w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
report
Laparoscopic
hemicolectomy
for
a
patient
with
situs
inversus
totalis
and
colorectal
cancer
Maria
Labalde
Martínez
∗,
Pilar
Veguillas
Redondo,
Jorge
Carlin
Gatica,
Jose
Manuel
Ramia
Angel
HospitalUniversitariodeGuadalajara,DepartamentodeCirugía,Guadalajara,Spain
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6February2017 Accepted28February2017 Availableonline17March2017
Keywords:
Colorectalcancer Situsinversustotalis Laparoscopicsurgery Laparoscopichemicolectomy Congenitalanomaly
a
b
s
t
r
a
c
t
Situsinversustotalisisacongenitalanatomicanomalycharacterizedbyacomplete inver-sionofthoracicandabdominalorgans.Wepresentacaseofa67year-oldpatientdiagnosed withsitusinversustotalsinhischildhoodwhowasreferredforatwo-monthhistoryof hematoquezia. Ascendingcoloncancerwhere foundandheunderwent a laparoscopic hemicolectomywithradicallymphadenectomy.Anexhaustivepreoperativestudyanda detailed planningoflaparoscopicsurgeryincludingpositionsofoperatorandassistants and trocar sites have been performed to beaware of anatomic challenges.The oper-ating timewas120minandblood losswasminimal.Histologicexaminationshoweda well-differentiatedadenocarcinomawithserosalinvasionandwithoutlymphnodes metas-tasis(pT3N0).Thepatientwasdischargedonpostoperative6thdaywithoutcomplications. Laparoscopicsurgeryforcoloncancerinpatientswithsitusinversustotaliscouldbemore difficultneverthelessasafeandfeasibleprocedureshouldbeperformedsuccessfully.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Colectomia
laparóscopica
para
um
paciente
com
situs
inversus
totalis
e
câncer
colorretal
Palavras-chave:
CâncerColorretal Situsinversustotalis Cirurgialaparoscópica Malformac¸ãocongênita
r
e
s
u
m
o
Situsinversustotaliséumaanomaliaanatómicaconsistindoemuminvestimentodeórgãos abdominais.Nesseestudo,descrevemosumpaciente,homem67anos,quefoidiagnosticado comsitusinversustotalisnainfância.Apresentavasintomasdesangramentoretalefoi diag-nosticadocomcâncerdecólondireitoetratadocirurgicamentecomrecec¸ãolaparoscópica. Paraa realizac¸ãodacolectomia laparoscopicaprecisamosde umestudo pré-operatória
∗ Correspondingauthor.
E-mail:[email protected](M.L.Martínez). http://dx.doi.org/10.1016/j.jcol.2017.02.004
completaeumplanodetalhadodecirurgiacomlocalizac¸ãodotrocateresecirurgiões.A cirurgiadurou120minutoseperdedesanguefoimínima.Oresultadodoexamepatológico relatouadenocarcinoma(T3N0).Nossopacientefoiadmitidopor7diasenãoapresentaram complicac¸ões.Paraospacientescomsitusinversus totalisecâncercolorretalarecec¸ão laparoscópicapodesermaisdifícilmaseficazesegura.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Situsinversustotalis(SIT)isacongenitalanatomicanomaly characterizedbyacompleteinversionofallthoracicand intra-abdominalorgansthatcreatesamirrorimageoftheirnormal locations. Theincidence rate of SIT is1 per 10,000–20,000 people and it isinherited ina simpleautosomal recessive manner.1 Surgical procedures in these patients, especially
laparoscopicapproaches,are moredifficultbecauseof con-currentunknowndefectsanddifferentpositionsoftheorgans resultinginanuncommonview.Wepresentacaseofapatient withSITandascendingcoloncancerwhounderwenta laparo-scopichemicolectomy.
