revbrashematolhemoter.2014;36(5):369–372
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
w w w . r b h h . o r g
Case
report
Quantification
of
mixed
chimerism
allows
early
therapeutic
interventions
Jóice
Merzoni
a,b,∗,
Gisele
Menezes
Ewald
b,
Alessandra
Aparecida
Paz
a,b,
Liane
Esteves
Daudt
a,b,
Luiz
Fernando
Job
Jobim
a,baUniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
bHospitaldeClínicasdePortoAlegre(HCPA),PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received7November2013
Accepted4June2014
Availableonline17July2014
Keywords:
Chimerism
Bonemarrowtransplantation
Myelodysplasticmyeloproliferative
diseases
Tandemrepeatsequences
a
b
s
t
r
a
c
t
Hematopoieticstemcelltransplantationisthecurativeoptionforpatientswith
myelodys-plasticsyndrome;however,itrequiresalongpost-transplantationfollow-up.A53-year-old
womanwithadiagnosisofmyelodysplasticsyndromeunderwentrelateddonorallogeneic
hematopoietic stem cell transplantationin July 2006. Threemonths after
transplanta-tion,acomparativeshorttandemrepeatanalysisbetweendonorandrecipientrevealed
full chimerism, indicating complete, healthy bone marrow reconstitution. Three years
and ten months after hematopoieticstem cell transplantation, the patient developed
leukopeniaandthrombocytopenia.Anothershorttandemrepeatanalysiswascarriedout
whichshowedmixedchimerism(52.62%),indicatingrelapseddisease.Adonorlymphocyte
infusionwasadministered.Thepurposeofdonorlymphocyteinfusionistoinducea
graft-versus-leukemiaeffect;infact,thisdonor’slymphocyteinfusioninducedfullchimerism.
Successiveshorttandemrepeatanalyseswereperformedaspartofpost-transplantation
follow-up,andinJuly2010,onesuchanalysisagainshowedmixedchimerism(64.25%).
Basedonthisfinding,aseconddonorlymphocyteinfusionwasadministered,butfailed
to eradicate the disease.In September 2011,the patient presented with relapsed
dis-ease, and a second related donor allogeneic hematopoietic stem cell transplantation
wasperformed.Subsequentshorttandemrepeatanalysesrevealedfullchimerism,
indi-cating complete bone marrow reconstitution. We conclude thatquantitative detection
of mixed chimerism is an importantdiagnostic tool that can guide early therapeutic
intervention.
©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published
byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:ProgramadePós-Graduac¸ãoemCiênciasCirúrgicasFAMEDeServic¸odeImunologiaHCPA,UniversidadeFederal
doRioGrandedoSul(UFRGS),RuaRamiroBarcelos,2350,RioBranco,90035-903PortoAlegre,RS,Brazil.
E-mailaddress:[email protected](J.Merzoni).
http://dx.doi.org/10.1016/j.bjhh.2014.07.004
1516-8484/©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Allrights
370
revbrashematolhemoter.2014;36(5):369–372Introduction
Hematopoieticstemcelltransplantation(HSCT)isaneffective
treatment for patients with immunological and
hemato-logicdiseases,including myelodysplasticsyndrome(MDS).1
In HSCT, the donor cells restore the recipient bone
mar-row, producing new blood cells that are responsible for
thehematopoieticandimmunological reconstitutionofthe
recipient. Consequently, HSCT results in a restoration of
hematopoiesis and in a gradual change of hematopoietic
cellgeneticsfrom therecipientprofiletothedonorprofile.
