Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
w w w . r b h h . o r g
Original
article
Frequency
of
p190
and
p210
BCR-ABL
rearrangements
and
survival
in
Brazilian
adult
patients
with
acute
lymphoblastic
leukemia
Ilana
de
Franc¸a
Azevedo
∗,
Rui
Milton
Patrício
da
Silva
Júnior,
Audrey
Violeta
Martins
de
Vasconcelos,
Washington
Batista
das
Neves,
Fárida
Coeli
de
Barros
Correia
Melo,
Raul
Antônio
Morais
Melo
Fundac¸ãodeHematologiaeHemoterapiadePernambuco(HEMOPE),Recife,PE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5September2013 Accepted5June2014 Availableonline18July2014
Keywords:
Acutebiphenotypicleukemia Adult
BCR-ABL Survivalanalysis
a
b
s
t
r
a
c
t
Objective:Thisstudyinvestigatedtheoccurrenceofthep190andp210breakpointcluster region-Abelson(BCR-ABL)rearrangementsinadultswithacutelymphoblasticleukemiaand possibleassociationswithclinicalandlaboratorycharacteristicsandsurvival.
Methods:Forty-oneover18-year-oldpatientswithacutelymphoblasticleukemiaofboth gendersfollowed-upbetweenJanuary2008andMay2012wereincludedinthisstudy.Clinical andlaboratorydatawereobtainedfromthemedicalchartsofthepatients.Reverse transcrip-tionpolymerasechainreaction(RT-PCR)usingspecificprimerswasemployedtoidentify molecularrearrangements.
Results:Atdiagnosis,themedianagewas33years,andtherewasapredominanceofmales (61%).ThemostcommonimmunophenotypewasBlineage(76%).BCR-ABLrearrangements wasdetectedin14(34%)patientswiththefollowingdistribution:p190(28%),p210(50%)and doublepositive(22%).Overallsurvivalofpatientswithamean/medianof331/246daysof followupwas39%,respectively,negativeBCR-ABL(44%)andpositiveBCR-ABL(28%). Conclusion: TheseresultsconfirmthehighfrequencyofBCR-ABLrearrangementsandthe lowsurvivalrateofadultBrazilianpatientswithacutelymphoblasticleukemia.
©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
Introduction
Acute lymphoblastic leukemia (ALL) in adultscomprises a group ofdiseases withbiological, clinical,laboratorial and prognosticheterogeneitycharacterizedbyabnormal prolifera-tionandaccumulationofimmaturelymphoidcellsinthebone
∗ Correspondingauthorat:LaboratóriodeBiologiaMolecular,Fundac¸ãodeHematologiaeHemoterapiadePernambuco(HEMOPE),Rua
JoaquimNabuco,171,Grac¸as,52011-000Recife,PE,Brazil.
E-mailaddress:[email protected](I.deFranc¸aAzevedo).
marrowand lymphoidtissues.1 Unlike ALLinchildren,the
advancesinthetherapyinadultshavebeenslow,withamean survivalof35%inpatientsagedbetween18and60years.2As
aresult,considerableefforthasbeenmadetoidentify mark-ersthatcanbetranslatedtotheclinicasnewprognostictools andtherapeutictargets.3
http://dx.doi.org/10.1016/j.bjhh.2014.07.016
At present, the diagnosis and classification of acute leukemia depend on cytomorphologic, immunophenotypic, cytogeneticandmolecularanalyses.Moleculartestsarepart ofthecriteriafortheriskclassificationsystemoftheWorld HealthOrganization(WHO)andareusedtoevaluatethe prog-nosiscorrectlyanddefinetherapeuticstrategies.4
OfthevariousgeneticalterationsobservedinadultALL, thebreakpointclusterregion-Abelson(BCR-ABL)fusiongene isthemostcommonandisassociatedwithaparticularlypoor prognosis.1,5,6Thisgenerearrangementcanpresenttwo
dis-tinctisoforms,p190andp210duetodifferentbreakpoints.7
Recentstudiesindicatethatthesetwoisoformsmaybe associ-atedwithdifferentclinicalphenotypesinadultALLpatients.8
Theaimofthisstudy wastoinvestigatethe occurrence ofthep190 andp210BCR-ABLrearrangementsinadultALL patientsandtoinvestigatepossibleassociationswithclinical andlaboratoryfeaturesandsurvival.
