SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Arthroscopic
surgical
treatment
of
recalcitrant
lateral
epicondylitis
–
A
series
of
47
cases
夽
Alexandre
Tadeu
do
Nascimento
∗,
Gustavo
Kogake
Claudio
HospitalOrthoservice,GrupodeOmbroeCotovelo,SãoJosédosCampos,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14December2015 Accepted18March2016
Availableonline21December2016
Keywords:
Tenniselbow/pathology Tenniselbow/therapy Tenniselbow/surgery Arthroscopy
Retrospectivestudies
a
b
s
t
r
a
c
t
Objective:Toevaluatetheresultsofpatientsundergoingarthroscopicsurgicaltreatmentof refractorylateralepicondylitis,identifyingpoorprognosisfactors.
Methods:A retrospective study of44 patients (47 elbows)who underwent arthroscopic debridementoftheextensorcarpiradialisbrevis(ECRB)tendontotreatrefractorylateral epicondylitisfromFebruary2013toFebruary2015,operatedbyasinglesurgeonatone cen-ter.PatientswereassessedbyDASHscore,visualanalogscaleofpain(VAS),andShortForm 36(SF-36).Themeanageatsurgerywas44.4years(32–60).Thedurationofsymptomsprior tothesurgerywasapproximately2.02years(range:6monthsto10years).Meanfollow-up was18.6months(rangeof6–31.9).
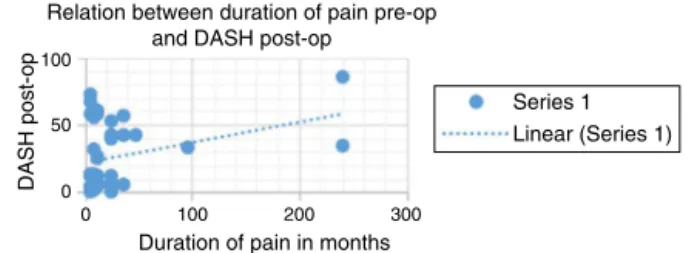
Results:ThemeanpostoperativeDASHscorewas25.9points;meanVAS,1.0pointatrest (allthepatientswithmildpain)and3.0pointsatactivity,ofwhich31(66%)casespresented mildpain,10(21%)moderatepain,andsix(13%)severepain;meanSF-36scorewas62.5.A moderatecorrelationwasobservedbetweendurationofpainbeforesurgeryandtheDASH scorewiththefinalfunctionaloutcome.Nosignificantcomplicationswiththearthroscopic procedurewereobserved.
Conclusions:Arthroscopicsurgicaltreatmentforrecalcitrantlateralelbowepicondylitis pre-sentedgoodresults,beingeffectiveandsafe.Theshorterthetimeofpainbeforesurgery andthelowerthepreoperativeDASHscore,thebettertheprognosis.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheHospitalOrthoservice,GrupodeOmbroeCotovelo,SãoJosédosCampos,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.T.Nascimento). http://dx.doi.org/10.1016/j.rboe.2016.03.008
Tratamento
cirúrgico
artroscópico
da
epicondilite
lateral
recalcitrante
–
Série
de
47
casos
Palavras-chave:
Cotovelodetenista/patologia Cotovelodetenista/terapia Cotovelodetenista/cirurgia Artroscopia
Estudosretrospectivos
r
e
s
u
m
o
Objetivo:Avaliarosresultadosdospacientessubmetidosatratamentocirúrgicoartroscópico da epicondilitelateral refratáriaa tratamentoconservadore identificar fatoresde pior prognóstico.
Métodos: Estudoretrospectivode44pacientes(47cotovelos)submetidosadesbridamento cirúrgicoartroscópicodotendãoextensorradialcurtodocarpo(ERCC)paratratamentode epicondilitelateralrefratáriaatratamentoconservadordefevereirode2013a fevereiro de2015,operadosporumúnicocirurgiãoemumúnicocentro.Ospacientesforamavaliados peloescoredeDASH,pelaclassificac¸ãovisualanalógicadedor(EVA)epeloShort-Form36 (SF-36).Amédiadeidadenacirurgiafoide44,4anos(32a60).Otempodesintomasantes dacirurgiafoide2,02anos(variac¸ãodeseismesesa10anos).Oseguimentomédiofoide 18,6meses(variac¸ãodeseisa31,9).
