jcoloproctol(rioj).2017;37(2):144–146
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Colovesical
fistula
secondary
to
hernia
mesh
migration:
an
unusual
incident
Sabarinathan
Ramanathan
∗,
Veeraraghavan
Krishnamoorthy,
Kini
Ratnakar,
Pugazhendhi
Thangavel,
Raju
Sundarraj
RajivGandhiGovernmentGeneralHospital,MadrasMedicalCollege,Chennai,India
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16September2016 Accepted16October2016 Availableonline4February2017
Keywords:
Colovesicalfistula Inguinalherniarepair Meshmigration Poliomyelitis
a
b
s
t
r
a
c
t
Weevaluateda27-yearoldmalewithpneumaturiaandfecaluriawithapasthistoryofright inguinalherniarepair.Though,cystoscopyandcontrastenhancedcomputedtomography didnotfurnishanyevidencetoarriveatadiagnosis,interestingly,colonoscopyrevealeda meshinthesigmoidcolonmakingapparentthediagnosisofcolovesicalfistulasecondary tomeshmigration.Later,surgicalremovalofthemeshfromthesigmoidcolonwithrent closureofthefistulousopeningwasdonesuccessfully.Ourcasethus,highlightsthevital roleofcommondiagnostictoollikecolonoscopyinmakinganuncommondiagnosis.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Fístula
colovesical
secundária
à
migrac¸ão
da
malha
para
reparo
de
hérnia:
um
incidente
incomum
Palavras-chave:
Fístulacolovesical Reparodehérniainguinal Migrac¸ãoderede Poliomielite
r
e
s
u
m
o
Avaliamosum homem de27 anos compneumaturia e fecalúriacom antecedentesde reparodahérniainguinaldireita.Emboraacistoscopiaeatomografiacomputadorizada comcontraste(TCC)nãotenhamfornecidonenhumaevidênciaparaobter-seum diagnós-tico,curiosamente,acolonoscopiarevelouumamalhanocólonsigmoide,estabelecendoo diagnósticodefístulacolovesical(FCV)secundáriaàmigrac¸ãodamalha.Maistarde,foifeita aremoc¸ãocirúrgicadamalhadocólonsigmoidecomfechamentodaaberturafistulosacom sucesso.Nossocaso,portanto,destacaopapelvitaldeumaferramentadiagnósticacomum, comoacolonoscopia,paraobter-seumdiagnósticoincomum.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](S.Ramanathan).
http://dx.doi.org/10.1016/j.jcol.2016.10.002
jcoloproctol(rioj).2017;37(2):144–146
145
Introduction
Enterovesical fistula is the existence of abnormal tract betweenthe bowelandthe bladder,withcolovesicalfistula (CVF)asits mostcommon type.Diverticulitisisdeemedas thecommonestetiologyaccountingforabout65–79%.1 CVF
subsequenttomeshmigrationisanunusualincident,andis rarelyreportedinliterature.WereportacaseofCVFsecondary tomeshmigration,followinginguinalherniarepair.
Case
report
A27-year-oldgentlemanpresentedwitha15dayshistoryof fecaluria and pneumaturiawith anincreasedfrequency of about20timesadaywithoutdiurnalvariation.Healso pre-sentedwithayearhistoryofrecurrentepisodesoffeverwith chills,dysuria,suprapubicpainandtenesmus.Herevealeda pasthistoryofright-sidedpostpoliomyelitisresidual paral-ysis.Abdominalexaminationrevealedtendernessintheleft iliacfossaanddigitalrectalexaminationshowedminimal ten-dernesswithnoothersignificantfindings.Hemoglobinwas 8.6g%suggestiveofanemia,whiletotalleukocytecountand plateletcountwerenormalwith9200cells/c.mmand1.47lakh cells/c.mmrespectively,whereas urinemicroscopyrevealed plenty ofpus cells with its culturegrowing Escherichia coli. Allotherlaboratoryinvestigationswerenormal.Ultrasound abdomen showed debris in the bladder while cystoscopy demonstrated ared glowwith debris inaddition toa bul-lousedemaobservedat7′oclockposition.Contrastenhanced
computedtomography(CECT)scanalsofailedtorevealany phenomenalfinding.Interestingly,colonoscopyvisualized a meshinthesigmoidcolonobscuringthelumen,thus preven-tingthescopetobepassedbeyondthatlevel(Fig.1).Anormal mucosalandvascularpatternwasseenuptothatlevel.On furtherprobingweelicitedthepasthistoryofhaving under-gone alaparoscopicright inguinalhernioplasty using inlay polypropylenemeshsevenyearsback,whichusheredusclose totheplausiblediagnosisofmeshmigration.
