w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Review
article
Myeloproliferative
neoplasms
and
the
JAK/STAT
signaling
pathway:
an
overview
Renata
Mendes
de
Freitas
∗,
Carlos
Magno
da
Costa
Maranduba
UniversidadeFederaldeJuizdeFora(UFJF),JuizdeFora,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30June2014 Accepted19October2014 Availableonline9June2015
Keywords:
Hematologicneoplasms Januskinase2
STATtranscriptionfactors JAK2V617Fmutation
a
b
s
t
r
a
c
t
Myeloproliferativeneoplasmsarecausedbyaclonalproliferationofahematopoietic progen-itor.Firstdescribedin1951as‘MyeloproliferativeDiseases’andreevaluatedbytheWorld HealthOrganizationclassificationsystem in2011,myeloproliferativeneoplasmsinclude polycythemiavera,essentialthrombocythemiaandprimarymyelofibrosisinasubgroup calledbreakpointclusterregion-Abelsonfusiononcogene-negativeneoplasms.According toWorldHealthOrganizationregardingdiagnosiscriteriaformyeloproliferativeneoplasms, thepresenceoftheJAK2V617Fmutationisconsideredthemostimportantcriterionin thediagnosisofbreakpointclusterregion-Abelsonfusiononcogene-negativeneoplasms andisthususedasaclonalmarker.TheV617FmutationintheJanuskinase2(JAK2)gene producesanalteredproteinthatconstitutivelyactivatestheJanuskinase/signal transduc-ersandactivatorsoftranscriptionpathwayandotherpathwaysdownstreamasaresultof signaltransducersandactivatorsoftranscriptionwhicharesubsequentlyphosphorylated. Thisaffectstheexpressionofgenesinvolvedintheregulationofapoptosisandregulatory proteinsandmodifiestheproliferationrateofhematopoieticstemcells.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
Introduction
Myeloproliferativeneoplasms(MPNs)areclonaldisordersof hematopoietic stem cells, in which there is an increased proliferation ofthe myeloid lineage with effective matura-tionresultinginperipheralbloodleukocytosis,andincreased redbloodcellmass;theseneoplasmscanprogressto fibro-sis or leukemic transformation. The MPNs are a group of diseases that include polycythemia vera (PV), essential thrombocythemia (ET) and primary myelofibrosis (PMF),
∗ Correspondingauthorat:RuaAristótelesBraga,125,SãoPedro,JuizDeFora,MG,Brazil.
E-mailaddress:[email protected](R.M.deFreitas).
which are collectively known asbreakpointcluster region-Abelson fusion oncogene (BCR-ABL)-negative neoplasms. These threediseases share commonclinical features,such asproliferationofhematopoieticstemcellsindependentof growthfactors,bonemarrowhypercellularity,increasedrisk ofthromboticeventsandhemorrhages.1–4
Studiescarriedoutin2005identifiedabnormalitiesinthe functioning of the Janus kinase 2 (JAK2) protein which is expressedbytheJAK2gene.Here,asensemutationatexon 14 ofthe JAK2gene (g.1849 G>T)5,6 resultsin the
substitu-tion ofavalineforaphenylalanine atposition617located
http://dx.doi.org/10.1016/j.bjhh.2014.10.001
inthepseudokinaseJH2domain.Itisresponsiblefor consti-tutivelyactivatingtheJAK/signaltransducersandactivators oftranscription(STAT)signalingpathwayandotherpathways downstream.TheJAK2V617Fmutationoccursatafrequency of95%inPVandof55–60%inETandPMF.5–10
Myeloproliferative
neoplasms
Dameshek1 carried out the first classification of