Resultados:Amédiadosescorespós-operatóriosfoide25,9pontosnoDASH;1pontonoEVA derepouso(todososcasosdedoresleve)e3pontosnaEVAematividade,31(66%)casos dedoresleves,10(21%)demoderadaseseis(13%)deintensas;SF-36de62,5.Observou-se umacorrelac¸ãomoderadaentreotempodedorantesdacirurgiaeapontuac¸ãonoescore deDASHcomoresultadofuncionalfinal.Nãoforamobservadascomplicac¸õessignificativas comoprocedimentoporviaartroscópica.
Conclusões: Otratamentocirúrgicoartroscópicoparaepicondilitelateralrecalcitrantedo cotoveloapresentabonsresultados,éeficazeseguro.Quantomenorotempodedorantes dacirurgiaequantomenoroDASHpré-operatório,melhoroprognóstico.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Lateralepicondylitis,or“tenniselbow”isthemostcommon complaintrelatedtotheelbow,affecting1–3%oftheadult pop-ulationannually.1,2 Despite theclassicaldescriptionrelated totennis practice, only5–10% ofpatients with epicondyli-tispracticethissport;theconditionismorerelatedtowork activities.3Althoughthenamesuggestsaninflammatory pro-cess, epicondylitis is characterizedas a non-inflammatory condition,atypeoftendinosis withfibroblastandvascular response,calledangiofibroblasticdegeneration.4Thisisa self-limitingpathology,andthevastmajorityofpatientsimprove withconservativetreatmentonly.However,somefactorssuch asduration ofsymptoms, previousinfiltration, prior ortho-pedic surgery, and work-related compensation, are known toberelatedtopoorprognosis, increasingthe chanceofa needforsurgery.5Therecurrencerateis8.5%,andpatients whosesymptoms last oversix monthshavea highrisk of presentingthemforlong periodsandwillprobablyrequire surgicalintervention6;theseareestimatedtorepresent4–16% ofcases.5,7,8Numeroussurgicalprocedurestotreatthis con-ditionhavebeen described.4,9–11 Thevast majorityhave in commonthereleaseordebridementoftheextensorcarpi radi-alisbrevis(ECRB)tendon.Somefactorshavebeenattributedto poorprognosisaftersurgicaltreatment,especiallyfemale gen-derandinjuryofthecommonextensortendongreaterthan 6mminmagneticresonanceimaging12(Fig.1).
Arthroscopic surgical treatment of lateral epicondylitis has advantagesover open surgery,including the ability to
debridetheinferiorsurfaceofthetendonwithoutinvading theaponeurosisofthecommonextensor(Fig.2),theability toassessthejointforintra-articularpathology,andashorter rehabilitationperiod.7,13
Material
and
methods
Patients included in this study were operated from Febru-ary 2013 to February 2015by a single surgeon at a single center. Thestudy includedpatients diagnosed with lateral epicondylitis who showedeitherno improvementor unsa-tisfactoryimprovementafterconservativetreatment,which consistedofsixmonthsofphysicaltherapyassociatedwithan orthosisforlateralepicondylitis,twoinfiltrationsortwo intra-muscularsteroidinjections,andmedicationsforpainrelief.
Patients with lateral epicondylitis who had chondral lesions, incipient arthrosis, or cases with previous elbow surgerywereexcluded.
TheDASH,VAS,andSF-36scoreswerecalculatedforall patientspreoperativelyandatthepostoperativefollow-up.
Surgicaltechnique
The surgical technique adopted was based on published reports,1,9withsomeadjustments.
Fig.1–Magneticresonanceimagingshowingcommon
extensortendonlesion(arrow).
tobemovedfrom 90◦ offlexion tofullextension.A pneu-matictourniquetwasplacedattherootofthearm.Surgical landmarksweredrawnontheelbow,includingtheolecranon, lateralepicondyle,medialepicondyle,radialhead,andulnar nerve.