Fig.1–Colonoscopicpictureshowingmeshinthesigmoid
colon.
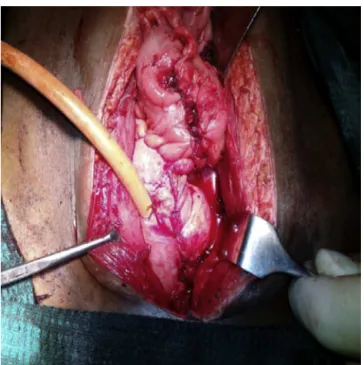
Fig.2–Themesherodingintothesigmoidcolonand
bladder.
Therefore,anexploratorylaparotomywasplanned.Under general anesthesia, a lower midline incision was made, whereintheintra-operativefindingsrevealedtheadherence ofsigmoidloopandleftanterolateralwallofbladderwiththat oftheparietalwallatleftinguinalregion.Subsequently, sig-moid colonwasmobilizedwithutmostcareandopenedin theanti-mesentricborder,transpiredapolypropylenemeshof 11×7cmwiththreetackersprotrudingintothelumenwhile
theotherendofthemeshfounderodingtheleftanterolateral wallofbladder(Figs.2and3).Shortly,theedgesofthefistulous openingonthebladderweretrimmedwithrentclosuredone
146
jcoloproctol(rioj).2017;37(2):144–146Fig.4–Post-oppictureshowingrentclosureofthefistulous
opening.
intwolayerswith28Frmalecotcatheter(Fig.4).Post-operative periodwasuneventful.
Discussion
Laparoscopicinguinalherniarepairusingmeshisknownto reducetherecurrenceofherniabyabout30–50%in compar-ison toopen hernia repair.2 Long term complicationsthat
frequently evinced withthe use ofmeshfor hernia repair arerecurrenceandpain.3AgrawalandAvill4haveinscribed
twoprobablemechanismsofmeshmigrationleadingtoCVF; theeventualityofmeshdisplacementalonganalleyoflow resistance being a consequence of inadequate fixation or anyexternaldisplacingforces.Yetanotherprobable explana-tionissecondarymigrationwhichoccursinsidiouslypastthe anatomicplanesduetoforeignbodyreactionmediated ero-sion,basedonthenatureofthemeshbiomaterialusedand thetypeoffixationofthemesh.
Poliomyelitisexplicitlyreducesthemuscletonepotentially contributingtoplausibleoccurrenceofherniainthispatient.5
Thusthethirdpossiblemechanismwhichcanbeascribedin thisparticularcaseisweaknessofbladderandcolonicwall musclesleadingtomeshmigrationandCVF.
CVFisesteemedasanunusualincident,withonlythree casesbeingreportedinliteraturetilldate,ofwhichtwocases presentedasasequeloflaparoscopicherniarepairandone subsequenttokugelmeshrepair. Soourreportisthethird caseofCVFfollowinglaparoscopicherniarepair.
Conclusion
CVFasaconsequenceofmeshrepair,thoughaveryrare pre-sentation,canbeeasilybediagnosedinsymptomaticpatients presentingyearsafterherniarepairifthereisahighindexof suspicion.Thisisthefirstcaseofmeshmigrationintosigmoid colonbeingdiagnosedbycolonoscopy,indicatingthe cardi-nalroleofcolonoscopywhentheimagingmodalitiesfailin suspectedcaseofmeshmigrationintobowel.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.GolabekT,SzymanskaA,SzopinskiT,BukowczanJ,Furmanek M,PowroznikJ,etal.Enterovesicalfistulae:aetiology,imaging, andmanagement.GastroenterolResPract.2013;2013:617967.
2.McCormackK,ScottNW,GoPM,RossS,GrantAM,EUHernia TrialistsCollaboration.Laparoscopictechniquesversusopen techniquesforinguinalherniarepair.CochraneDatabaseSyst Rev.2003:CD001785.
3.MuschallaF,SchwarzJ,BittnerR.Effectivityoflaparoscopic inguinalherniarepair(TAPP)indailyclinicalpractice:early andlong-termresult.SurgEndosc.2016;30:4985–94.
4.AgrawalA,AvillR.Meshmigrationfollowingrepairofinguinal hernia:acasereportandreviewofliterature.Hernia.
2006;10:79–82.