Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
w w w . r b h h . o r g
Review
article
Influence
of
cyclosporine
on
the
occurrence
of
nephrotoxicity
after
allogeneic
hematopoietic
stem
cell
transplantation:
a
systematic
review
Juliana
Bastoni
da
Silva
a,b,∗,
Maria
Helena
de
Melo
Lima
b,
Sílvia
Regina
Secoli
aaUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
bUniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11September2013
Accepted14January2014
Availableonline3April2014
Keywords:
Stemcelltransplantation
Bonemarrowtransplantation
Cyclosporine
Acutekidneyinjury
Toxicity
a
b
s
t
r
a
c
t
Cyclosporine, adrugusedinimmunosuppressionprotocolsforhematopoieticstemcell
transplantationthathasanarrowtherapeuticindex,maycausevariousadversereactions,
includingnephrotoxicity.Thishasadirectclinicalimpactonthepatient.Thisstudyaims
tosummarizeavailableevidenceinthescientificliteratureontheuseofcyclosporinein
respecttoitsriskfactorforthedevelopmentofnephrotoxicityinpatientssubmittedto
hematopoieticstemcelltransplantation.Asystematicreviewwasmadewiththe
follow-ingelectronicdatabases:PubMed,WebofScience,Embase,Scopus,CINAHL,LILACS,SciELO
andCochraneBVS.Thekeywordsusedwere:“bonemarrowtransplantation”OR“stemcell
transplantation”OR“grafting,bonemarrow”ANDcyclosporineORcyclosporinOR“risk
fac-tors”AND“acutekidneyinjury”OR“acutekidneyinjuries”OR“acuterenalfailure”OR“acute
renalfailures”OR“nephrotoxicity”.Thelevelofscientificevidenceofthestudieswas
clas-sifiedaccordingtotheOxfordCentreforEvidenceBasedMedicine.Thefinalsamplewas
composedof19studies,mostofwhich(89.5%)hadanobservationaldesign,evidencelevel
2Bandpointedtoanincidenceofnephrotoxicityabove30%.Theavailableevidence,
con-sideredasgoodqualityandappropriatefortheanalyzedevent,indicatesthatcyclosporine
representsariskfactorfortheoccurrenceofnephrotoxicity,particularlywhencombined
withamphotericinBoraminoglycosides,agentscommonlyusedinhematopoieticstemcell
transplantationrecipients.
©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published
byElsevierEditoraLtda.Allrightsreserved.
Introduction
Cyclosporineisanessentialdruginthetherapeuticregimen
ofallogeneichematopoieticstemcelltransplantation(HSCT)
∗ Correspondingauthorat:RuaTessáliaVieiradeCamargo,126,UniversidadeEstadualdeCampinas–UNICAMP,13084-971Campinas,SP,
Brazil.
E-mailaddress:[email protected](J.B.daSilva).
recipients. Itmainlyactson Tcells,suppressingtheir
acti-vationanddecreasingthereleaseoflymphokines.1,2Onthe
otherhand,cyclosporineadministrationdemandssystematic
andregular serumlevelmonitoringas,beingasubstrateof
the cytochrome P450enzymesystem, it presentsa narrow
http://dx.doi.org/10.1016/j.bjhh.2014.03.010
1516-8484/©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Allrights
therapeuticindexandisinvolvedindruginteractionsand
rel-evantadversereactions.3,4Theadditionand/orinterruptionof
otherco-administereddrugsmayaffectcyclosporineserum
levels, sincetheymaysuppress or inducethe cyclosporine
metabolismor the metabolism ofits metabolites, possibly
causingineffectivetherapyorincreasedtoxicity,particularly
nephrotoxicity.5
Although the epidemiology of nephrotoxicity in HSCT
varieswidely(from14% to73%),it isimportantduetothe
clinicimpactofthe resulting adverseeffects.6–8 The
varia-tion inincidence can beexplainedby differences between
studiesregardingpatientfollow-up,typeofconditioning
reg-imen,the presenceof hypertensionpriorto HSCT,hepatic
sinusoidalobstructionsyndrome,amphotericinBusageand
other nephrotoxic drugs, aswell as the differences in the
criteriausedforthedefinitionofnephrotoxicity.9–11However,
independentofriskfactors,nephrotoxicityaffectsHSCT
recip-ients,worseningtheirclinicalcondition.
