revbrashematolhemoter.2016;38(3):267–270
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
report
Renal
papillary
necrosis
in
a
patient
with
sickle
cell
disease
Benedito
Jorge
Pereira
a,b,∗,
Raquel
de
Andrade
baUniversidadedeSãoPaulo,FaculdadedeMedicina,HospitaldasClínicas,SãoPaulo,SP,Brazil bUniversidadeNovedeJulho(Uninove),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19March2016 Accepted10May2016 Availableonline4June2016
Introduction
Renalmanifestationsinsicklecelldisease(SCD)occurin one-thirdofadolescentsandyoungadults.1Thesemanifestations occurbecausethekidneyissensitivetohypoxia-induced vaso-occlusionresultingfromtheadhesionofsickledredbloodcells totheendothelium.2,3Therenalmedullaischaracterizedby acidosis,hypertension,andhypoxia.Thesefactorspromote thepolymerizationandsicklingofhemoglobin(Hb)S,which makesthisareaofthekidney susceptibletochangesinthe supplyofoxygen.3
Proteinuriaassociatedwithanemia increasestheriskof renalinsufficiencymainlyamongtheelderlywithSCD.4These chroniccomplicationsandtheimminentriskofasevereacute vaso-occlusiveeventshouldbeemphasizedtocliniciansand pediatricianswho treat SCD patients inemergency rooms, whichjustifiestheneedtoreviewtheclinicalfindingsofrenal involvementenablingdiagnosis,monitoring,andearly treat-ment.
ThisarticlereportsaclinicalcaseofapatientwithSCD withapossiblediagnosisofrenalpapillarynecrosisandrenal insufficiencythatrequireddialysis.
∗ Correspondingauthorat:HospitaldasClínicasdaFaculdadedeMedicinadaUniversidadedeSãoPaulo(HCFMUSP),SãoPaulo,SP,Brazil. E-mails:[email protected],[email protected](B.J.Pereira).
Case
report
Wereportonacaseofa30-year-oldmarriedmulattomale, whowasbornandraisedinSaoPauloandisself-employed.
Hepresentedtothe emergencyroomwithdyspnea and reddish-coloredurinethathadcontainedclotsforthreedays priortohisclinicvisit.Hehadacoughwithyellowsputum, andoccasionalepisodesofbilateralchestpain.Forfivedays, he had alsoexperienceddiffuse body pain, similarto pre-vious painfulcrises,but which evolvedtocontinuous right flankpainassociatedwiththreeepisodesofgrosshematuria. Hereportedtaking2mg/nightofclonazepam,dipyrone,and 5mg/dayoffolicacidathome.Nofever,headache,dysuria,or edemaofthelowerlimbswaspresent.
ThepatienthadpreviouslybeendiagnosedwithSCDand referredtotheHematologyClinicofthe Hospitaldas Clini-casoftheMedicalSchool,UniversidadedeSãoPaulo(FMUSP) for monitoring. The patient brought with him his records from the other service however, the patient had not been seenforthreeyears,andhismostrecentexams(12/29/2005) showedpreservedrenalfunction(urea:17mg/dLand creati-nine:0.65mg/dL). Thepatientreportedhavingundergonea
http://dx.doi.org/10.1016/j.bjhh.2016.05.004
268
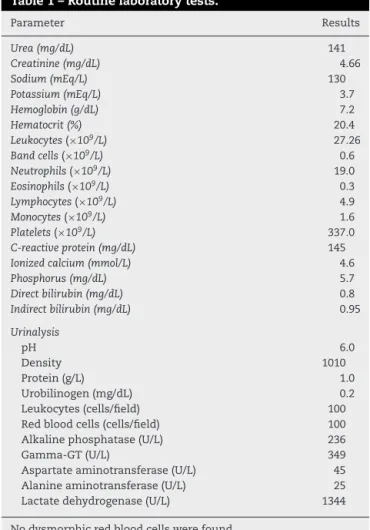
revbrashematolhemoter.2016;38(3):267–270Table1–Routinelaboratorytests.