Theelbowjointwasinflatedwith40mLofsaline,placedat theelbowpuncturesiteinthemiddleofatriangleformedby thelateralepicondyle,theradialhead,andtheolecranon,to facilitateentranceofthearthroscopeintotheintra-articular space.
Theanterosuperomedialand anterosuperolateralportals werepreferred,startingwiththeformer,wherethetrochanter andthearthroscopewereplaced.Thesecondportalismade withthehelpofaneedleunderintra-articularvisualizationto
enhanceitspositioning.Acompleteanalysisoftheanterior compartmentoftheelbowjointismade,includingthejoint andthecapsulesurfaces.
Then,a partialcapsulotomyofthe lateralregion is per-formedtoallowthevisualizationoftheECRBorigin,whichis extra-articular.Witharadiofrequencydevice,theECRBtendon isdetachedfromthehumerus.Then,thedisengagedtendon isdebridedwithasofttissueshaverandthelateralportionof thehumerus,withaboneshaver,inordertocausebleeding andcellmigrationtotheregion.TheoriginoftheECRBtendon isnotreinserted.
The collateral ligament may be damaged if the ECRB resectionismade“blindly,”duetothecollapseoftheanterior softtissueinto theviewingspace.Forthis reason,an infu-sionpumpwasusedinallcases(approximately60mmHg), maintainingthejointinflated.
Postoperativeperiod
Intheimmediatepostoperativeperiod,patientswere immo-bilizedwithasling(forthreetofivedays),forcomfortonly; movementwasauthorizedaccordingtopain,andonly exer-tion withthe affected limbwasavoided. Physiotherapyfor range ofmotiongain wasstarted aftertwoweeks; isomet-ricstrengtheningwasinitiatedafterfullrangeofmotionwas achieved,typicallyaroundfourweekspostoperatively. Resis-tanceexerciseswereinitiatedfourtosixweeksaftersurgery. Unrestricted use ofthelimbwas authorizedafter approxi-mately12weeks.
Statisticalanalysis
Statisticalanalysiscomparedthepre-andpostoperative mea-surementswithStudent’st-test.Two-tailedpairedtestswere usedinallcases;p-values<0.05were consideredas signifi-cant.Pearson’scoefficientwasusedtoassesspossiblefactors thatinterfereinthefinalresult;valuesbetween0and0.3were consideredasweakcorrelation,between0.3and0.6,as mod-erate,andgreaterthan0.6,asstrong.Negativevaluesindicate aninversecorrelation;positivevalues,adirectcorrelation.
Results
Inclusioncriteriaweremetby44patients(47elbows),30men and14women.Meanageatsurgerywas44.4years(32–60). The mean duration of symptoms before surgery was 2.02
Fig.2–ArthroscopicimagesshowingacaseofaBakerIIepicondylitis,7openingofthelateralcapsule,debridement,and
Table1–ResultsofDASHandVASscores.
DASH VAS
Preoperativeperiod 50.1±19.9(3.33–90)a 7.8±1.8(3–10)a
Postoperativeatrest 25.9±23.8(0–85)a 1.0±0.9(0–3)a
Postoperativeduring activity
25.9±23.8(0–85)a 3.0±2.7(0–9)a
p-Value <0.001 <0.001
a Valuesareexpressedasmeanandstandarddeviation;therange
ispresentedinparentheses.
years(range: sixmonths to10 years).Meanfollow-up was 18.6months(range:6–31.9).Atotalof31rightelbowsand16 leftwere operated.Thedominantarmwasaffectedin65% ofcases.Overall,82%ofallpatientsdescribedtheirworkas “repetitivemotion”;24%receivedsomesocialsecurity bene-fit.Thecauseofthediseasewasclassifiedasassociatedwith laboractivityin32patients(73%);inthree(7%),duetotennis practice;andinfive(11%),duetotrauma.