Thischangeofgeneticprofile,inwhichdonorandrecipient
hematopoieticcellscancoexist,iscalledchimerism.2
One of the methods used to verify chimerism is short
tandem repeat (STR) testing. STRs, or microsatellites, are
repetitivesequencesofthreetosevenbasepairsthat
iden-tify different alleles by the number of copies of repetitive
sequencescontainedintheDNAregionanalyzed.STRsexhibit
ahigh level ofheterozygosity, high polymorphism and are
highlyinformativeofhumanindividuality.3
ThestudyofSTRsusesthepolymerasechainreaction(PCR)
technique,whichenablestheselectiveamplificationof
spe-cificDNAsequences.TheadvantagesofPCRincludethesmall
numberofcellsrequiredforanalysisandthetechnique’shigh
sensitivity,asitisabletodetect1cellin1×106.3
Thus,theroleofSTRsasmarkersofchimerismstatusafter
HSCThasbeenusedtoguideclinicalinterventionstoachieve
successinHSCT.4
Case
report
On10November2004,a53-year-oldwomanwasdiagnosed
withMDS withanInternational PrognosticScoringSystem
(IPSS)stageofIntermediate2.Herkaryotypeatdiagnosis
fea-tureddeletions ofchromosomes 1and 6. Thepatient was
referredforrelateddonorHSCT(identicalHLAsibling–Donor
#1)asatherapeuticoptionduetothehighriskof
transfor-mationtoacutemyeloidleukemia(AML). PriortoHSCT,an
analysisof the STRprofiles of 15 lociand the amelogenin
locuswasconductedindonorand recipientblood samples
toenablefollow-upofthechangesingeneticprofilein
recip-ienthematopoieticcellswhichwouldsignalreconstitutionof
hematopoiesisandengraftment.STRanalysiswasperformed
bymultiplexPCRandthedetectionofthePCRproductswas
performedinanABI3100AvantGeneticAnalyzerwiththe
Identifilerkit(AppliedBiosystems®).4
Thepre-transplantationconditioningregimenconsistedof
busulfanandcyclophosphamide,withthe HSCTbeing
per-formedinJuly2006with2.4×106CD34+cells/kg.Thepatient
did not develop acute graft-versus-host disease (GVHD).
EngraftmentoccurredatDay+26asevaluatedbybloodcount
andbonemarrowaspiration.ThreemonthsaftertheHSCT,
afollow-up STRanalysis revealed fullchimerism; inother
words,thegeneticprofileintherecipient’sbloodsamplewas
identicaltothedonorprofile,indicatingfullengraftment
with-outmolecularevidenceofdiseaserecurrence.
InApril2010,threeyearsandtenmonthsaftertheHSCT,
the patient developed leukopenia and thrombocytopenia.
Another STRanalysiswasperformedwhich showedmixed
chimerism (donorand receptor cellscoexisting), indicating
relapse ofthedisease.Chimerismwasquantifiedusingthe
area underthecurvepeaks oftheelectropherogram asper
Kristtetal.4usingfiveinformativelociofSTRsandtheresult
was52.62%donorchimerism.
To halt disease progression, a donor lymphocyte
infu-sion (DLI) was performed with the objective of inducinga
graft-versus-leukemia (GVL) reaction. The patient received
1×107CD3+cells/kg.Twomonthsaftertheinfusion,inJune
2010,thepatientagainpresentedfullchimerism,indicating
thattheDLIwaseffective.
Afurtherfollow-upwas performedbyblood countsand
bonemarrowaspiration.Thepatientremainedclinically
sta-bleandwithoutclinicalorhematologicalevidenceofrelapse
until July 2010, when STR analysis showed 64.25% donor
chimerism. Basedon these results, a second DLI was
per-formedinanattempttoinduceanearlyGVLresponseand
preventamajorrecurrence.STRanalysisperformedafterthis
DLI, in September 2010,revealed 51.20% donor chimerism,
indicating the persistence of this phenomenon. Although
mixed chimerismpersisted,the patientremainedclinically
stableandthetherapeuticoptionswereevaluated.
In August 2011,the patientdeveloped pancytopenia.As
shehad anotherHLA-identicalsibling(Donor#2), asecond
HSCTwasperformedon23September2011.Theconditioning
regimenconsistedofbusulfanandmelphalan,andtheHSCT
was performed withan infusionof 1.6×106CD34+cells/kg.