Parameter Results
Urea(mg/dL) 141
Creatinine(mg/dL) 4.66
Sodium(mEq/L) 130
Potassium(mEq/L) 3.7
Hemoglobin(g/dL) 7.2
Hematocrit(%) 20.4
Leukocytes(×109/L) 27.26
Bandcells(×109/L) 0.6
Neutrophils(×109/L) 19.0
Eosinophils(×109/L) 0.3
Lymphocytes(×109/L) 4.9
Monocytes(×109/L) 1.6
Platelets(×109/L) 337.0
C-reactiveprotein(mg/dL) 145
Ionizedcalcium(mmol/L) 4.6
Phosphorus(mg/dL) 5.7
Directbilirubin(mg/dL) 0.8
Indirectbilirubin(mg/dL) 0.95
Urinalysis
pH 6.0
Density 1010
Protein(g/L) 1.0
Urobilinogen(mg/dL) 0.2
Leukocytes(cells/field) 100
Redbloodcells(cells/field) 100 Alkalinephosphatase(U/L) 236
Gamma-GT(U/L) 349
Aspartateaminotransferase(U/L) 45 Alanineaminotransferase(U/L) 25 Lactatedehydrogenase(U/L) 1344
Nodysmorphicredbloodcellswerefound.
splenectomyfiveyearsprevioustoadmission;this informa-tion could notbeconfirmed because it isassumedthat at anadultage,theoccurrenceofsignificanthyposplenismmay haveoccurred.
Thepatient smoked, consumed alcohol (2–3 beers/day), andwasadailydruguser(marijuanaplusinhaledand intra-venouscocaine),butreportedbeingabstinentforthreedays.
Inthe physical examinationthe patientpresented with generaloveralldiscolorationoftheskin(2+/4+)andicterus (2+/4+);hewasalsoacyanoticandeupneic.Hewasafebrile withablood pressureof200/110mmHgandaheartrateof 96beatsperminute.Onlungauscultation,vesicularbreath soundswerefoundthroughoutthechest,aswerecrepitant rales in the left pulmonary base; the respiratory rate was 18breathsperminute.Uponauscultationofthe cardiocircu-latorysystem,normophoneticrhythmicsounds werefound withtwonormalsoundsanda1+/6+systolicpanfocal mur-mur.Theabdomenwasflatwithasplenectomyscar,andpain wasinduceduponrightflankpalpation;theabdomenwasalso flaccid,negativeonabdominaldecompressiontest,and neg-ativeforGiordano’ssign.Anexaminationofthelowerlimbs showedgoodperipheralperfusionandnoedemaorsignsof deepvenousthrombosis.
Uponarrival attheemergency room(6/18/2010),achest X-rayandroutinelaboratorytestswereperformed(Table1).
Hypertensive emergency and uremic syndrome were identified in association with severe low back pain and
a possible concomitant infection. The indication of treat-ment includedemergency treatmentforhypertensionwith sodium nitroprusside, antibiotics (ceftriaxone 1g IV b.i.d. andclarithromycin250mgIVb.i.d.)forpossibleurinaryand tracheal-bronchialinfections,andemergencyhemodialysis.
ADopplerultrasound (US)oftherenal arteriesrevealed rightrenalhydronephrosiswiththerightkidneymeasuring 12cm, ahyperechoic right kidney without obstruction and no thrombi in the renal arteries and veins. Moreover, US showedahyperechoicleftkidneymeasuring10cm,without hydronephrosis.Anabdomenandpelviccomputed tomogra-phy(CT)revealedmild/moderaterightpyelocalycealdilatation andproximalureteralectasiawithhyperattenuatingmaterial inthemiddlethird(clot).Hydronephrosiswasnotidentified intheleftkidney.Apresumptivediagnosiswasmadeofrenal infarctionandrenal papillarynecrosiscomplicatedbySCD. Afterthepatient’sbloodpressurewasstabilizedand antibi-otictreatmentwascompleted,hecontinuedtoreceivechronic dialysisasanoutpatient.
Discussion
Fortunately,renal changes thatoccur inpatientswith SCD arelesssevere,usuallyhaveasloweronset,andareless pro-gressivethantherenalchangesthatthispatientexperienced. Threeyearspreviously,thepatienthadpreservedrenal func-tion, andtherefore, it issuggestedthatanacute condition occurredatthetimeofadmission,rememberingthatthetime fromlossofrenalfunctiontodialysislevelsisveryshortin chronicinfarctions.Inaddition,thekidneyimagingat admis-sionindicatednocontractedkidney(secondarytofibrosis),as occursinchronicinfarctions.Inthiscase,theclinicalpicture wasoneofasuddenonsetofrenalpapillarynecrosis,which ledtosevererenalfailurethatrequireddialysis.