The study included patients diagnosed with lateral epicondylitiswho showed eithernoimprovementor unsa-tisfactoryimprovementafterconservativetreatment,which consistedofsixmonthsofphysicaltherapyassociatedwithan orthosisforlateralepicondylitis,twoinfiltrationsortwo intra-muscularsteroidinjections,andmedicationsforpainrelief. TheresultsfortheimprovementintheVASandDASHscores areshowninTable1.ThemeanpostoperativeDASHscorewas 25.9points.Meanpost-operativeVASwas3points;31patients (66%)presentedmildpain,10(21%),moderatepain,andsix (13%),intensepain. For theVAS,painwas assessedduring activities,notduringrest.MeanSF-36was62.5.Threepatients (6.3%)showednoimprovementwiththeprocedure.Thirteen patients(29%)wereamateurathletes;aftertheprocedure,10 (77%)wereabletoreturntothesamelevelofactivitypriorto theinjuryandthree(23%)wereunabletoreturntoprevious sport.Pearson’scoefficientdemonstratedamoderate correla-tionbetweendurationofpainbeforesurgeryandDASHscore withfinalfunctionaloutcome.
TheresultsofSF-36weresubdividedaccordingtoitsareas; thedetailedresultsarepresentedinTable2.
Afterevaluatingresultsofscores,thecorrelationofsome variableswiththeoutcomewasassessed(Table3).Pearson’s coefficientwas usedforthis analysis, and novariable was showntohaveastrong correlationwith theoutcome.Two variablesshowedmoderate correlationwiththe finalDASH
Table3–Pearson’scoefficientforthecorrelation betweenthevariablesandtheoutcomeoftreatmentby DASHandVAS.
DASH VAS
Patientreceivespensionbenefit 0.25 0.20
Repetitivework 0.01 0.01
Age −0.24 −0.15
Durationofpreoperative 0.30 0.16
Pre-opfunctionalcapacitybySF-36 −0.09 −0.16 Pre-oplimitationduetophysicalaspectsby
SF-36
0.3 0.18
Pre-oppainbySF-36 −0.22 −0.13
Pre-opgeneralhealthbytheSF-36 −0.17 −0.09
Pre-opvitalitybySF-36 −0.18 −0.21
Pre-opsocialaspectsbySF-36 −0.29 −0.29 Pre-oplimitationsduetoemotionalaspects −0.13 −0.10
Pre-opmentalhealth −0.13 −0.18
DASH 0.58 0.52
VAS 0.15 0.22
Femalegender 0.1 0.17
10
5
0
20
0 40 60 80 100
DASH pre-op Linear (Series 1)
Relation between pre-op DASH and post-op VAS
VAS post-po
–5
Fig.3–Scatterplot(variable:DASHpre-op).
10 5 0 50 0 DASH pre-op
Relation between DASH pre-op and post-op
DASH post-op
Series 1
Linear (Series 1)
100 –5
Fig.4–Scatterplot(variable:DASHpre-op).
andVAS;thecorrelationwasstrongerforpreoperativeDASH scorethan forduration ofpain beforesurgery.This superi-orityinthecorrelationcanbeobservedinTable3(Pearson’s coefficient),andinthescatterplotsshowninFigs.3–5.
Table2–SF-36–comparisonofthepre-andpostoperativeperiods.a
Functional capacity Limitationdue tophysical aspects Pain General health Vitality Social aspects Limitationsdue toemotional aspects Mental health
Pre-op 67.5±16.9 (25–100)
22.4±35.7 (0–100)
35.8±21.3 (0–80)
69±19.6 (30–100)
55.4±24.5 (5–100)
78.3±27.2 (0–100)
39.5±45.1 (0–100)
63.5±23 (4–100) Post-op 72±21.5
(15–100)
37.5±46.2 (0–100)
55.5±25.2 (10–90)
65.7±21 (15–100)
68±23.5 (0–100)
76.9±24.6 (0–100)
47±45.3 (0–100)
77.7±17.6 (28–100)
p-Value 0.03 0.01 0.000003 0.25 0.004 0.007 0.40 0.0003
100
50
0
0 100
Duration of pain in months
Series 1 Linear (Series 1) Relation between duration of pain pre-op
and DASH post-op
DASH post-op
200 300
Fig.5–Scatterplot(variable:durationofpainbefore
surgery).