Myelo-proliferative Diseases in 1951. However, the World Health Organization(WHO)classificationsystempublishedin2011 introducedanewclassificationoftumorsofhematopoietic and lymphoid tissue and changed the term to ‘myelopro-liferative neoplasms’. The MPNs include chronic myeloid leukemia(CML),PV, PMF,ET,chronic neutrophilicleukemia (CNL), chronic eosinophilic leukemia (CEL), mast cell dis-ease (MCD) and unclassified myeloproliferative neoplasms (MPN-u).11–13 CML is characterized by the presence of the
Philadelphiachromosome(Ph)resultingfromatranslocation betweenchromosomes9and22.Theresultinghybridgene, BCR-ABL,encodesa proteinof210kDa, displayingtyrosine kinaseactivityandaffectsgrowthandcelldifferentiation.14
In addition to their common features, PV is character-izedprimarilybyanincreaseinredbloodcellproduction,ET forexcessiveproductionofplatelets,andPMFfor morpho-logicalchangesinmegakaryocytesand thedevelopmentof monocytes thatlead tothe secretion ofangiogenicfactors responsibleforpromotingfibrosisinthebonemarrow.15
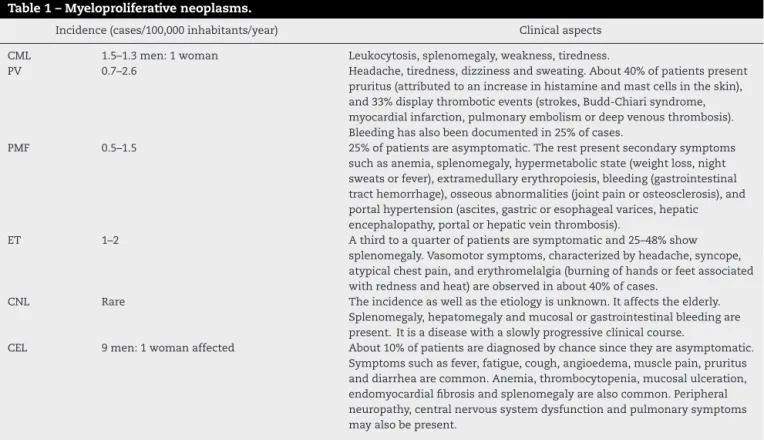
Table1presentstheMPNtypes,theincidencesandclinical aspectsofeach.
InadditiontotheJAK2gene,workscarriedoutsince2005 havefoundothermutationsincandidategenes,includingthe
myeloproliferativeleukemia(MPL),ten-eleventranslocation2(TET2) amemberoftheTEToncogenefamily,additionalsexcomb-like 1(ASXL1),CasitasB-lineagelymphoma(CBL),isocitrate dehydro-genase(IDH)andIKAROSfamilyzincfinger1(IKZF1)genes,all identifiedwithinthegroupofBCR-ABL-negativeneoplasms. MutationsintheJAK2andMPLencodergenesseemtohave greatereffectandaremoreassociatedwithPV,ETandPMF withfrequenciesaround95%,55%and60%forJAK2and0%, 0.3%and10%forMPL.16
ThefunctionalconsequencesofthesemutationsinMPNs include disruptionofthe JAK/STAT signaling pathway, epi-genetic modulation of transcription as well as abnormal accumulationofoncoproteins.However,itisstillunclearhow alltheseabnormalitiescontributetowarddiseaseonsetand clonalevolutionofcells.16
Pathogenesis
of
myeloproliferative
neoplasms
In the literature, some evidence suggests that phenotypic characteristics observed inMPNs are caused due to disor-dersinthehematopoieticcellsignalingprocess.Ithasbeen reportedthathematopoieticprogenitorsarehypersensitiveto severalgrowthfactorsinPV,ETandPMF,17 andthat
abnor-malmyeloproliferationinpatientswithMPNsoriginatesfrom constitutiveactivationofsignaltransductionpathways.These arecausedbygeneticrearrangementsormutationsthataffect tyrosinekinasesorassociatedmolecules.18Basedonthisand
otherevidence,someresearchgroupsstartedtoworkwiththe hypothesisthatalterationsinthefunctionoftheJAK2protein couldberelatedtoMPNs,sincethisproteinismainly respon-siblefortheactivationofmoleculesinvolvedincellsignaling processesandredbloodcellproduction.19
Table1–Myeloproliferativeneoplasms.
Incidence(cases/100,000inhabitants/year) Clinicalaspects
CML 1.5–1.3men:1woman Leukocytosis,splenomegaly,weakness,tiredness.
PV 0.7–2.6 Headache,tiredness,dizzinessandsweating.About40%ofpatientspresent
pruritus(attributedtoanincreaseinhistamineandmastcellsintheskin), and33%displaythromboticevents(strokes,Budd-Chiarisyndrome, myocardialinfarction,pulmonaryembolismordeepvenousthrombosis). Bleedinghasalsobeendocumentedin25%ofcases.