Case
report
A 67 year-old male with hypertension and diabetes melli-tuswasreferredbyhispersonalphysiciantothecolorectal surgical department for a 2-months history of hemato-quezia. He and several relatives had been diagnosed with SIT from early childhood. Physical examinationwas unre-markable. Laboratory examination confirmed anemia (red bloodcellcount,3.6×106/mm3;haemoglobin,9.2g/dL;
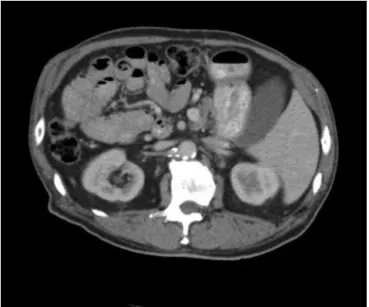
hema-tocrit 29.8%). Adiagnosis ofcolonycancer wasmade after acomplete colonoscopyrevealed anulcerative mass90cm fromanalverge.Histologicexamofcolonoscopybiopsy indi-cated adenocarcinoma. Achest X-ray showed dextrocardia andright-sided gastricairbubble(Fig.1).Echocardiography alsorevealeddextrocardiawithoutcardiacvalvularpathology and cardiac malformation. AbdominalComputed tomogra-physhowedacomplete transposition ofabdominalviscera confirming SIT,a colonicmasslocated inascendingcolon, whichwas invertedto theleft side(Fig.2)and no hepatic andperitonealmetastasis.Theserumconcentrationsof carci-noembryonicantigenandCa19.9wereelevated(12.5ng/mL, referencerate0–4.9ng/dL,and30U/mL,referencerate0–37, respectively).
Accordingtothefindingsabovelaparoscopic hemicolec-tomywasperformedundergeneralanesthesiainalithotomy positiontiltedtotherightandwithhisheaddown.The sur-geonandthesecondassistantweresituatedattherightsideof thepatientandthefirstassistantwaspositionedontheleft, whichare oppositethepositionsusedforanormalpatient. Pneumoperitoneumwasestablishedaboveumbilicususinga Hassontrocar(12mmopticaltrocar)forthecamerainserted byopentechniqueunderdirectvision.Trocarswereplacedin amirrormannerincluding a12mmtrocarintherightiliac
Fig.1–ChestX-rayshoweddextrocardiaandright-sided gastricairbubble.
Fig.3–Placementoftrocarsforlaparoscopicright hemicolectomyinpatientswithsitusinversustotalis.
fossaanda5mmtrocarintheleftiliacfossafortheoperator, anda5mmtrocarintheleftflantusedbythefirstassistant forsuction,irrigationandtraction(Fig.3).
Laparoscopicexplorationoftheabdominalcavitywas car-riesouttoallowvisualizationoftheliverlocatedontheleft and the stomachand the spleenon the right demonstrat-ingSIT.Othersmalformationswerenotfound.Theappendix, cecalandthecolonicmassintheascendingcolonwere iden-tifiedintheleftsideofabdominalcavity(Fig.4).
Themesentery was incised caudal to the ileocolic ves-sels. A mesentericwindow below the vessels was created searchingthesecond part ofduodenum. Theileocolic ves-selsweredividedatitsrootaftersuperiormesentericvessels wereexposedandradicallymphadenectomyaroundthisarea
Fig.4–Laparoscopicviewidentifyingcolonicmassinthe ascendingcolonlocatedontheleftofabdominalcavity.
wasperformed.Dissectionofthelymphnodescontinuedup totherootofthemiddlecolicarteryandtheleftbranchof thisarterywasdivided.Acarefulmobilizationofthe ascend-ingcolonincludingtumorwasperformedalongToldt’sfascia mediallytolaterallytoavoidbleeding.
Throughaleftsubcostalincisionthebowelwasextracted. The reconstruction was carried out extracorporeally and a side-to-sidefunctional anastomosisbetweentheileumand transverse colon was performed using a stapling method. Totaloperatingtimewas120min,thebloodlosswaslessthan 100mLandthepatientwasdischargedonthe6thdayafter theoperationwithoutcomplications.
Histologicexaminationoftheresectedspecimenshowed awell-differentiatedadenocarcinomawithserosalinvasion, no metastasistothe sixtyisolated lymphnodes and with-outvenous,lymphaticandperineuralinvasion(pT3N0).2The
patientdidnotreceiveadjuvanttreatmentandheisdoingwell withoutrecurrencesixmonthsaftercolectomy.
Discussion
SITwasfirstdescribedin1600byFabricius.3SITreferstoa
completeinversionofallthethoracicandabdominalorgans challengingtheleftandrightaspectsofthecavitiesand result-inginuncommonview.Laparoscopicsurgeryforcoloncancer inSITmay bemoredifficultbut saferprocedureshouldbe performedcarefully.
SITitselfhasnopathophysiologicsignificanceandgenetic predisposition has been established.4 In this case, several
membersofpatient’sfamilypresentthisconditionsuggesting geneticpredisposition.Cardiacandintestinalmalformations aswellasothercongenitalanomaliescanbeassociatedwith SIT.5CaseswithSITanasplenia,polysplenia,biliaryatresiaor
intestinalmalrotationhavebeenreported.6Thiscaseisnot
associatedwithothermalformations.