Complications
Twopatientshadsuperficialinfection,whichimprovedafter oneweekoforalantibiotictherapy. Asecond debridement was not necessary, and no additional complications were observed.
Discussion
Lateralepicondylitisisacommondiagnosisthatrespondswell toconservativetreatment.Surgicalinterventionisnecessary when symptomsdo notimprove or whenimprovement is unsatisfactoryafteratleastsixmonthsoftreatment,which occurs in 4–16% of cases.5,7,8 Thepresent study evaluated the functional responseand pain inthis groupofpatients withrecalcitrantepicondylitis whounderwent arthroscopic debridementoftheECRB tendon.Significantimprovements wereobservedinscoresstudied,withtheexceptionofonly twoitemsfromSF-36.ResultsobtainedattheVASare con-sistentwiththeliterature,whichshowsslightlybetterresults whenthescoreismeasuredwiththepatientatrestthan dur-ingactivitywiththeupperlimb.14
TheliteratureindicatesthattheDASHscoreresultsforthis typeoftreatmentaregood.Inastudycomparingthe arthro-scopicprocedure withapercutaneoustechnique,theDASH scorewasassessedbeforeandaftersurgery,showing signifi-cantresults(p<0.05).TheDASHscorechangedfrom72to48 pointsinarthroscopiccasesandfrom70to50inthe percu-taneousgroup.15Inthepresentstudy,patientshadalower meanfinalscore(25.9points),butthemeanpreoperative val-ueswerealsolower.OtherBrazilianstudieshavealsoshown goodresultswiththissurgery,observingasignificant improve-mentinthescoresevaluated.16–18
Despitethegoodresults,itshouldbenotedthat approxi-mately23%ofpatientswhowereamateurathletesfailedto returnto the level ofactivity priortothe injury or had to changesports.Anotherpointtoconsideristhatthreepatients (6%ofcases)didnotobserveanyimprovementwithsurgical treatment.
Somestudies indicate that, regardless ofthe technique used,resultsofepicondylitissurgeryarenotuniform.Verhaar etal.19reportedapatientsatisfactionrateof66%inoneyearof follow-up.Onlyone-thirdofthepatientshadreturnedtowork. NirschlandPettrone4reportedthat 85%ofpatients treated withopentechniquehad completereliefofsymptomsand hadnoactivityrestrictions.Inthepresentstudy,onlyseven patients(15%)hadcompleteremissionofsymptomseven dur-ingmanualactivity.
Oneoftheadvantagesofthearthroscopictreatmentis ear-lierrehabilitation.Owensetal.11reportedimprovementsin16 patientsafterarthroscopicrelease,withameanreturntowork withoutrestrictionofsixdays.
Baker and Baker20 publishedthe long-termresults ofa cohortstudyandindicatedthattheydidnotdeteriorateover time.Patientswhowerewellaftertwoyearsmaintainedtheir functionallevel,withoutworseningpaininsomecases,even tenyearsaftertheprocedure.
Asforprognosticfactors,preoperativeDASHandduration ofpainpresentedamoderatecorrelation.Thesefactorsmay berelatedtotheseverityofthecondition.Otherstudies12have detectedasprognosticfactors the femalegender, whichin thepresentstudyshowednoassociation,andthestageofthe conditionatresonance,notassessedinthepresentstudy.
Conclusions
Arthroscopicsurgeryforthetreatmentofrecalcitrantlateral epicondylitis showed good results, representing an effec-tive and safe technique. With this treatment, a significant improvementinallscoreswasobserved.Theshorterthe dura-tion ofpain beforesurgery and thelower the preoperative DASH,thebetterthepostoperativeresultsare.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LattermannC,RomeoAA,AnbariA,MeiningerAK,McCarty LP,ColeBJ,etal.Arthroscopicdebridementoftheextensor carpiradialisbrevisforrecalcitrantelateralepicondylitis.J ShoulderElbowSurg.2010;19(5):651–6.