EngraftmentoccurredatDay+19asevaluatedbybloodcounts
and bone marrow aspiration. The patient was tested for
chimerisminOctober2011,January2012,September2012and
September 2013.All investigationsrevealed fullchimerism,
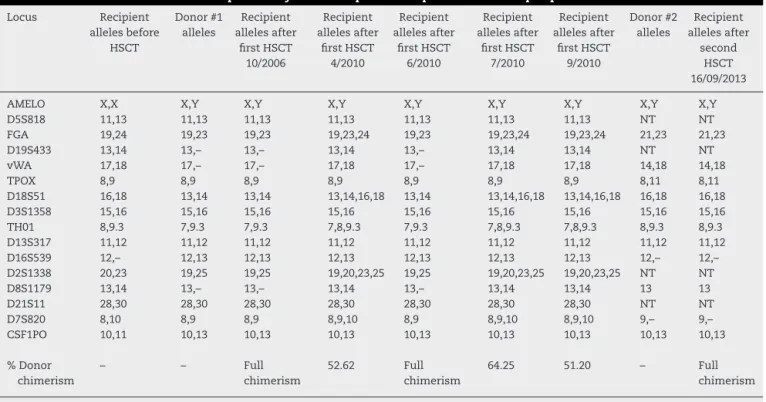
indicatingcompletebonemarrowrecovery.Resultsare
sum-marizedinTable1.
Discussion
Oneofthemostwidelyusedparametersformonitoringinthe
post-HSCTperiodisthedonor:recipientDNAratio.This
con-ditionisestimatedandexpressedasthepercentageofdonor
chimerism. A value approaching 100% indicates a greater
numberofdonorcellsintheanalyzedsample.AfterHSCT,the
optimalgoalis100%donorchimerism.Whenthisconditionis
achieved,itisknownas‘fullchimerism’.4
Informativelociwereusedforcalculationpurposes,which
was performed by measuring the area under the curve
of the peaks on an electropherogram. The formula was
(D1+D2/D1+D2+R1+R2)×100,whereD1,D2,R1andR2
rep-resenttheareaunderthecurveofrecipientanddonoralleles.4
After the first HSCT, the FGA, TH01, D2S1338, D7S820 and
D18S51lociwereusedtocalculatemixedchimerism,because
theywereinformativeloci.Thecalculatedcoefficientof
vari-ationwas<10%.TheseresultsareconsistentwiththeKristt
etal.acceptancecriteria.5
ItiswellknownthatthesuccessofHSCTdepends,inpart,
ontheGVLeffectinducedbythedonorTlymphocytes.The
GVLeffectplaysanimportantroleindiseaseeradicationin
patientswithhematologicmalignancytreatedbyHSCT.1 In
revbrashematolhemoter.2014;36(5):369–372
371
Table1–Resultsofshorttandemrepeatanalysisinsamplesofrecipientanddonorperipheralblood.
Locus Recipient allelesbefore HSCT Donor#1 alleles Recipient allelesafter firstHSCT 10/2006 Recipient allelesafter firstHSCT 4/2010 Recipient allelesafter firstHSCT 6/2010 Recipient allelesafter firstHSCT 7/2010 Recipient allelesafter firstHSCT 9/2010 Donor#2 alleles Recipient allelesafter second HSCT 16/09/2013
AMELO X,X X,Y X,Y X,Y X,Y X,Y X,Y X,Y X,Y
D5S818 11,13 11,13 11,13 11,13 11,13 11,13 11,13 NT NT
FGA 19,24 19,23 19,23 19,23,24 19,23 19,23,24 19,23,24 21,23 21,23
D19S433 13,14 13,– 13,– 13,14 13,– 13,14 13,14 NT NT
vWA 17,18 17,– 17,– 17,18 17,– 17,18 17,18 14,18 14,18
TPOX 8,9 8,9 8,9 8,9 8,9 8,9 8,9 8,11 8,11
D18S51 16,18 13,14 13,14 13,14,16,18 13,14 13,14,16,18 13,14,16,18 16,18 16,18
D3S1358 15,16 15,16 15,16 15,16 15,16 15,16 15,16 15,16 15,16
TH01 8,9.3 7,9.3 7,9.3 7,8,9.3 7,9.3 7,8,9.3 7,8,9.3 8,9.3 8,9.3
D13S317 11,12 11,12 11,12 11,12 11,12 11,12 11,12 11,12 11,12
D16S539 12,– 12,13 12,13 12,13 12,13 12,13 12,13 12,– 12,–
D2S1338 20,23 19,25 19,25 19,20,23,25 19,25 19,20,23,25 19,20,23,25 NT NT
D8S1179 13,14 13,– 13,– 13,14 13,– 13,14 13,14 13 13
D21S11 28,30 28,30 28,30 28,30 28,30 28,30 28,30 NT NT
D7S820 8,10 8,9 8,9 8,9,10 8,9 8,9,10 8,9,10 9,– 9,–
CSF1PO 10,11 10,13 10,13 10,13 10,13 10,13 10,13 10,13 10,13
%Donor chimerism
– – Full
chimerism
52.62 Full
chimerism
64.25 51.20 – Full
chimerism
HSCT:hematopoieticstemcelltransplantation;NT:nottested.