StudieshaveshownthatthenephrotoxicityinHSCT
recip-ientsrepresentsarelevantriskfactorforthedevelopmentof
chronickidneyinjury.Ithasbeenassociatedwithincreases
inbothshort-termandlong-termmortalityandmayaffect
around 70% of patients.6,10 Considering the importance of
cyclosporineforthesuccessofHSCT,itsnephrotoxicpotential
andthelackofstudiesthataddressthisresearchquestion,the
purposeofthecurrentstudywastoaccumulatetheevidence
availableinthescientificliteratureaboutcyclosporineusage
asariskfactorforthedevelopmentofnephrotoxicityinHSCT
recipients.
Method
Asearchforarticleswasperformedwiththefollowing
elec-tronicdatabases:PubMed,WebofScience,Embase,Scopus,
CINAHL, LILACS, SciELO and Cochrane BVS, without
lim-its on time. Keyword selection was based on the PICO12
strategy. Thus, the included keywords were “bone marrow
transplantation” OR “stem cell transplantation” OR
“graft-ing, bone marrow” for patient (P) AND “cyclosporine” OR
“cyclosporin”OR“riskfactors”forintervention(I)AND“acute
kidneyinjury”OR“acutekidneyinjuries”OR“acuterenal
fail-ure”OR“acuterenalfailures”OR“nephrotoxicity”foroutcome
(O).
Theinclusioncriteriaofthestudywere:articlespublished
inPortuguese,EnglishorSpanish,withsummariesavailable
indatabases,whichreferencedcyclosporineusageand
nep-hrotoxicityinHSCTrecipients.Studiesconcerningpediatric
populations,editorials,lettersandreviewswereexcluded.The
systematicreviewwascompletedinDecember2012.
Articles were selected by two authors separately and,
in case ofdisagreement, a third author reviewedthem to
decideaboutinclusion.Uponsearching,countlesstermswere
observedrelated tonephrotoxicity, suchaskidney toxicity,
kidneydysfunction,acuterenalfailure(ARF)andacute
kid-neyinjury (AKI).InspiteofAKI beingthe mostcommonly
usedterminrecentstudies,inthissystematicreviewtheterm
“nephrotoxicity”wasconsideredmoreappropriatetoanalyze
adversedrugevents.
At the outset, 746 articles were found that were
trans-ferred to Endnote® Web.13 This program identified 184
duplicate articles, with 562 publications remaining. After
reading thetitlesandabstracts, 518articleswere excluded.
The remaining 44 articles were evaluated by reading in
full and another 25 were excluded for the following
rea-sons:twowerehistologicalstudiesandcyclosporinewasnot
investigatedasanindependentvariableofprobablerisk
fac-tor for nephrotoxicity in HSCT recipients in the other 23
articles.
Thus,19studieswereincludedinthisresearchandwere
summarized based on:the identification ofthe article, the
databasewhereitwasfound,thestudiedpopulation,study
design, patient characteristics, incidenceof nephrotoxicity,
intervention (cyclosporine,dosage, routes, usagetime) and
nephrotoxicity-relatedfactors.
On reading thetexts infull,the articleswere evaluated
usingtheStrengtheningtheReportingofObservational
Stud-iesinEpidemiology(STROBE)technique.14Althoughthisisnot
atooltoevaluatethequalityofanarticle’smethodology, it
presentsimportantaspectsregardingfeaturesofthe
method-ology considered relevant for this research, which are: (A)
context:placedescription,relevantdatesincludingrecruiting
time,exposure,follow-upandcollecteddata;(B)participants:
eligibilitycriteria, selectionmethodofparticipants; and(C)
datasource/measurement:datasourceanddetailed
evalua-tionmethods.Incaseswheredatawerelacking,thearticlewas
excluded.ThedataonthearticlesweresavedonaMicrosoft
Excel®worksheetandclassifiedbasedonthelevelofscientific
evidence,accordingtotheOxfordCentreforEvidenceBased
Medicine.15,16
Results
MostofthepublicationswereidentifiedinPubMed(84.2%)and
presentedanobservationalmethodologicaldesignand
non-probabilistic sample (89.5%) on patients undergoing HSCT,
withfollow-upsequaltoorgreaterthan100days(52.6%).All
thestudiespresentedlevel2Bscientificevidence.