2.CohenM,MottaFilhoGR.Epicondilitelateraldocotovelo.Rev BrasOrtop.2012;47(4):414–20.
3.BoyerMI,HastingsH2nd.Lateraltenniselbow:isthereany scienceoutthere?JShoulderElbowSurg.1999;8(5):481–91. 4.NirschlRP,PettroneFA.Tenniselbow.Thesurgicaltreatment
oflateralepicondylitis.JBoneJointSurgAm.1979;61(6):832–9. 5.KnutsenEJ,CalfeeRP,ChenRE,GoldfarbCA,ParkKW,Osei
DA.Factorsassociatedwithfailureofnonoperativetreatment inlateralepicondylitis.AmJSportsMed.2015;43(9):2133–7. 6.SandersTLJr,MaraditKremersH,BryanAJ,RansomJE,Smith
J,MorreyBF.Theepidemiologyandhealthcareburdenof tenniselbow:apopulation-basedstudy.AmJSportsMed. 2015;43(5):1066–71.
7.BakerCLJr,MurphyKP,GottlobCA,CurdDT.Arthroscopic classificationandtreatmentoflateralepicondylitis:two-year clinicalresults.JShoulderElbowSurg.2000;9(6):475–82. 8.CoonradRW,HooperWR.Tenniselbow:itscourse,natural
history,conservativeandsurgicalmanagement.JBoneJoint SurgAm.1973;55(6):1177–82.
9.BakerCL.Arthroscopicversusopentechniquesforextensor tenodesisoftheelbow.TechShoulderElbowSurg.
2000;1:184–91.
11.OwensBD,MurphyKP,KukloTR.Arthroscopicreleasefor lateralepicondylitis.Arthroscopy.2001;17(6):582–7. 12.YoonJP,ChungSW,YiJH,LeeBJ,JeonIH,JeongWJ,etal.
Prognosticfactorsofarthroscopicextensorcarpiradialis brevisreleaseforlateralepicondylitis.Arthroscopy. 2015;31(7):1232–7.
13.SzaboSJ,SavoieFH3rd,FieldLD,RamseyJR,HosemannCD. Tendinosisoftheextensorcarpiradialisbrevis:anevaluation ofthreemethodsofoperativetreatment.JShoulderElbow Surg.2006;15(6):721–7.
14.OkiG,IbaK,SasakiK,YamashitaT,WadaT.Timeto functionalrecoveryafterarthroscopicsurgeryfortennis elbow.JShoulderElbowSurg.2014;23(10):1527–31. 15.OthmanAM.Arthroscopicversuspercutaneousreleaseof
commonextensororiginfortreatmentofchronictennis elbow.ArchOrthopTraumaSurg.2011;131(3):383–8. 16.MartynetzFA,FariacFF,SuperticMJ,MussiFilhoS,Oliveira
LMM.Avaliac¸ãodepacientessubmetidosaotratamento
artroscópicodaepicondilitelateralrefratáriaaotratamento conservador.RevBrasOrtop.2013;48(6):532–7.
17.MiyazakiAN,FregonezeM,SantosPD,daSilvaLA,PiresDC, MotaNetoJ,etal.Avaliac¸ãodosresultadosdotratamento artroscópicodaepicondilitelateral.RevBrasOrtop. 2010;45(2):136–40.
18.ZoppiFilhoA,VieiraLAG,FerreiraNetoAA,BenegasE. Tratamentoartroscópicodaepicondilitelateraldocotovelo. RevBrasOrtop.2004;39(3):93–101.
19.VerhaarJ,WalenkampG,KesterA,vanMamerenH,vander LindenT.Lateralextensorreleasefortenniselbow.A prospectivelong-termfollow-upstudy.JBoneJointSurgAm. 1993;75(7):1034–43.
20.BakerCLJr,BakerCL3rd.Long-termfollow-upofarthroscopic treatmentoflateralepicondylitis.AmJSportsMed.