PMF 0.5–1.5 25%ofpatientsareasymptomatic.Therestpresentsecondarysymptoms
suchasanemia,splenomegaly,hypermetabolicstate(weightloss,night sweatsorfever),extramedullaryerythropoiesis,bleeding(gastrointestinal tracthemorrhage),osseousabnormalities(jointpainorosteosclerosis),and portalhypertension(ascites,gastricoresophagealvarices,hepatic encephalopathy,portalorhepaticveinthrombosis).
ET 1–2 Athirdtoaquarterofpatientsaresymptomaticand25–48%show
splenomegaly.Vasomotorsymptoms,characterizedbyheadache,syncope, atypicalchestpain,anderythromelalgia(burningofhandsorfeetassociated withrednessandheat)areobservedinabout40%ofcases.
CNL Rare Theincidenceaswellastheetiologyisunknown.Itaffectstheelderly. Splenomegaly,hepatomegalyandmucosalorgastrointestinalbleedingare present.Itisadiseasewithaslowlyprogressiveclinicalcourse.
CEL 9men:1womanaffected About10%ofpatientsarediagnosedbychancesincetheyareasymptomatic. Symptomssuchasfever,fatigue,cough,angioedema,musclepain,pruritus anddiarrheaarecommon.Anemia,thrombocytopenia,mucosalulceration, endomyocardialfibrosisandsplenomegalyarealsocommon.Peripheral neuropathy,centralnervoussystemdysfunctionandpulmonarysymptoms mayalsobepresent.
TheJanuskinase2gene
The JAK2 gene, located on chromosome 9p24 in humans, includes25 exonsencodingaproteinofabout 1132amino acids.ThisproteinisnamedJAK2anditisamemberofthe Januskinase(JAK)family.Fourmembersofthisfamilyhave alreadybeenidentified:JAK1,JAK2,JAK3andTyk2.20
In2005,thediscoveryoftheJAK2mutation(JAK2V617F) expandedtheknowledgeaboutthepathogenesisof BCR-ABL-negativeneoplasms.Amissensemutationatpositiong.1849 withaguanine-thyminetransversion(g.1849G>T)5,6was
iden-tifiedinexon14oftheJAK2gene.Thismutationresultsinthe substitutionofvalineforphenylalanineataminoacidposition p.617,5affectingthepseudokinasedomain(JH2)oftheprotein.
TheJAK2V617FmutationispresentinmostpatientswithPV andinasubgroupofpatientswithETandPMF(∼95%inPV,
50–60%inETand50–60%inPMF).5–9,19
It has been shown that the JAK2 V617F mutation causes genetic instability in gene expression by induc-ing changes in the chromatin structure and by reducing the apoptotic response to DNA damage. These are mech-anisms that can increase the accumulation of genetic lesionsleadingtomalignanttransformations.12Besidesthe
g.1849 G>T (p.V617F) mutation,5,6 other mutations were
found in exon 12 in 2007 namely: p.N542-543del, p.E543-D544del,p.K539L,p.F537-K539delinsL,p.H538-p.K539delinsL, p.H538QK539L, p.V536-1546dup11, p.F537-1546dup10+F547L, p.R541E543delinsK-and-p.I540E543delinsMK.21–23Thesewere
foundtoshowlowfrequenciesofabout3–4%inPVpatients. Therearevalidtechniquesthatdetectthesemutationsand theiractivesearchisjustifiednotonlyduetotheabsenceof theexon14mutation,butalsoinpatientsthathave erythro-cytosisandinthosewithlowlevelsoferythropoietin.24
TheJanuskinase2protein
MembersoftheJAK2proteinfamilyhavesevenhomologous domains(JH)thatarenumberedfrom1to7.TheJH1domain acts as a kinase domain, which contains the adenosine triphosphate(ATP)-bindingandsignalingpathwayactivation regions.TheJH2domainisapseudokinasethatishomologous totheJH1domain.Itlackscatalyticactivityduetoa substitu-tionofanaspartateresidueinthecatalyticloop(His–Arg–Asp– HRDmotif).JH2hasaninhibitoryfunctionthatregulatesboth thebasalactivityofJAKandthecytokine-inducedactivation byinteractingwiththeactivesite,JH1,blockingATPand/or substratesbindingtothecatalyticsite.25–27