Themedianageofsubjectsofthestudiesrangedfrom18
to52yearsandthemeanagewasbetween25and56.5years.
There wasapredominance ofmyeloablativetherapy(79%),
andadiagnosisofleukemia(100%)orlymphoma(57.9%).More
thanhalfthestudies(52.6%)presentedthetermsARForAKIto
definenephrotoxicity,whicharethepredominanttermsafter
2000.
The cyclosporine dose varied from 2.5 to 5mg/kg/day
by intravenous administration, with a subsequent switch
to peroral administration. The oraldose ranged from 5to
12.5mg/kg/dayforthreetosixmonths.Mostofthestudies
(89.5%)showedagreaterthan30%incidenceofnephrotoxicity
and cyclosporine appeared as a risk factor for
nephrotox-icity in around one-third of the studies (31.6%)associated
with amphotericin B and/or aminoglycoside. Cyclosporine
was used as an immunosuppressive agent monotherapy
in 52.6% of the studies. In the others, it was associated
with different immunosuppressants suchas methotrexate,
prednisone, cyclophosphamide and mycophenolate mofetil
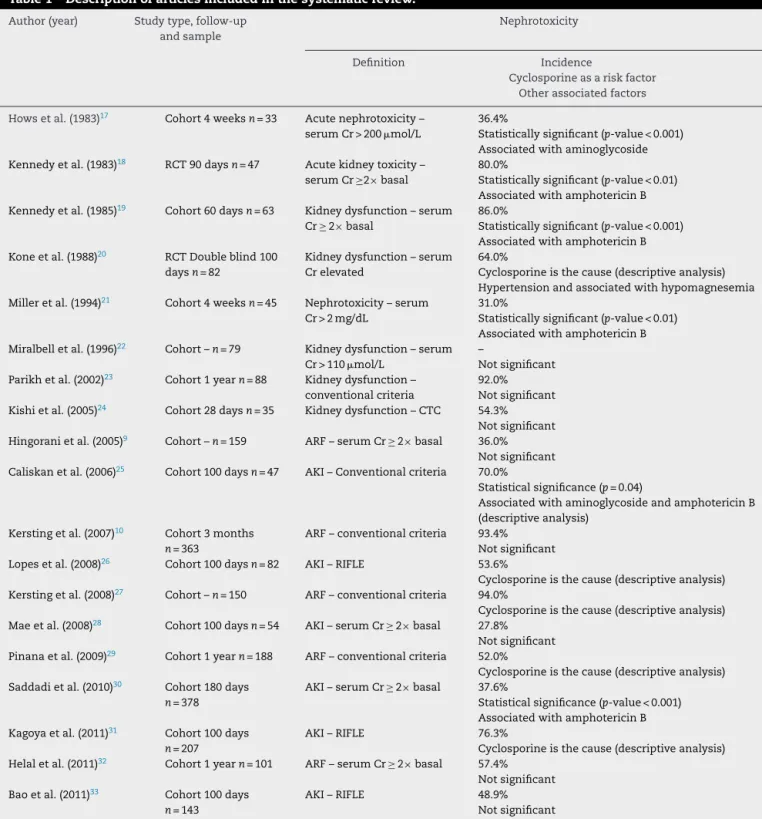
Table1–Descriptionofarticlesincludedinthesystematicreview.