SIT itself isnota premalignantcondition. In the litera-turereviewmorethan50casesofneoplasiasinpatientswith SIhavebeendescribed untilnowadays.6–9 Therehavebeen
publishedseveralcasesofSITassociatedwithsynchronous andmetachronousmultiplegastrointestinalmalignancies.10
Inthegeneralpopulation,theincidenceofsynchronousand metachronouscoloncancerrangesfrom3to8%andfrom0.5 to3.6%respectively,andtheseincidencesdonotseemtobe higher inpatients withSIT.11 Thediagnosis ofmalignancy
inpatient withSImay besporadicbut someauthors have proposed ahypothesisthat defendsapossiblerelationship betweenunidentifiedgenesaffectingleft-rightaxis arrange-mentandgenesrelatedtocancersusceptibility.12
MostcasesofSITaredetectedduringmedicalcheck-ups using chest radiograph. Careful preoperative study is very important inthese cases.13 Apart from standard
examina-tion duringa staging workup forcolon cancer in which a chestradiograph,laboratoriesstudiesandthoracoabdominal computed tomographyare included,patientswithSITwho underwent surgery,neededanechocardiographytoidentify cardiacvalvularpathologyorcardiacmalformation.14
Table1–WorldwidepublicationsaboutlaparoscopiccolectomyforcoloncancerinpatientswithSIT.
Author Year Location Diagnosisof SITinthe childhood
Other malfor-mations
Complications Bloodloss (ml) Operating time(min) Discgarge (postoperative day)
Fujiwaraetal.13 2007 Ascending
colon
Yes No None 60 191 10th
KimWKetal.10 2011 Transverse
andsigmoid colon
No No None – – 18th
KimHJetal.16 2011 Ascending
colon
No No None Minimal 119 7th
SumiYetal.17 2013 Transverse
colon
Yes No None 230 402 16th
YaegashiMetal.18 2015 Sigmoid
colon
Yes No None 13 189 7th
Presentcase 2016 Ascending
colon
Yes No None 100 120 6th
examination.Literaturereportsindicatethattherewerenot moreadverseeventsduringcolonocospyinpatientswithSI but someauthors havefoundaprolonged cecalintubation time.15
SITandcolorectalcancermaybecomeeasilydetectedwith currentradiologicandendoscopicmethodsofdiagnosisbut otherunexpectedanomaliescouldarise duringsurgery.For thisreason,surgicaltechniques,especiallylaparoscopic pro-cedures,aremoredifficultandcomplexandadetailedplanis neededforsuccessfulsurgicaltreatment.
Only five laparoscopic procedures for colon cancer in patients with SIT have been published in the English literature10,13,16–18 (Table1).Principlesofradicalresectionof
thecancerandaccompanyingdissectionofthelymphnodes were preserved. Authors emphasize the importance of an exhaustive preoperative study and a detailed planning of laparoscopicsurgeryincludingpositionsofoperatorand assis-tants,trocarsitesandacarefulsurgicaltechniquetobeaware ofanatomic challenges.Fourpatientshavebeen diagnosed withSITinthechildhood.Theywerenotfoundwithanyother malformations.Nocomplicationshavebeenreported.Blood losswasminimal,totaloperatingtimeandthehospitalstay werecomparablewiththatofpatientswithordinary anatom-icalpositions.
Thetrocar siteshave to becarefully considered forSIT patients.16–19 We proposed the use of four trocars to
per-formlaparoscopicrighthemicolectomy.Inthepresentcase, the surgeon was situated at the right side of the patient, opposite the usual side for surgery, the 12mmtrocar was placed at the right iliac fossa for surgeon’s right hand and the 5mm trocar was placed at the right flank for her left hand. We began by identifying and dividing the ileocolic vessels and then continued with the dissection mobilization of the ascending colon including tumor that wascarriedoutmediallytolaterallytomaketheprocedure morefeasible.Someauthorsproposethataleft-handed sur-geon may have a technical advantage during laparoscopy in patients with SIT.20 However, this condition could not
precluderight-handedsurgeonsfromperformingthe laparo-scopicprocedureinSITpatientsaccuratelybecausesurgeons have to employrightly their dominant and non-dominant hands.