Mutationsin exon 12 ofJAK2 are found in the binding regionoftheSrchomology2(SH2)andJH2domains.Although notdirectlylocatedintheJH2domain,thesemutationsmay modifythestructureofthepseudokinasedomain,inducing erythropoietinhypersensitivitysimilartothatcausedbythe JAK2p.V617Fmutation.5,9,28,29
TheJanuskinase2/signaltransducersandactivatorsof transcriptionsignalingpathway
Signalingreceptors
Cytokines from the hematopoietic system include inter-leukins (ILs), colony stimulating factors (CSFs), interferon
(INF), erythropoietin (EPO) and thrombopoietin (TPO) all of which activate the signal transduction of the JAK/STAT signalingpathway.30,31 Mostofthesereceptorsarepartofa
typeI-homodimerreceptorfamily,thatincludesthe erythro-poietin(EPO-R)andthrombopoietin(TPO-R)receptors.32
Thetype Ireceptoris specificallyexpressedduring ery-throid and myeloid differentiation and its expression may account for the preferential activity of JAK2 V617F over myeloid lineage cells rather than lymphoid lineage cells, whichlackthistypeofreceptor.32
Janus
kinases
JAKsareassociatedwiththeintracellulardomainsofcytokine receptors; they show intrinsic kinase activity mediated through their band-4.1 protein, ezrin, radixin, and moesin (FERM)andSH2domainsandarekeptinaninactivestatein theabsenceofspecificreceptor-activatingligands.33,34
Cytokine binding leads to a conformational change of thereceptor,cytoplasmicallyaffectingassociatedJAKs, caus-ingactivationandphosphorylation.Phosphorylatedtyrosine residues in JAKs actas binding sitesfor the SH2 domains in signaling molecules. Mutations in JAK2 generate con-stitutive activation of the JAK/STAT pathway, mainly in STAT3 and STAT5. In addition to ‘hot spot’ mutations, constitutive activation of tyrosine kinases also occurs by chromosomal translocation, deletion and tandem duplica-tion,whicharecommonpathogeniceventsinhematopoietic malignancies.10,27,31–35
TheSTATsarelocatedinthecytosoland migratetothe nucleus,regulatinggenetranscriptiononlyuponactivation. OnceassociatedwiththephosphorylatedsitesofJAK,these STATsalsophosphorylateanddimerize.26
DimerizedSTATsmigratetowardthenucleus,wherethey act as transcription factors, activating or repressing genes thatareimportantincellproliferationandsurvival.Someof thesegenesincludethosethatexpresscyclinsaswellas anti-apoptotic proteins.36 STAT dimers also activate genes that
encodeinhibitoryproteinsthatcontributetowardthe termi-nation ofcellularresponse.Someoftheseproteinsbindto phosphorylated JAKsand inactivate them,as well as their associated receptors. Others bind to phosphorylated STAT dimersandstopthemfrombindingtotheirtargetgene.37
JAK/STAT-mediatedsignalingcontrolmechanismsinclude dephosphorylationofJAKandSTAT.Thisiscausedbyan inhi-bition triggeredbysuppressorsofcytokinesignaling(SOCS) proteins,thelymphocyteadaptorprotein(LNKalsoknownas SH2B3)andCBL.30,32
NegativeregulationoftheJanuskinase2/signal transducersandactivatorsoftranscriptionpathway
threePIAS:SOCS,CBLandLymeneuroborreliosis(LNB) pro-teins.