Author(year) Studytype,follow-up andsample
Nephrotoxicity
Definition Incidence
Cyclosporineasariskfactor Otherassociatedfactors
Howsetal.(1983)17 Cohort4weeksn=33 Acutenephrotoxicity– serumCr>200mol/L
36.4%
Statisticallysignificant(p-value<0.001) Associatedwithaminoglycoside Kennedyetal.(1983)18 RCT90daysn=47 Acutekidneytoxicity–
serumCr ≥2× basal
80.0%
Statisticallysignificant(p-value<0.01) AssociatedwithamphotericinB Kennedyetal.(1985)19 Cohort60daysn=63 Kidneydysfunction–serum
Cr≥ 2× basal
86.0%
Statisticallysignificant(p-value<0.001) AssociatedwithamphotericinB Koneetal.(1988)20 RCTDoubleblind100
daysn=82
Kidneydysfunction–serum Crelevated
64.0%
Cyclosporineisthecause(descriptiveanalysis) Hypertensionandassociatedwithhypomagnesemia Milleretal.(1994)21 Cohort4weeksn=45 Nephrotoxicity–serum
Cr>2mg/dL
31.0%
Statisticallysignificant(p-value<0.01) AssociatedwithamphotericinB Miralbelletal.(1996)22 Cohort–n=79 Kidneydysfunction–serum
Cr>110mol/L
–
Notsignificant Parikhetal.(2002)23 Cohort1yearn=88 Kidneydysfunction–
conventionalcriteria
92.0% Notsignificant Kishietal.(2005)24 Cohort28daysn=35 Kidneydysfunction–CTC 54.3%
Notsignificant Hingoranietal.(2005)9 Cohort–n=159 ARF–serumCr≥ 2× basal 36.0%
Notsignificant Caliskanetal.(2006)25 Cohort100daysn=47 AKI–Conventionalcriteria 70.0%
Statisticalsignificance(p=0.04)
AssociatedwithaminoglycosideandamphotericinB (descriptiveanalysis)
Kerstingetal.(2007)10 Cohort3months n=363
ARF–conventionalcriteria 93.4% Notsignificant Lopesetal.(2008)26 Cohort100daysn=82 AKI–RIFLE 53.6%
Cyclosporineisthecause(descriptiveanalysis) Kerstingetal.(2008)27 Cohort–n=150 ARF–conventionalcriteria 94.0%
Cyclosporineisthecause(descriptiveanalysis) Maeetal.(2008)28 Cohort100daysn=54 AKI–serumCr≥ 2× basal 27.8%
Notsignificant Pinanaetal.(2009)29 Cohort1yearn=188 ARF–conventionalcriteria 52.0%
Cyclosporineisthecause(descriptiveanalysis) Saddadietal.(2010)30 Cohort180days
n=378
AKI–serumCr≥ 2× basal 37.6%
Statisticalsignificance(p-value<0.001) AssociatedwithamphotericinB Kagoyaetal.(2011)31 Cohort100days
n=207
AKI–RIFLE 76.3%
Cyclosporineisthecause(descriptiveanalysis) Helaletal.(2011)32 Cohort1yearn=101 ARF–serumCr≥ 2× basal 57.4%
Notsignificant Baoetal.(2011)33 Cohort100days
n=143
AKI–RIFLE 48.9%
Notsignificant
RCT:randomizedclinicaltrials;Cr:creatinine;CTC:commontoxicitycriteria;ARF:acuterenalfailure;AKI:acutekidneyinjury;RIFLE:risk, injury,failure,lossandend-stagekidneydisease.
Discussion
Theevidencefrom thisresearchsuggeststhatcyclosporine
representsariskfactorforthedevelopmentofnephrotoxicity
inHSCTrecipients,17–19,21,25,30 inthe contextofcontinuous
usageandincreasingserumlevels17,19ofcyclosporine,17–19,34
with the co-administration of amphotericin B18,19,21,25,30
and/oraminoglycosideantibiotics.17,25
Therewasapredominanceofcohortstudies,9,10,17,19,21–33
which were classifiedaccording totheir scientificevidence
as level2B. Inother words, theyare trustworthyand good
quality studies;thus,it ishighlyunlikely that newstudies
canshowsubstantialchangesregardingeffects.15,16Although
theobservationalmethodologicaldesigndoesnotrepresent
thehighestlevelofscientificevidence,itbringsinformation
aboutcyclosporineusagebydifferentpatientgroupsand
proposingimportantfindingsoneventsoftoxicity,especially
thoseatlowfrequencythatarenottypicallyidentifiedin
clin-icaltrials.
Ingeneral,patientfollow-upsweregreaterthanorequal
to100days.20,23,25,26,28–33Thisisexpectedsincethesepatients
generallypresentrisksforacutecomplicationsand
mortal-itywithinthistimeframe.Moreover,theliteraturesuggests
thatthefirst 100dayspost-transplantisa“cutoff”forthe
occurrenceofnephrotoxicity,6,35theobjectofanalysisinthis
systematicreview.