Methods
The study group comprised 41 over 18-year-old patients of both genders diagnosed with ALL at the Fundac¸ão de HematologiaeHemoterapiadePernambuco(Hemope)from January2008toMay2012.Thediagnosiswasestablishedby clinical,cytomorphologicaland immunophenotypiccriteria. The standard treatment protocol used was the hyperfrac-tionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (HyperCVAD) regimen.9 This project was
approvedbytheResearchEthicsCommitteeoftheinstitution (#17/2010)andthestudywasconductedinaccordancewith theDeclarationofHelsinki2008.
Clinical and laboratory data were obtained from the patients’ records. Samples of peripheral blood and bone marrow were collected after informed consent had been given.Theidentificationofthep190andp210BCR-ABLgene rearrangementswasperformedbyreversetranscription poly-merasechainreaction(RT-PCR)accordingtotheinternational BIOMED-1protocol.10Thefollowingcontrolswereusedinthe
RT-PCRreactions:positive,negative,endogenousand contam-ination.
StatisticalanalysiswasperformedusingtheBioestat5.0 andStata9.1programs.Thet-testwasusedtocomparethe groupsregardingage,leukocytecount,blasts,plateletcount and hemoglobin. The Fisher exact test was used for the categoricalvariables(gender andimmunophenotype). Over-allsurvivalwascalculatedusingtheKaplan–MeierLogrank method.p-values <0.05 were considered statistically signifi-cant.
Results
Ofthe41patientsanalyzed,ALLwasmoreprevalentinyoung adultsandmenandthe mostcommonimmunophenotype wasBlineage(Table1).
Nostatisticallysignificantdifferenceswerefoundbetween thegroupsofBCR-ABLpositiveandnegativepatientsinrespect totheclinicalandlaboratoryvariables.However,thep210 BCR-ABLpatientshadhigherleukocytecountsandallp190BCR-ABL patientshadtheBimmunophenotype(Table2).
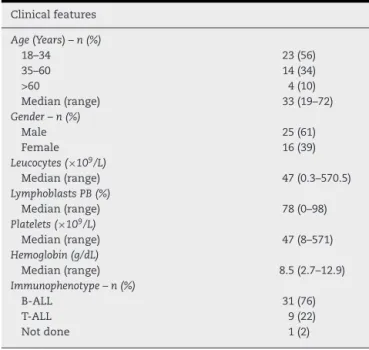
Table1–Clinicalfeaturesatdiagnosisof41adult patientswithacutelymphoblasticleukemiafrom2008 to2012atHEMOPE.
Clinicalfeatures
Age(Years)–n(%)
18–34 23(56)
35–60 14(34)
>60 4(10)
Median(range) 33(19–72)
Gender–n(%)
Male 25(61)
Female 16(39)
Leucocytes(×109/L)
Median(range) 47(0.3–570.5)
LymphoblastsPB(%)
Median(range) 78(0–98)
Platelets(×109/L)
Median(range) 47(8–571)
Hemoglobin(g/dL)
Median(range) 8.5(2.7–12.9)
Immunophenotype–n(%)
B-ALL 31(76)
T-ALL 9(22)
Notdone 1(2)
The overall survivalwas 39%with amean follow-up of 331days(median246days).SurvivalwaslowerforBCR-ABL positive(28%)thanforBCR-ABLnegative(44%)patients.The Log-ranktest,however,showednostatisticallysignificant dif-ference (p-value=0.2297)betweenthesurvivalcurvesofthe two groups (Fig. 1). The mortalityrate ofBCR-ABL positive patients is1.94timesgreater [95%ConfidenceInterval(CI): 0.80–4.26]thantheBCR-ABLnegativeindividuals,butagainthe differenceisnotstatisticallysignificant(p-value=0.148).