SOCSproteinsareafamilyofcytokinesignaling suppres-sorsoftheJAK/STATpathway,characterizedbythepresenceof anamino-terminaldomainthatisvariableinsize.Itincludes aninhibitorydomain,aSH2domainandacarboxy-terminal domain called SOCS box. Currently, there are eight mem-bersin this family, namely: SOCS1, SOCS2, SOCS3, SOCS4, SOCS5,SOCS6,SOCS7andCIS.Undernormalconditions,they areexpressedatlowlevelsinunstimulatedcellswhiletheir expressionincreaseswhenSTATsareactivated.30,31,38
SOCS can inhibit the JAK/STAT signaling through two mechanisms: (1)inhibitionofJAK2 kinase activity by com-petingwiththeSTATsSH2domainsforbindingsitesinthe cytoplasmicdomainofthereceptoror(2)proteasomal degra-dationofsignalingproteinsbybindingtotheJH1domainof JAK2,inhibitingtheactivationofallotherJAK/STAT-associated pathways.39
SomemutationsindifferentSOCShavebeenidentifiedin MPNs,butarerarelyfound.HypermethylationofCpGislands in SOCS1 and SOCS3 is associated with a decrease in the expressionoftheseregulatorsinp.V617F-positivePVandET patients.5,10
Other important components of this negative regula-torycomplexincludemultifunctionalproteinswithubiquitin ligaseactivity, suchas CBL.CBL is usuallyinvolved inthe negativefeedbackoftyrosine kinase receptorsby competi-tiveblockingsignaling.Itinducesproteasomaldegradationof tyrosinekinasesactivatedbyubiquitination.AllCBLhave sin-gledomainproteinsthatrecognizesphosphorylatedtyrosine residuesthatarepresentonactivatedtyrosinekinases.10,40
LNK,includedintheSH2Bproteinfamily,negatively reg-ulatestheactivityofJAK2bybindingtoSH2-phosphorylated tyrosine.ItalsoregulatesthesignalingofTPO-RandEPO-R, anditisdetectedinbothJAK2V617F-positiveand-negative patients.10IncreasedLNKdeficiencyincreasestheoncogenic
ability of JAK2 to expand myeloid progenitors in vitro and
invivo.41
MutationintheJanuskinase2geneandchangesin proteinfunction
InadditiontoactivatingtheJAK/STATpathway,thep.V617F mutation5 also constitutively activates the rat sarcoma
(RAS)/Mitogen-activated proteinkinases (MAPK) and phos-phoinositide3-kinase(PI3K)/proteinkinaseB(PKB,akaAkt) pathways,whichresultsinanincreasedexpressionofmitotic proteins,regulatoryproteinsfromthecellularcycle[cyclins D1, CDC25A (cell division cycle)] and anti-apoptotic genes [B-celllymphoma-extra-large(Bcl-XL)andBcl2].These abnor-malitiesinvolvingtheJAK/STATandrelatedpathwaysresult inproliferationofaffectedcells(Figure1).10
In mutated cells, down-regulation becomes inadequate and/or inefficient. SH2 domains, normally present in PIAS proteins,cannotdephosphorylateJAK2.Inaddition,the anti-apoptotic mechanismsareexpressedatmuchhigherlevels thannormal.Anacquiredmutationinoneoftheseregulatory proteinscantriggeranexacerbatedactivationofSTAT,evenin theabsenceofspecificmutationsinJAK2.42
Additional molecular events appear to interfere with the activity of JAK2, such as cytogenetics, which increase
EPO-R
Linker
Extracellular
Intracellular
JAK2 JAK2
P13K
Akt
CORE
DNA
STAT
socs JAK2
JAK2 JAK2
JAK2
P P PP P P
P
P P
P P
P P
P P
P
STAT3,
STAT5
Negative feedback
SOCS, Bcl-xl, p21, MYC etc
Promoter
Figure1–Signalingpathwaysactivatedbycytokinereceptorbinding.PI3K,AktandSTATareactivatedafterthe
the kinase activity of the protein, the regulatory ability ofphosphorylasesandSOCS proteins,polymorphisms,and mutationsincytokinereceptors.43
Questionsaboutthedifferentphenotypesin
BCR-ABL-negativemyeloproliferativeneoplasmsandthe V617Fmutation
AfurtherintriguingquestionforresearchersregardingMPNs ishowthesame mutationcantriggerthreephenotypically differentdiseases.Thereisstillnoclearunderstandingofthe molecularmechanismsinvolvedintheprocess,just hypothe-ses.Oneofthemisthedose–responsegenehypothesis,which isassociatedwithallele load.Anotheristhattheremaybe epigeneticchangesthatpredisposethepatient’sorganismto developcertain MPNs aswell as changes ingenes specific inthedevelopmentofmalignancies,aswellasmutationsin othersignalingpathwaysthatmightaffectsignalingin regu-latoryproteins.16
For Kralovics et al., Plo et al., Smith & Fan, Cross and Pagliarini,26,44–47thephenotypeofthediseaseisrelatedtothe
conceptofallelicload.Thus,lowlevelsofmutantalleleswould resultinETphenotype,whilehigherlevelsofmutatedalleles wouldleadtoaphenotypesimilartoPV.Thesehigherlevelsof mutatedallelesinhematopoieticstemcellscouldbe associ-atedwiththepatient’shomozygouscondition,causedbyloss ofheterozygosity,asexplainedbythetheoryofuniparental disomy.48
Presumably,homozygosity confersaproliferative advan-tageoverothercells,whichpresentonlyonemutatedallele, increasingtheactivitylevelofthetyrosinekinasegenerated bythe mutatedJAK2.PatientswithETandPMFaremostly heterozygousandseldomshowhomozygosity.48
Besidestheassociationbetweenphenotypeand homozy-gosity/heterozygosity,thereare otherhypothesesthat have attempted to correlate the different phenotypes observed relatedtotheJAK2V617Fmutation.