Morethanhalf (52.6%)ofthe includedpapersusedARF
orAKItodefinenephrotoxicity. Asmentioned,theseterms
became predominant after 2000. The variety of terms for
definingnephrotoxicitycanbeexplainedbytheadditionof
different diagnostic criteria in 1980. One criterion of
nep-hrotoxicity that has become common is serum creatinine
levelequaltoor greater thandoublethe patient’s baseline
value.9,17,19,21,30,32,36
Thepredominantconditioningregimenwasmyeloablative
(79%),theintensityofwhichcausestotaloralmosttotalbone
marrowcelldestructionintherecipient,ingeneral,through
highdosesofchemotherapy.37Patientsundergoing
myeloab-lativeconditioning,onthewhole,presentedameanormedian
ageunder50yearsandtheregimenwasnotanindependent
variablefornephrotoxicity.
Almostallstudies(89.5%)indicatedanincidenceof
nep-hrotoxicityofmorethan30%.9,10,17–21,23–27,29–33Inotherwords,
nearlyone-third ofpatients undergoingHSCTand exposed
tocyclosporineatdoses from5.0to12.5mg/kg/daybyoral
administrationdevelopedsomesortofkidney dysfunction.
Cyclosporinewasconsideredariskfactorfornephrotoxicity
in31.6%oftheinvestigations.17–19,21,25,30
Inthestudieswhichindicatedsomeassociationbetween
cyclosporine and nephrotoxicity, synergism between
dif-ferent nephrotoxic agents – cyclosporine, amphotericin
B and/or aminoglycosides – was observed.17–19,21,25,30 The
complex pharmacotherapy in patients undergoing HSCT,
which includes not only a large number of drugs with
interactive potential, but also combinations of agents
with similar adverse reaction profiles, enhances the toxic
effects.19,21,25,30,38 In this case, it is well known that
cyclosporine,aminoglycosidesandamphotericinBmaycause
acute tubular necrosis. This dysfunction can appear in
patientsundergoingmonotherapy,but,overall,itisworsened
bythesecombinations(toxicsynergism).39
Thestudiesindicateacorrelationbetweennephrotoxicity
andincreasedserumcreatininelevelsaswellascyclosporine
level.17,18 One of them clearly demonstrated a correlation
betweenserumlevelsofcyclosporine,creatinineandurea(p
-value<0.001);inonefractionofthesample,theriseinserum
cyclosporineprecededanincreaseincreatinine.Anotherrisk
factor for acute nephrotoxicity with cyclosporine therapy
wasthesimultaneoususe ofaminoglycosideantibiotics(p
-value=0.01).Cyclosporinelevelsoflessthan400ng/mLwere
notseentocauseseriousacutenephrotoxicity.17
Anotherinvestigationcomparedagroupofpatientswho
simultaneouslytookmethotrexateandamphotericinBwith
anothergroupconcurrentlytakingcyclosporineand
ampho-tericin B; the group treated with cyclosporine presented a
higher incidence of nephrotoxicity (80%) than the group
treatedwithmethotrexate(19%)(p-value<0.01).18
The cyclosporine concentrations used were associated
with nephrotoxicity in patients undergoing myeloablative
therapy. The concentrations varied from <150ng/mL to
>250ng/mL;furthermore, whenpatientspresentedaserum
cyclosporineconcentrationhigherthan250ng/mL,the
devel-opment oftoxicitywas faster. These differences relatedto
cyclosporineconcentrationwerenotexplainedbyriskfactors
suchasage,basalcreatinineorconcurrentuseofnephrotoxic
antibiotics.Itwasascertainedthatthehighestmean
concen-trationofcyclosporinewasassociatedwiththehighestriskfor
thedevelopmentofnephrotoxicity(p-value<0.001).In
addi-tion,comparingpatientswhotookamphotericinBwiththose
whohadnottakenthisantifungal,stratifiedbycyclosporine
concentration,showedthatthisdrugwasasignificant
inde-pendent risk factor for the development of nephrotoxicity
(p-value<0.01).19
In allogeneic bone marrow transplant recipients,
cyclosporine represented the most frequent cause of
nephrotoxicity. However, the authors did not observe a
correlationbetweenashortperiodofelevatedcyclosporine
concentration and creatinine clearanceover aperiod of20
days post-transplant. Nephrotoxicity was more frequent