aGVL responsecapable ofinhibiting the dysplastic clones thathadresisted theconditioning andfollow-up regimens. AdministeringaDLIonthebasisofbloodcounts,bone mar-row aspiration,and karyotype findings alone could expose thepatienttoanunnecessaryriskofGVHD.Mixedchimerism quantificationenablescorrecttreatment decisions,such as performingDLIsonlywhenadequateandnecessary. Admin-istrationofaDLItopatientswithdonorchimerism≥40%is stronglyassociatedwithconversiontofullchimerism.Inthis case,thebenefitoftheDLIwouldbesignificantlysuperiorto theriskofdevelopingGVHD.6 Therefore,theimportanceof
mixedchimerismquantificationasatooltosupportadequate,
correct,andearlytreatmentdecisionscannotbeoverstated.
ThesecondDLIadministeredtoourpatientfailedtoinduce
fullchimerism, whichsuggeststhat thisDLIwasunableto
achievemaximumantitumoreffectandthuseradicatethe
dis-ease.Campregheretal.foundthatpatientswithMDS with
high-risk IPSS stages treated with DLI have better results
thanpatients withintermediateIPSS.These authors found
that the major response to the DLI observed in patients
withMDSand high-riskIPSSisduetothehigh expression
of tumor-associated antigens in these patients. This high
antigenexpressionmaymaketheneoplasticclonemore
sus-ceptibletoimmuneattackbytheDLI.7
Inthepresentcase,administrationofDLIstoapatientwith
IPSSIntermediate-2MDSdidnotseemtoproducealong-term
result,but theseDLIswere abletoinducecomplete
remis-sion,withlowriskofmortalityattimeswhenfewtherapeutic
optionswereavailable.Thequantificationofmixedchimerism
contributedtothedecisiontoperformasecondHSCTusing
anothersiblingasdonor.Atthetimeofwriting,thepatient
wasclinicallystable,transfusion-independent,and without
anyclinicalcomplications.
Inthiscase,STRanalysisthroughmultiplexPCRfollowed
bydetectioninageneticanalyzerallowedearlyclinical
inter-vention and contributed decisively to post-transplantation
therapy.Mixedchimerismquantificationwasof
fundamen-talimportancetosupportdecisionsaboutDLIadministration.
Inconclusion,quantitativefollow-upofthechimerism
pro-fileafterHSCTisavaluablediagnostictoolthatenablesearly
interventioninthepost-transplantationperiod.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HiramotoN,KurosawaS,TajimaK,OkinakaK,TadaK, KobayashiY,etal.Positiveimpactofchronicgraft-versus-host diseaseontheoutcomeofpatientswithdenovo
myelodysplasticsyndromeafterallogeneichematopoieticcell transplantation:asingle-centeranalysisof115patients.EurJ Haematol.2014;92(2):137–46.
2.PopeS,ChapmanH,LambertJ.Theeffectofbonemarrow transplantsonDNAprofiles:acaseexample.SciJustice. 2006;46(4):231–7.
3.GrubicZ,StinglK,Cecuk-JelicicE,ZunecR,ServentiSeiwerth R,LabarB,etal.Evaluationofmixedchimerisminbone marrowtransplantationprograminCroatia.TransplantProc. 2005;37(2):1388–91.
372
revbrashematolhemoter.2014;36(5):369–3725.KristtD,KleinT.Reliabilityofquantitativechimerismresults: assessmentofsampleperformanceusingnovelparameters. Leukemia.2006;20(6):1169–72.
6.DeyBR,McAfeeS,ColbyC,SacksteinR,SaidmanS,TarbellN, etal.Impactofprophylacticdonorleukocyteinfusionson mixedchimerism,graft-versus-hostdisease,andantitumor responseinpatientswithadvancedhematologicmalignancies
treatedwithnonmyeloablativeconditioningandallogeneic bonemarrowtransplantation.BiolBloodMarrowTransplant. 2003;9(5):320–9.