Intheirstudy,Ploetal.45discussthegene-dose
hypothe-sis,whichpostulatesthattheJAK2mutationcanbeastarting pointforthethreepathologies.Theyalsodiscussthe exist-enceofothergeneticeventsthatcanmodifytheJAK2kinase activity,whichmayexplaintheheterogeneitypresentin clas-sicMPNs.Severalmechanismshavebeenproposedtoaidthe understandingoflossofheterozygosityand/orthepresence ofnewgeneticabnormalities,includingthedouble-stranded breakrepairmechanismsinDNA,homologousrecombination andnon-homologousendjoining.Alltheseleadtogenomic instability,whichhighlightshowessentialtheprecise regula-tionofthesemechanismsisforthemaintenanceofgenome stabilityanddiversity.49–51
AccordingtoMascarenhas et al.52 biological eventsthat
leadtotheinitiationandprogressionofMPNsarelinkednot onlytoacquisitionofgeneticmutationssuchasJAK2V617F. Theyarealsoduetoepigeneticchangesthatdonotaffectthe primaryDNAsequence,butthegeneexpressionresponsible forchromatinremodeling.Deregulationofmodulation pro-cessesbetweennucleosomesmayresultinsilencingoftumor suppressoraswellasdifferentiationgenes,promotingcell sur-vivalbyblockingapoptosis andsenescence,contributingto malignanttransformation.Theresearchersalsohighlighted
twocategoriesofepigeneticalterationsinMPNs:(1)changes inthegenesthatencodeproteinsinvolvedinremodelingof thechromatinstructure,suchastheTET2,ASXL1,JAK2genes, amongothers,and(2)changesinthepromotersiteofgenes essential for cell survival, differentiation and proliferation. Besides its role insignaling,the JAK2 V617Fmutationalso affects chromatin structure byblocking the recruitment of repressorproteins.9
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.DameshekW.Editorial:somespeculationsonthe myeloproliferativesyndromes.Blood.1951;6(4):372–5.
2.SpivakJL,BarosiG,TognoniG,BarbuiT,FinazziG,MarchioliR, etal.Chronicmyeloproliferativedisorders.HematolAmSoc HematolEducProgr.2003;2003(1):200–24.
3.FinazziG,BarbuiT.HowItreatpatientswithpolycythemia vera.Blood.2007;109(12):5104–11.
4.HaferlachT,BacherU,KernW,SchnittgerS,HaferlachC.The diagnosisofBCR/ABL-negativechronicmyeloproliferative diseases(CMPD):acomprehensiveapproachbasedon morphology,cytogenetics,andmolecularmarkers.Ann Hematol.2008;87(1):1–10.
5.denDunnenJT,AntonarakisSE.Mutationnomenclature extensionsandsuggestionstodescribecomplexmutations:a discussion.HumMutat.2000;15(1):7–12.
6.VainchenkerW,DelhommeauF,ConstantinescuSN,Bernard OA.Newmutationsandpathogenesisofmyeloproliferative neoplasms.Reviewarticle.Newmutationsandpathogenesis ofmyeloproliferativeneoplasms.Blood.2011;118(7):1723–35.
7.VannucchiAM,AntonioliE,GuglielmelliP,RambaldiA,Barosi G,MarchioliR,etal.ClinicalprofileofhomozygousJAK2 617V>Fmutationinpatientswithpolycythemiaveraor essentialthrombocythemia.Blood.2007;110(3):840–6.