Discussion
Themedianageofthepatientswas33years,whichis sim-ilar toseveralpublished series.11–17 Males predominatedin
thesample,whichisinaccordancewiththemain multicen-terstudies.11–15,18–21Theresultsofseveralstudieshaveshown
similar numbersofleucocytes11,12,20 atdiagnosis,including
thepercentageofblastsintheperipheralblood13andplatelet
count.17 The76%frequencyofBcellphenotypeisin
accor-dancewithvariouspublishedstudies.11,12,17,21–23
The34%frequencyoftheBCR-ABLrearrangementissimilar tothatfoundinseveralstudieswithvaluesrangingfrom17%
to37%,1,11–14,17–22includinginelderlypatients,asreportedby
Larson.24NopublishedBrazilianstudieswithdataregarding
themolecularanalysisofBCR-ABLinadultALLpatientswere found for comparison. A case series of 42 adult Brazilian patientsshowed7%ofPh+samples.25
Theresultspresentedinthisstudyconfirmthehigh fre-quency of BCR-ABL rearrangements in adult ALL patients, but,differfromotherstudiesregardingthetypeofisoforms found.Gleieret al.21showed a37% positivityforthe
BCR-ABLfusiongenein478adultALLpatientsincludingthep190 (77%)andp210(20%)rearrangementsandbothisoforms(3%). Dombretetal.22foundthefollowingfrequenciesamong154
Table2–Summaryofclinicalandlaboratoryparametersof41adultpatientsdiagnosedwithacutelymphoblastic leukemiaatHEMOPE.
Variable BCR-ABL−
(n=27)
BCR-ABL+
(n=14)
BCR-ABL+
p190 (n=4)
BCR-ABL+
p210 (n=7)
BCR-ABL+
p190/p210 (n=3)
Age(years)
Median(range) 35(19–72) 38(20–72) 45(22–61) 35(20–72) 34(20–48)
Leucocytes(×109/L)
Median(range) 30.4(1–492) 77.1(0.3–570) 76.6(0.3–378) 96.0(6.7–570) 7.7(4.2–298.8)
Platelets(×109/L)
Median(range) 41(8–571) 69(18–213) 175.5(18–213) 60(27–155) 70(60–112)
Lymphoblasts(%)
Median(range) 78(0–97) 80(0–98) 75(0–93) 85(31–98) 36(3–94)
Immunophenotypea–n(%)
B-ALL 21(78.0) 10(71.5) 4(100.0) 3(43.0) 3(100.0)
T-ALL 5(22.0) 4(28.5) 0(0) 4(57.0) 0(0)
−:negative;+:positive.
a n=40.
1
0,8
0,6
Accumulated survival
Time (days) 0,4
BCR-ABL+ BCRABL -p = 0.2297
0,2
0
1 25 49 73 97
121 145 169 193 217 241 265 289 313 337 361 385 409 433 457 481 505 529 553 577 601 625 649 673 697 721 745 769 793 817 841 865 889 913 937 961 985 1009 1033
Figure1–Overallsurvivalcurvesof41adultpatientswithacutelymphoblasticleukemiaatFundac¸ãoHEMOPEaccordingto thepresenceofBCR-ABLrearrangements.
occurrenceofBCR-ABLpositivityinT-ALLcases19,butmaybe
duetosamplesizeorcharacteristicsofthepopulation stud-ied,aswellaspatientswithchronicmyeloidleukemiainacute phase.26
Theanalysis ofthe survival curves,in addition to con-firming the low rate of overall survival for adult patients diagnosed with ALL,9,14,20,21,23 also suggests an increased
adverse prognosis conferred by the presence of BCR-ABL rearrangements,2,18,21–23,27andthereforeaneedforother
ther-apeutic modalities, including targeted therapies and bone marrowtransplantation.28Therangeoftheconfidence
inter-valofthemortalityratesuggeststhatthesamplesizewastoo smalltoshowadifferenceandthatincreasingitwouldmakeit moreevident.Phenotypicdifferencesbetweenp190andp210 BCR-ABLpatientsiscontroversial.8,21 Furtherstudieswitha
largersamplesize,includingelderlypatients,areneededto bettercharacterizetheassociationbetweenthese rearrange-mentsanddifferentphenotypicexpressionsandsurvival.The detection of the BCR-ABL fusion gene is importantfor the classificationofriskgroupsofALL patientsandthecorrect targetingoftherapy.2,3Moreover,inadditiontotheBCR-ABL
fusion gene,other rearrangements, suchasE2A-PBX1, TEL-AML1,MLL-AF4,shouldbescreened,becausetheyalsohave prognosticsignificance.29
Conclusion
patients.Thestudyconfirmstheimportanceofdetecting BCR-ABLrearrangementsforthetreatmentandprognosisofthese patients.