with myeloablative allogeneic (91%) than with autologous
transplantation (52%) (p-value=0.004). Those differences
were attributed to graft-versus-host disease and
immuno-suppressive drug usage, including the toxicity caused by
cyclosporine.25 Comparing kidney dysfunction patients to
thosewithregularkidneyfunction,aunivariateanalysisdid
not indicate statistically significant differences concerning
aminoglycoside oramphotericinBuse.Nonetheless, inthe
descriptive analysis,amphotericinBcontributed to
nephro-toxicity in the group undergoing allogeneic HSCT (5%). In
the group of autologous HSCT, amphotericin B (31%) and
aminoglycoside(8%)usecontributedtonephrotoxicity.25
Inotherstudies,authorsfoundthatcyclosporinecauses
significant dose-dependent toxicity (relativerisk: 6.17; 95%
confidence: 4.03–9.43;p-value<0.001).Inadescriptive
anal-ysis,aminoglycoside(amikacin)andamphotericinBusewere
related to 14.2% and 10.3% of instances of nephrotoxicity,
respectively.30
Somestudiesconsideredcyclosporineacauseof
nephro-toxicitybasedondescriptiveanalysis.20,25,26,28,31Oneofthese
studiesinparticularindicatedthatcyclosporinewas
respon-siblefor21%ofgrade2nephrotoxicitycases.27
Thepresentsystematicreviewwaslimitedduetolackof
detailedinformationfromprimarystudies,especiallyabout
agentexposure(cyclosporine):biochemicalmethodsusedto
dosecyclosporine,thetimeintervalbetweenthelast
adminis-trationofcyclosporineandbloodcollectionforserumdosage
oftheimmunosuppressivedrug,thetypeofbiological
sam-pleusedtodosethedrug,aswellastheroutesandtimeof
cyclosporineadministration.Thesedatacouldsupportfurther
analysis.Thenephrotoxicityvaluationparameters,aswellas
theirdefinition,werequitevariable.Furthermore,almost
one-thirdofthestudiesuseddescriptiveanalysis.Hence,inspite
ofawideandsystematicsearch,thepossibilityofbiasshould
Contributiontotheclinicalcontext
Someofthestudiesinthissystematicreviewconsideredthat
nephrotoxicitycanbepreventedbyameasureofcaution
dur-ingtheuse ofcyclosporineassociatedwithamphotericinB
oraminoglycosidesintheformofcarefuladministrationand
kidney function monitoring.18,20,21 Another study32
recom-mendedthatearlyidentificationofriskfactorsforAKI,would
avoid,wheneverpossible,theexposureofmoresusceptible
patientstonephrotoxic drugsduringfollow-up.29 Therisk,
injury,failure,loss,end-stagekidneydisease(RIFLE)criteria
wereconsideredanimportanttooltostratifyHSCTrecipients
inrelationtoriskofdeath.33,40Inapreviousstudy,these
diag-nosticcriteriapresentedgoodsensitivityontheevaluationof
nephrotoxicity.
Conclusion
Theincidence ofnephrotoxicity following allogeneic HSCT
rangedfrom 27.8% to94% with cyclosporinebeing
consid-eredariskfactor forthis adverseeventinone-third ofthe
studies.Somestudies,which showanassociation between
cyclosporineandnephrotoxicity,havefoundsynergismwith
othernephrotoxicdrugssuchasamphotericinBand
amino-glycoside. Systematic monitoring of serum levels of the
administereddrugs and monitoringofthe patient’s kidney
functionareessential.Inaddition,itisindispensabletoavoid,
wheneverpossible,theassociationofcyclosporinewithother
nephrotoxicdrugs.Furthermore,itisnecessarytoinvestigate
possibleriskfactorsfornephrotoxicityineachHSCTrecipient.
Finally,consideringtheimportanceofcyclosporinetothe
suc-cessofHSCTandthatnephrotoxicityinHSCTrecipientshas
beenassociatedwithincreasedmortality,thisissuerequires
particularattention.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BorelJF,FeurerC,GublerHU,StähelinH.Biologicaleffectsof cyclosporinA:anewantilymphocyticagent.AgentsActions. 1976;6:468–75.
2. YeeGC.Pharmacokineticandpharmacodynamicstudiesof cyclosporineinbonemarrowtransplantation.Transplant Proc.1990;22:1327–30.
3. LeatherHL.Druginteractionsinthehematopoieticstemcell transplant(HSCT)recipient:whateverytransplanterneedsto know.BoneMarrowTransplant.2004;33:137–52.