8.TefferiA.Thehistoryofmyeloproliferativedisorders:before andafterDameshek.Leukemia.2008;22(1):3–13.
9.JonesAV,ChaseA,SilverRT,OscierD,ZoiK,WangYL,etal. JAK2haplotypeisamajorriskfactorforthedevelopmentof myeloproliferativeneoplasms.NatGenet.2009;41(4):446–9.
10.GäblerK,BehrmannI,HaanC.JAK2mutants(e.g.,JAK2V617F) andtheirimportanceasdrugtargetsinmyeloproliferative neoplasms.JAKSTAT.2013;2(3):e25025.
11.VardimanJW,ThieleJ,ArberDA,BrunningRD,BorowitzMJ, PorwitA,etal.The2008revisionoftheWorldHealth Organization(WHO)classificationofmyeloidneoplasmsand acuteleukemia:rationaleandimportantchanges.Blood. 2009;114(5):937–51.
12.KiladjianJJ.ThespectrumofJAK2-positivemyeloproliferative neoplasms.HematolAmSocHematolEducProgr.
2012;2012:561–6.
13.KimHR,ChoiHJ,KimYK,KimHJ,ShinJH,SuhSP,etal.Allelic expressionimbalanceofJAK2V617Fmutationin
BCR-ABL-negativemyeloproliferativeneoplasms.PLoSONE. 2013;8(1):e52518.
14.ChauffailleML.Neoplasiasmieloproliferativas:revisãodos critériosdiagnósticosedosaspectosclínicos.RevBras HematolHemoter.2010;32(4):308–16.
16.FreitasRM,SantosMO,MarandubaCM.TheJAK2geneasa protagonistinchronicmyeloproliferativeneoplasms.Rev BrasHematolHemoter.2013;35(4):278–9.
17.AxelradAA,EskinaziD,CorreaPN,AmatoD.Hypersensitivity ofcirculatingprogenitorcellstomegakaryocytegrowthand developmentfactor(PEG-rHuMGDF)inessential
thrombocythemia.Blood.2000;96(10):3310–21.
18.RöderS,SteimleC,MeinhardtG,PahlHL.STAT3is constitutivelyactiveinsomepatientswithPolycythemia rubravera.ExpHematol.2001;29(6):694–702.
19.KaushanskyK.Thechronicmyeloproliferativedisordersand mutationofJAK2:Dameshek’s54yearoldspeculationcomes ofage.BestPractResClinHaematol.2007;20(1):5–12.
20.YamaokaK,SaharinenP,PesuM,HoltVEIII,SilvennoinenO, O’SheaJJ.TheJanuskinases(Jaks).GenomeBiol.
2004;5(12):253–6.
21.CazzolaM.SomaticmutationsofJAK2exon12asamolecular basisoferythrocytosis.Haematologica.2007;92(12):1585–9.
22.WilliamsDM,KimAH,RogersO,SpivakJL,MoliternoAR. PhenotypicvariationsandnewmutationsinJAK2 V617F-negativepolycythemiavera,erythrocytosis,and idiopathicmyelofibrosis.ExpHematol.2007;35(11):1641–6.
23.LaughlinTS,MoliternoAR,SteinBL,RothbergPG.Detection ofexon12mutationsintheJAK2geneenhancedanalytical sensitivityusingclampedPCRandnucleotidesequencing.J MolDiagn.2010;12(3):278–82.
24.KjærL,WestmanM,HasselbalchRileyC,HøgdallE,Weis BjerrumO,HasselbalchH.Ahighlysensitivequantitative real-timePCRassayfordeterminationofmutantJAK2exon 12alleleburden.PLoSONE.2012;7(3):e33100.
25.SchaferAI.Molecularbasisofthediagnosisandtreatmentof polycythemiaveraandessentialthrombocythemia.Blood. 2006;107(11):4214–22.
26.SmithCA,FanG.ThesagaofJAK2mutationsand translocationsinhematologicdisorders:pathogenesis, diagnosticandtherapeuticprospects,andrevisedWorld HealthOrganizationdiagnosticcriteriaformyeloproliferative neoplasms.HumPathol.2008;39(6):795–810.