Authors’
contributions
and
declaration
of
conflicts
of
interest
TheauthorsIlanadeFranc¸aAzevedoandRuiMiltonPatrício daSilvaJúniorcontributedequallytothedevelopmentofthe work.Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The authors thank the Fundac¸ão de Amparo à Ciência e TecnologiadoEstadodePernambuco(#APQ-1343-4.00-08)for fundingthestudyandProf.RicardodeAlencarXimenesArraes forhissupportwiththestatistics.
r
e
f
e
r
e
n
c
e
s
1. FoáR,ChiarettiS,GuariniA,VitaleA.Adultacute
lymphoblasticleukemia.RevBrasHematolHemoter.2009;31 (Suppl2):41–7.
2. BassanR,HoelzerD.Moderntherapyofacutelymphoblastic leukemia.JClinOncol.2011;29(5):532–43.
3. MullighanCG.Newstrategiesinacutelymphoblastic leukemia:translatingadvancesingenomicsintoclinical practice.ClinCancerRes.2011;17(3):396–400.
4. SwerdlowSH,CampoE,HarrisNL,JaffeES,PileriSA,SteinH, etal.WorldHealthOrganizationclassificationoftumorsof haematopoieticandlymphoidtissues.Lyon:IARCPress;2008.
5. JuricD,LacayoNJ,RamseyMC,RacevskisJ,WiernikPH,Rowe JM,etal.Differentialgeneexpressionpatternsandinteraction networksinBCR-ABL–positiveand–negativeadultacute lymphoblasticleukemias.JClinOncol.2007;25(11):1341–9.
6. SchaffelR,SimõesBP.Phyladelphiapositiveacute lymphoblasticleukemia.RevBrasHematolHemoter. 2008;30(1):52–8.
7. AdvaniAS,PendergastAM.BCR-ABLvariants:biologicaland clinicalaspects.LeukRes.2002;26(8):713–20.
8. JasoJ,ThomasDA,CunninghamK,JorgensenJL,Kantarjian HM,MedeirosLJ,etal.Prognosticsignificanceof
immunophenotypicandkaryotypicfeaturesofPhiladelphia positiveb-lymphoblasticleukemiaintheeraoftyrosine kinaseinhibitors.Cancer.2011;117(17):4009–17.
9. KantarjianH,ThomasD,O’BrienS,CortesJ,GilesF,JehaS, etal.Long-termfollow-upresultsofhyperfractionated cyclophosphamide,vincristine,doxorubicin,and
dexamethasone(Hyper-CVAD),adose-intensiveregimen,in adultacutelymphocyticleukemia.Cancer.
2004;101(12):2788–801.
10.VanDongenJJ,MacintyreEA,GabertJA,DelabesseE,RossiV, SaglioG,etal.StandardizedRT-PCRanalysisoffusiongene transcriptsfromchromosomeaberrationsinacuteleukemia fordetectionofminimalresidualdisease.Leukemia. 1999;13(12):1901–28.
11.GabertJ,BeillardE,vanderVeldenVH,BiW,GrimwadeD, PallisgaardN,etal.Standardizationandqualitycontrol studiesof‘real-time’quantitativereversetranscriptase polymerasechainreactionoffusiongenetranscriptsfor residualdiseasedetectioninleukemia–aEuropeAgainst CancerProgram.Leukemia.2003;17(12):2318–57.
12.TakeuchiJ,KyoT,NaitoK,SaoH,TakahashiM,MiyawakiS, etal.Inductiontherapybyfrequentadministrationof doxorubicinwithfourotherdrugs,followedbyintensive consolidationandmaintenancetherapyforadultacute lymphoblasticleukemia:theJALSG-ALL93study.Leukemia. 2002;16(7):1259–66.
13.HunaultM,HarousseauJL,DelainM,Truchan-GraczykM, CahnJY,WitzF,etal.Betteroutcomeofadultacute lymphoblasticleukemiaafterearlygenoidenticalallogeneic bonemarrowtransplantation(BMT)thanafterlatehigh-dose therapyandautologousBMT:aGOELAMStrial.Blood. 2004;104(10):3028–37.