The presence of a normal contralateral kidney associ-atedwithanobstructedkidneyafterpapillarynecrosisisan uncommonfindingincasesofsevererenalinsufficiencythat requires dialysis.Possiblepapillarynecrosisofthe left kid-ney wasnot evidentonimaging.In addition, thepresence ofacontractedkidney,asoccursinchronicrenalinfarctions, wasnotobserved.Notably,theserenalchangesaretheresult ofthesicklingofredblood cellsandvaso-occlusiveevents. Theadherenceoferythrocytestothevascularendotheliumis likelytheprimarymechanismbywhichmolecularalterations thatoccurinredbloodcellsaffecttissues.5,6
The urinary and pulmonary tract infections also con-tributed tothe patient’s admission tohospital. Amongthe conditions that are commonly seen in these patients are cardiopulmonarycomplications(especiallycongestiveheart failure and acute chest syndrome),renal insufficiency, and strokes;infectionsmayprecedeorbeconcomitantwiththese complications,aswasobservedinthispatient.5,6
revbrashematolhemoter.2016;38(3):267–270
269
andhypoxia,andthesefactorscontributetothesicklecell cri-sisthatisresponsiblefortheocclusionoftherenalvessels.3 Themostimportantconsequenceofthesecrisesisdamage tothe renaltubules; this causes atrophyordilation ofthe tubules,thepresenceofproteincylinders,andirondeposition alongwithdegenerationofthetubuleepithelium.1,7
Regardingthepatient’scomplaintofhematuria,wenote thatthisisacommonclinicalmanifestation.Bleedingoccurs duetothepolymerizationofredbloodcellswithintherenal medulla.In 80% ofcases, bleeding occurs in just one kid-ney. Treatment forhematuriais conservative and includes bedrest,maintenanceofahighurineflowrate,urine alkalin-ization,and(ifnecessary)bloodtransfusions.1Mostepisodes are limited but can occur due to micro infarctions in the renalpyramids,whichmaybeassociatedwithrenalpapillary necrosis.3,7
Upon admission to the emergency room, the following clinicalpicturewasobserved:ahypertensiveemergency asso-ciatedwithrenalfailure,whichpreviouslydidnotexist.Renal insufficiencyduetonephropathyisobservedin4–21%ofadult SCDpatients.Renalinsufficiencyisoneofthemostserious complicationsofthisdiseaseandcontributestotheearly mor-talityofpatients.Diseaseduration,severityofanemia,and geneticfeaturesareriskfactorsthatinfluencethe develop-mentofrenalinsufficiency.8
This patient experienced a long interval during which his disease was not regularly monitored, and because it is viewed as a chronic disease, the patient’s serious drug addiction problems were detrimental to the clinical and laboratoryparametersofrenalimpairmentpriorto hospital-ization.Severalmarkershavebeenstudiedasearlyindicators of renal impairment, including the estimated glomerular filtration rate (eGFR), microalbuminuria, and proteinuria. Microalbuminuria,anearlymarkerofkidneydamage,maybe directlyrelatedtoage,andisinverselyrelatedtohemoglobin levels.8
Nephrotic syndromewould indicate a chronicevolution offocal segmentalglomerulosclerosis. However,no clinical reportrevealednephroticsyndromepriortotheadmissionof thispatienttothehospital.Inaddition,clinicalsymptomsof acutevaso-occlusiveevents,suchasthosethatoccurin papil-larynecrosis,wereobserved.Therefore,imagingexamswere importanttoconfirmthisfinding.
