayofexposurewerebilateralhyperintensityintheglobus pallidusonaxial,coronalT2-weighted(T2)(Fig.1BandC), and axialFLAIR sequences.In addition, axialand sagittal unenhancedT1-weighted(T1)(Fig.1D)imagesinterestingly revealedperipheralhyperintensityoftheglobuspallidus.
The patient progressivelyrecovered within3 days and wasdischargedfromthehospitalonthe8thdayof admis-sion. The patient was followed for 90 days and did not developanyneurologicalsequela.
Case
2
A 58-year-oldwomanwas admittedtointensive care unit after several hours of CO exposure. The clinical exam-ination revealed heart rate 80beatsmin−1, respiratory
rate15min−1, andblood pressure80/60mmHg.Results of
blood gas analysiswere pH:7.18, pO2:11.6mmHg,pCO2: 50mmHg,HCO314.9mEqL−1,COHb:56.2%,BE:
−12.7,and
lactate: 9mEqL−1 (<1.5). The laboratory findings showed
myoglobin 4000ngmL−1 (0---38.5), CK: 247UL−1 (0---145),
CK-MB: 27.6ngmL−1 (0---5.6), and troponin-I 0.131gL−1
(<0.1),andProBNP1040pmolL−1(<350).Physical
examina-tionshowedmydriaticpupilsandpapilledema,theGCSscore of5/15,andthepatienthadgeneralizedconvulsions.
Radiologyandoutcomeincarbonmonoxidepoisoning 531
Figure1 (A)AxialCT,(B)axialT2MRI,(C)coronalT2MRI,and(D)axialT1MRIofCase1.
532 N.Ozcanetal.
capsuleinaxialT2,axialFLAIR(Fig.2C),coronalT2images. Cerebralwhitematterchangeswerenotobservedinanyof theimages.
Thepatientrecoveredwithin5days.Shewasdischarged fromthehospitalonthe8thdayofadmission.Thispatient haddeveloped disorientationand memory impairment on the27thdayof follow-up.Anotherdiffusion MRIwas per-formedonthe30thdayofexposure.Inadditiontoprevious findings,diffusehyperintensityinthecerebralwhitematter appeared,whichwasconsistentwithwhitematterdamage inaxialT2imagesanddiffusionT2images(Fig.2D).
Conclusion
Acute and intense CO exposure can lead to diffuse hypoxic---ischemic encephalopathy, including basal ganglia andcerebral whitematter involvement.3,7The globus
pal-lidusisthemostcommonsiteofinvolvementofbasalganglia in CO poisoning.4,6,8 Several studies concluded that there
may bea correlation between acute stage hypoperfusion areas and the neuropsychiatric symptoms which develop consequently.1,3,7,9,10 Ithasbeensuggestedthatwhite
mat-terlesionsweremorecommonlyassociatedwithneurologic sequelaecomparedtolesionsintheglobuspallidus.10
After CO inhalation, globus pallidus damage usually occurs immediately, and cerebral white matter damage occurswithinhours.3---5 Ithasbeen reportedthatthemost
commondemyelinationareasaretheperiventricularwhite matterandcentrumsemiovale.4,6,7Inseverecases,
demyeli-nationcanextendtothesubcorticalwhitematter, corpus callosum,andexternalandinternalcapsules.Thesefindings correlatewellwiththeprognosis.4
In our cases,bilateral andsymmetrical hypodensity of globuspalliduswaspresentinearlyCTscansofbothcases. In early MRIs, globus pallidus was isointense in the first case and in the second, interestingly, the periphery of globuspalliduswashyperintenseinT1images.However,we observedthetypicalfindingofCOpoisoninginT2andFLAIR images,bilateral,symmetricalhyperintenseglobuspallidus forbothcases.Inaddition,theposteriorcrusofthe inter-nal capsule was hyperintense in T2 and FLAIR images for thesecond case.IncontrolMRIexaminationofthesecond case,which wasperformedone monthlater,we observed diffuselyhyperintensewhitematterinT2andFLAIRimages whichindicateswhitematterdamage.Restricteddiffusion inthe white matter, whichreflects cytotoxicedema, was observedinDWimagesandADCmap,atthesametime.
Inconclusion,ourcasesconfirmtheregionalspecificityof COpoisoninginthecerebralwhitematterandbasalganglia. Whitematterlesionsprogresstodemyelination,whichcan bepredictiveofoutcomeandneuropsychologicalsequelae. EarlyCTandMRIimagesdonotalwayscorrelatewellwith theclinicaloutcome.FurthercasesofCTandMRIwithlarger numbersofpatientsareneededtodemonstratetheclinical outcomeandprognosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Kim HJ, Chang KH, Song IC, et al. Delayed encephalo-pathy of acute carbon monoxide intoxication: diffusivity of cerebral white matter lesions. Am J Neuroradiol. 2003;24: 1592---7.
2.OmayeST.Metabolicmodulationofcarbonmonoxidetoxicity. Toxicology.2002;180:139---50.
3.ThomSR, FisherD, ManevichY.Roles for platelet-activating factor and NO-derived oxidants causing neutrophil adher-ence after CO poisoning. Am J Physiol Heart Circ Physiol. 2001;281:H923---30.
4.Porter SS, Hopkins RO, Weaver LK, et al. Corpus callosum atrophy and neuropsychological outcome following car-bon monoxide poisoning. Arch Clin Neuropsychol. 2002;17: 195---204.
5.O’DonnellP,BuxtonPJ,PitkinA,etal.Themagneticresonance imagingappearancesof thebraininacute carbon monoxide poisoning.ClinRadiol.2000;55:273---80.
6.ChuK,JungKH,KimHJ,etal.Diffusion-weightedMRIand99m Tc-HMPAOSPECTin delayedrelapsing type ofcarbon monoxide poisoning:evidenceofdelayedcytotoxicedema. EurNeurol. 2004;51:98---103.
7.Chang KH, Han MH,Kim HS, et al. Delayed encephalopathy afteracutecarbonmonoxideintoxication:MRimagingfeatures and distributionofcerebral whitematterlesions. Radiology. 1992;184:117---22.
8.LoCP,ChenSY,LeeKW,etal.Braininjuryafteracutecarbon monoxidepoisoning:earlyand latecomplications. AJRAmJ Roentgenol.2007;189:W205---11.
9.Silver DA, Cross M, Fox B, et al. Computed tomography of the brain in acute carbon monoxide poisoning. Clin Radiol. 1996;51:480---3.