4. KahanBD,KeownP,LevyGA,JohnstonA.Therapeuticdrug monitoringofimmunosuppressantdrugsinclinicalpractice. ClinTher.2002;24:330–50,discussion329.
5. YeeGC.Clinicalpharmacologyofcyclosporine.IntJRadAppl InstrumB.1990;17:729–32.
6. LopesJA,JorgeS.AcutekidneyinjuryfollowingHCT: incidence,riskfactorsandoutcome.BoneMarrow Transplant.2011;46:1399–408.
7. HosingC,NashR,McSweeneyP,MineishiS,SeiboldJ,Griffith LM,etal.Acutekidneyinjuryinpatientswithsystemic
sclerosisparticipatinginhematopoieticcelltransplantation trialsintheUnitedStates.BiolBloodMarrowTransplant. 2011;17:674–81.
8.ParikhCR,SchrierRW,StorerB,DiaconescuR,SorrorML, MarisMB,etal.ComparisonofARFaftermyeloablativeand nonmyeloablativehematopoieticcelltransplantation.AmJ KidneyDis.2005;45:502–9.
9.HingoraniSR,GuthrieK,BatchelderA,SchochG,Aboulhosn N,ManchionJ,etal.Acuterenalfailureaftermyeloablative hematopoieticcelltransplant:incidenceandriskfactors. KidneyInt.2005;67:272–7.
10.KerstingS,KoomansHA,HeneRJ,VerdonckLF.Acuterenal failureafterallogeneicmyeloablativestemcell
transplantation:retrospectiveanalysisofincidence,risk factorsandsurvival.BoneMarrowTransplant.2007;39:359–65.
11.ParikhCR,CocaSG.Acuterenalfailureinhematopoieticcell transplantation.KidneyInt.2006;69:430–5.
12.daCostaSantosCM,deMattosPimentaCA,NobreMR. ThePICOstrategyfortheresearchquestionconstructionand evidencesearch.RevLatAmEnfermagem.2007;15:
508–11.
13.ThompsonReuters.Endnote.[internet][cited2014Jan22]
Availablefrom:https://www.myendnoteweb.com/
EndNoteWeb.html?returnCode=ROUTER.Unauthorized &SrcApp=CR&Init=Yes
14.MaltaM,CardosoLO,BastosFI,MagnaniniMM,SilvaCM. STROBEinitiative:guidelinesonreportingobservational studies.RevSaudePublica.2010;44:559–65.
15.OxfordCentreforEvidenceBasedMedicine.Oxford,UK:
UniversityofOxford.[cited2013Nov9]Availablefrom:
http://www.cebm.net/
16.SeshiaSS,YoungGB.Theevidence-basedmedicineparadigm: wherearewe20yearslater?Part2.CanJNeurolSci.
2013;40:475–81.
17.HowsJM,ChippingPM,FairheadS,SmithJ,BaughanA, Gordon-SmithEC.Nephrotoxicityinbonemarrowtransplant recipientstreatedwithcyclosporinA.BrJHaematol. 1983;54:69–78.
18.KennedyMS,DeegHJ,SiegelM,CrowleyJJ,StorbR,Thomas ED.AcuterenaltoxicitywithcombineduseofamphotericinB andcyclosporineaftermarrowtransplantation.
Transplantation.1983;35:211–5.
19.KennedyMS,YeeGC,McguireTR,LeonardTM,CrowleyJJ, DeegHJ.Correlationofserumcyclosporineconcentration withrenaldysfunctioninmarrowtransplantrecipients. Transplantation.1985;40:249–53.
20.KoneBC,WheltonA,SantosG,SaralR,WatsonAJ. Hypertensionandrenaldysfunctioninbonemarrow transplantrecipients.QJMed.1988;69:985–95.
21.MillerKB,SchenkeinDP,ComenzoR,ErbanJK,FogarenT, HirschCA,etal.Adjusted-dosecontinuous-infusion cyclosporinAtopreventgraft-versus-hostdiseasefollowing allogeneicbonemarrowtransplantation.AnnHematol. 1994;68:15–20.