14.ThomasX,BoironJM,HuguetF,DombretH,BradstockK,Vey N,etal.Outcomeoftreatmentinadultswithacute
lymphoblasticleukemia:analysisoftheLALA-94trial.JClin Oncol.2004;22:4075–86.
15.HuguetF,LeguayT,RaffouxE,ThomasX,BeldjordK, DelabesseE,etal.Pediatric-inspiredtherapyinadultswith Philadelphiachromosome-negativeacutelymphoblastic leukemia:theGRAALL-2003study.JClinOncol.
2009;27(6):911–8.
16.GokbugetN,ArnoldR,BohmeA,FietkauR,FreundM,Ganser A,etal.ImprovedoutcomeinhighriskandveryhighriskALL byriskadaptedSCTandinstandardriskALLbyintensive chemotherapyin713adultALLpatientstreatedaccordingto theprospectiveGMALLstudy07/2003.Blood.2007:
110.
17.BrüggemannM,RaffT,FlohrT,GökbugetN,NakaoM,Droese J,etal.Clinicalsignificanceofminimalresidualdisease quantificationinadultpatientswithstandard-riskacute lymphoblasticleukemia.Blood.2006;107(3):1116–23.
18.BassanR,SpinelliO,OldaniE,IntermesoliT,TosiM,PerutaB, etal.Improvedriskclassificationforrisk-specifictherapy basedonthemolecularstudyofminimalresidualdisease (MRD)inadultacutelymphoblasticleukemia(ALL).Blood. 2009;113(18):4153–62.
19.AnninoL,VegnaML,CameraA,SpecchiaG,VisaniG,Fioritoni G,etal.Treatmentofadultacutelymphoblasticleukemia (ALL):long-termfollow-upoftheGIMEMAALL0288 randomizedstudy.Blood.2002;99(3):863–71.
20.RibeiraJM,OriolA,BethencourtC,ParodyR,Hernández-Rivas JM,MorenoMJ,etal.Comparisonofintensivechemotherapy, allogeneicorautologousstemcelltransplantationas post-remissiontreatmentforadultpatientswithhigh-risk acutelymphoblasticleukemia:resultsofthePETHEMAALL 93trial.Haematologica.2005;90(10):1346–56.
21.GleinerB,GokbugetN,BartramCR,JanssenB,RiederH, JanssenJW,etal.Leadingprognosticrelevanceofthe BCR-ABLtranslocationinadultacuteB-lineagelymphoblastic leukemia:aprospectivestudyoftheGermanMulticenter TrialGroupandconfirmedpolymerasechainreaction analysis.Blood.2002;99(5):1536–43.
22.DombretH,GabertJ,BoironJM,HuguetFR,BlaiseD,Thomas X,etal.OutcomeoftreatmentinadultswithPhiladelphia chromosome-positiveacutelymphoblasticleukemia–results oftheprospectivemulticenterLALA-94trial.Blood.
2002;100(7):2357–66.
23.RoweJM,BuckG,BurnettAK,ChopraR,WiernikPH,Richards SM,etal.Inductiontherapyforadultswithacute
lymphoblasticleukemia:resultsofmorethan1500patients fromtheinternationalALLtrial:MRCUKALLXII/ECOGE2993. Blood.2005;106(12):3760–7.
24.LarsonRA.Managementofacutelymphoblasticleukemiain olderpatients.SeminHematol.2006;43(2):126–33.
26.RaananiP,TrakhtenbrotL,RechaviG,RosenthalE,AvigdorA, Brok-SimoniF,etal.Philadelphia-chromosome-positive T-lymphoblasticleukemia:acuteleukemiaorchronic myelogenousleukemiablasticcrisis.ActaHaematol. 2005;113(3):181–9.
27.RegoMF,PinheiroGS,MetzeK,Lorand-MetzeI.Acute leukemiasinPiauí:comparisonwithfeaturesobservedin otherregionsofBrazil.BrazJMedBiolRes.2003;36(3): 331–7.
28.AlvaradoY,ApostolidouE,SwordsR,GilesFJ.Emerging therapeuticoptionsforPhiladelphia-positiveacute lymphocyticleucemia.ExpertOpinEmergDrugs. 2007;12(1):165–79.