Conclusion
Laparoscopic surgeryforcolon cancer inpatients withSIT couldbesafelyperformed.Acompletepreoperative evalua-tion isimportantforsuccessfulsurgicaltreatment.Because ofanatomicchallenges,laparoscopy requiresacarefulplan includingpositionsofsurgeonsandtrocarsitesaswellasa skillfultechnique.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.MayoCW,RiceRG.Situsinversustotalis:astatisticalreview ofdataon76caseswithspecialreferencetodiseaseofthe biliarytract.ArchSurg.1949;58:724–30.
2.EdgeSB,ByrdDR,ComptonCC,editors.AJCCcancerstaging manual(Colonandrectum).7ed.NewYork:Springer;2010.p. 143–64.
3.TakeiHT,MaxwellJG,ClancyTV,TinsleyEA.Laparoscopic cholecystectomyinsitusinversustotalis.JLaparoendosc Surg.1992;2:171–6.
4.GoiT,KawasakiM,YamazakiT,KoneriK,KatayamaK,Hirose K,etal.Ascendingcoloncancerwithhepaticmetastasisand cholecystolithiasisinapatientwithsitusinversustotalis withoutanyexpressionofUVRAGmRNA:reportofacase. SurgToday.2003;33:702–6.
5.UchidaH,KawamuraYJ,TakegamiK,MatsudaK,WatanabeT, MasakiT,etal.Coloncancercomplicatedbyvascularand intestinalanomaly.Hepatogastroenterology.2004;51:156–8. 6.ZhuH,YangK,HuJK.Gastrectomyforgastriccarcinomawith
situsinversustotalis:casereportandliteraturereview. Hippokratia.2015;19:360–2.
7.IwamuraT,ShibataN,HaraguchiY,HisashiY,NishikawaT, YamadaH,etal.Synchronousdoublecancerofthestomach andrectumwithsitusinversustotalisandpolysplenia syndrome.JClinGastroenterol.2001;33:148–53.
9. KynoD,KimuraY,ImamuraM,UchiyamaM,IshiiM,Meguro M,etal.Pancreaticoduodenectomyforbiliarytractcarcinoma withsitusinversustotalis:difficultiesandtechnicalnotes basedontwocases.WorldJSurgOncol.2013;11:312.
10.KimYW,RyuH,KimDS,KimIY.Doubleprimarymalignancies associatedwithcoloncancerinpatientswithsitusinversus totalis:twocasereports.WorldJSurgOncol.2011;9:109. 11.ParkU,YuCS,KimHC,JungYH,HariKR,KimJC.
Metachronouscolorectalcancer.ColorectalDis.2006;8:323–7. 12.GaliatsatosP,KasprzakL,ChongG,JassJR,FoulkesWD.
Multipleprimarymalignanciesinapatientwithsitus ambiguous.ClinGenet.2006;69:528–31.
13.FujiwaraY,FukunagaY,HigashinoM,TanimuraS,Takemura M,TanakaY,etal.Laparoscopichemicolectomyinapatient withsitusinversustotalis.WorldJGastroenterol.
2007;13:5035–7.
14.FrancisR,AdamC,DeviceW,OstrowskiL,LoC.Congenital heartdiseaseandthespecificationofleft-rightasymmetry. AmJPhysiolHeartCircPhysiol.2012;302:2102–11.
15.ChoiDH,ParkJW,KimBN,HanKS,HongCW,SohnDK,etal. Colonoscopyinsitusinversustotalispatients.AmJ Gastroenterol.2008;103:1311–2.
16.KimHJ,ChoiGS,ParkJS,LimKH,JangYS,ParkSY.
LaparoscopicrighthemicolectomywithD3lymphnode
dissectionforapatientwithsitusinversustotalis:reporta case.SurgToday.2011;41:1528–42.
17.SumiY,TomonoA,SuzukiS,KurodaD,KakejiY.Laparoscopic hemicolectomyinapatientwithsitusinversustotalisafter opendistalgastrectomy.WorldJGastroenterolSurg. 2013;5:22–6.
18.YaegashiM,KimuzaT,TakashiS,SatoT,KawasakiY,Otsuka K,etal.Laparoscopicsigmoidectomyforapatientwithsitus inversustotalis:effectofchangingoperatorposition.IntSurg. 2015;100:638–42.
19.ChoiSI,ParkSJ,KangBM,LeeKY,LeeHC,LeeSH.
Laparoscopicabdominoperinealresectionforrectalcancerin apatientwithsitusinversustotalis.SurgLaparoscEndosc PercutanTech.2011;21:87–90.