22.MiralbellR,BieriS,MermillodB,HelgC,SanchoG,PastoorsB, etal.Renaltoxicityafterallogeneicbonemarrow
transplantation:thecombinedeffectsoftotal-body irradiationandgraft-versus-hostdisease.JClinOncol. 1996;14:579–85.
23.ParikhCR,McSweeneyPA,KorularD,EcderT,MerouaniA, TaylorJ,etal.Renaldysfunctioninallogeneichematopoietic celltransplantation.KidneyInt.2002;62:566–73.
25.CaliskanY,BesisikSK,SarginD,EcderT.Earlyrenalinjury aftermyeloablativeallogeneicandautologoushematopoietic celltransplantation.BoneMarrowTransplant.2006;38:141–7.
26.LopesJA,Gonc¸alvesS,JorgeS,RaimundoM,ResendeL, Lourenc¸oF,etal.Contemporaryanalysisoftheinfluenceof acutekidneyinjuryafterreducedintensityconditioning haematopoieticcelltransplantationonlong-termsurvival. BoneMarrowTransplant.2008;42:619–26.
27.KerstingS,DorpSV,TheobaldM,VerdonckLF.Acuterenal failureafternonmyeloablativestemcelltransplantationin adults.BiolBloodMarrowTransplant.2008;14:125–31.
28.MaeH,OoiJ,TakahashiS,TomonariA,TsukadaN,KonumaT, etal.Earlyrenalinjuryaftermyeloablativecordblood transplantationinadults.LeukLymphoma.2008;49:538–42.
29.PinanaJL,ValcarcelD,MartinoR,BarbaP,MorenoE,SuredaA, etal.Studyofkidneyfunctionimpairmentafter
reduced-intensityconditioningallogeneichematopoietic stemcelltransplantation.Asingle-centerexperience.Biol BloodMarrowTransplant.2009;15:21–9.
30.SaddadiF,NajafiI,HakemiMS,FalaknaziK,AttariF,BaharB. Frequency,riskfactors,andoutcomeofacutekidneyinjury followingbonemarrowtransplantationatDrShariati HospitalinTehran.IranJKidneyDis.2010;4:20–6.
31.KagoyaY,KataokaK,NannyaY,KurokawaM.Pretransplant predictorsandposttransplantsequelsofacutekidneyinjury afterallogeneicstemcelltransplantation.BiolBloodMarrow Transplant.2011;17:394–400.
32.HelalI,ByzunA,RerolleJP,MorelonE,KreisH,
Bruneel-MamzerMF.Acuterenalfailurefollowingallogeneic hematopoieticcelltransplantation:incidence,outcomeand riskfactors.SaudiJKidneyDisTranspl.2011;22:437–43.
33.BaoYS,XieRJ,WangM,FengSZ,HanMZ.Anevaluationof theRIFLEcriteriaforacutekidneyinjuryaftermyeloablative allogeneichaematopoieticstemcelltransplantation.Swiss MedWkly.2011;141:w13225.
34.ShulmanH,StrikerG,DeegHJ,KennedyM,StorbR,Thomas ED.NephrotoxicityofcyclosporinAafterallogeneicmarrow transplantation:glomerularthrombosesandtubularinjury.N EnglJMed.1981;305:1392–5.
35.Nivison-SmithI,BradstockKF,SzerJ,DurrantS,DoddsA, HermannR,etal.Allogeneichaemopoieticcelltransplantsin Australia,1996–amulti-centreretrospectivecomparisonof theuseofperipheralbloodstemcellswithbonemarrow. BoneMarrowTransplant.2001;28:21–7.
36.KennedyMS,DeegHJ,StorbR,DoneyK,SullivanKM, WitherspoonRP,etal.Treatmentofacutegraft-versus-host diseaseafterallogeneicmarrowtransplantation.Randomized studycomparingcorticosteroidsandcyclosporine.AmJMed. 1985;78:978–83.
37.SchattenbergAV,LevengaTH.Differencesbetweenthe differentconditioningregimennsforallogeneicstemcell transplantation.CurrOpinOncol.2006;18:667–70.
38.FonsecaRB,SecoliSR.Drugsusedinbonemarrow
transplantation:astudyaboutcombinationsofantimicrobial potentiallyinteractives.RevEscEnfermUSP.2008;42:706–14.
39.LeeA.Reac¸õesadversasamedicamentos.2nded.Porto Alegre:Artmed;2009.p.488.