Renalpapillarynecrosisischaracterizedbypyelocalyceal andureteralocclusions,whichareduetoclotsandnecrotic papillae, and may have various causes including diabetes, analgesics,andSCD.Themaincauseofpapillarynecrosisin SCDisrelatedtotheenvironmentoftherenalmedulla,which ishypertonic,hypoxic,and favorsthe sicklingofredblood cells.5 Iftheischemic processisduetoatemporaryspasm andnormalcirculationisrestored,thetissuesthatareaffected wouldbeabletorecover.However,iftheischemiacontinues and perfusion is not restored, these factors lead to coag-ulativenecrosisand tubular fibrosis,which are irreversible processes.9
ACTscanshowsischemicchangeswithgreateraccuracy thanUS. InhelicalCT,changes thatleadtorenal papillary necrosis may be observed at the beginning of the corti-comedullaryphase,butthesecanbebetterdescribedusing urography. In urography, changes are presented as poorly
margined areasofenhancement,which arereduced atthe pointofthemedullarypyramid.10
In this case, no regular outpatient follow-up was con-ducted,whichhamperedthepossibilityofearlyintervention withrespecttotherenalmanifestationsoranyattemptsto preventthevasculareventinquestion.Measurestoprevent such renal lesions include angiotensin converting enzyme inhibitorsandhydroxyurea,whicharebelievedtoprovidethe greatestbenefitsinthecontrolofsicklecellnephropathy.The earlyidentificationofriskfactorsforrenalinvolvementmay allowthephysiciantoprovideappropriatetreatmenttothe patient.5,7,8
Studiesindicatethatlactatedehydrogenase(LDH)maybe used as anearly marker foridentifying the risk ofkidney failureinSCDpatients.TheserumLDHlevelsareusedasa measureofintravascularhemolysis,whichisamajor patho-logicalmechanismofcardiovascularcomplicationsaswellas pulmonary,gastrointestinal,andrenalmanifestationsofSCD patients.8,10 Exacerbatedhemolysisisassociatedwithearly mortalityinpatientswiththisdisease.8
Regardingtheclinicalevolutionofhisdisease,thispatient receivedhypertensiveemergencytreatment,including intra-venoussodiumnitroprussideanddialysisforbloodvolume andmetaboliccontrol.Hewasthendischargedandcontinued toreceiveoutpatientdialysis.Theevolutionofthisdiseasewill undoubtedlyincreasethemorbidityofSCDpatientsanditis correlatedwithanincreasedmortalityrate.
Conclusions
Itisextremelyimportanttorecognizesicklingmechanisms and howtheyaffect renaldisorders.Itisalsonecessaryto understandthatrenalchangesoccur overtheyearsinSCD patients,andwhenaccompaniedbyclinicalsymptomssuch ashematuria,microalbuminuria,andproteinuria, itsignals thenecessityofimprovedpatientcare.Promptcarewill pre-vent more serious and permanent injuries such as renal papillary necrosisand consequent renal insufficiency that requiresdialysisandcanfurtherimpairthequalityoflifeand increasethemortalityofSCDpatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BriehlRW.Nucleation,fibergrowthandmelting,anddomain
formationandstructureinsicklecellhemoglobingels.JMol
Biol.1995;245(5):710–23.
2.ZagoMA.Anemiafalciformeedoenc¸asfalciformes.Manual
deDoenc¸asmaisImportantes,porRazõesÉtnicas,na
Populac¸ãoBrasileiraAfro-Descendente.SérieA.Normase
ManuaisTécnicosno.123.Brasília:MinistériodaSaúde;2001.
3.MagalhaesIQ.Alterac¸õesrenaisnasdoenc¸asfalciformes.Rev
BrasHematolHemoter.2007;29(3):279–84.
4.AtagaKI,DerebailVK,ArcherDR.Theglomerulopathyof
270
revbrashematolhemoter.2016;38(3):267–2705. HaymannJP,StankovicK,LevyP,AvellinoV,TharauxPL,
LetavernierE,etal.Glomerularhyperfiltrationinadultsickle
cellanemia:afrequenthemolysisassociatedfeature.ClinJ
AmSocNephrol.2010;5(5):756–61.
6. TelenMJ.Redbloodcellsurfaceadhesionmolecules:their
possiblerolesinnormalhumanphysiologyanddisease.
SeminHematol.2000;37(2):130–42.
7. AlhwieshA.Anupdateonsicklecellnephropathy.SaudiJ
KidneyDisTranspl.2014;25(2):249–65.
8. GurkanS,ScarponiKJ,HotchkissH,SavageB,DrachtmanR.
Lactatedehydrogenaseasapredictorofkidneyinvolvement
inpatientswithsicklecellanemia.PediatrNephrol.
2010;25(10):2123–7.
9.JungDC,KimSH,JungSI,HwangSI,KimSH.Renalpapillary
necrosis:reviewandcomparisonoffindingsatmulti-detector
rowCTandintravenousurography.Radiographics.
2006;26(6):1827–36.
10.RajVM,FreundlichM,HamidehD,AlvarezO,Seeherunvong
W,AbitbolC,etal.Abnormalitiesinrenaltubularphosphate
handlinginchildrenwithsicklecellanemia.PediatrBlood