27.UngureanuD,WuJ,PekkalaT,NiranjanY,YoungC,Jensen ON,etal.ThepseudokinasedomainofJAK2isa
dual-specificityproteinkinasethatnegativelyregulates cytokinesignaling.NatStructMolBiol.2011;18(9):971–6.
28.LakeyMA,PardananiA,HoyerJD,NguyenPL,LashoTL, TefferiA,etal.Bonemarrowmorphologicfeaturesin polycythemiaverawithJAK2exon12mutations.AmJClin Pathol.2010;133(6):942–8.
29.IkedaK,OgawaK,TakeishiY.TheroleofHMGA2inthe proliferationandexpansionofahematopoieticcellin myeloproliferativeneoplasms.FukushimaJMedSci. 2012;58(2):91–100.
30.YoshimuraA,NakaT,KuboM.SOCSproteins,cytokine signallingandimmuneregulation.NatRevImmunol. 2007;7(6):454–65.
31.TamiyaT,KashiwagiI,TakahashiR,YasukawaH,Yoshimura A.Suppressorsofcytokinesignaling(SOCS)proteinsand JAK/STATpathways:regulationofT-cellinflammationby SOCS1andSOCS3.ArteriosclerThrombVascBiol. 2011;31(5):980–5.
32.MorganKJ,GillilandDG.AroleforJAK2mutationsin myeloproliferativediseases.AnnuRevMed.2008;59:213–22.
33.TanAY,WestermanDA,DobrovicA.Asimple,rapid,and sensitivemethodforthedetectionoftheJAK2V617F mutation.AmJClinPathol.2007;127(6):977–81.
34.GariM.TheroleofJanusKinase2(JAK2)inthe pathologenesisofmyeloproliferativedisorders.JKing AbdulazizUnivMedSci.2009;16(1):3–19.
35.WalzC,CrossNC,VanEttenRA,ReiterA.Comparisonof mutatedABL1andJAK2asoncogenesanddrugtargetsin myeloproliferativedisorders.Leukemia.2008;22(7):1320–34.
36.FiskusW,GangulyS,KambhampatiS,BhallaKN.Roleof additionalnoveltherapiesinmyeloproliferativeneoplasms. HematolOncolClinNAm.2012;26(5):959–80.
37.HaricharanS,LiY.STATsignalinginmammarygland differentiation,cellsurvivalandtumorigenesis.MolCell Endocrinol.2014;382(1):560–9.
38.KhwajaA.TheroleofJanuskinasesinhaemopoiesisand haematologicalmalignancy.BrJHaematol.
2006;134(4):366–84.
39.HookhamMB,ElliottJ,SuessmuthY,StaerkJ,WardAC, VainchenkerW,etal.Themyeloproliferative
disorder-associatedJAK2V617Fmutantescapesnegative regulationbysuppressorofcytokinesignaling3.Blood. 2007;109(11):4924–9.
40.NaramuraM,NadeauS,MohapatraB,AhmadG, MukhopadhyayC,SattlerM,etal.MutantCblproteinsas oncogenicdriversinmyeloproliferativedisorders.Oncotarget. 2011;2(3):245–50.
41.JiangQ,SongC,NangreaveJ,LiuX,LinL,QiuD,etal.DNA origamiasacarrierforcircumventionofdrugresistance.J AmChemSoc.2012;134(32):13396–403.
42.RawlingsJS,RoslerKM,HarrisonDA.TheJAK/STATsignaling pathway.JCellSci.2004;117Pt8:1281–3.
43.PerrottaS,CucciollaV,FerraroM,RonzoniL,TramontanoA, RossiF,etal.EPOreceptorgain-of-functioncauseshereditary polycythemia,altersCD34+celldifferentiationandincreases
circulatingendothelialprecursors.PLoSONE. 2010;5(8):e12015.
44.KralovicsR.Geneticcomplexityofmyeloproliferative neoplasms.Leukemia.2008;22(10):1841–8.
45.PloI,NakatakeM,MalivertL,deVillartayJP,GiraudierS, VillevalJL,etal.JAK2stimulateshomologousrecombination andgeneticinstability:potentialimplicationinthe
heterogeneityofmyeloproliferativedisorders.Blood. 2008;112(4):1402–12.
46.CrossNC.Geneticandepigeneticcomplexityin
myeloproliferativeneoplasms.HematolAmSocHematol EducProgr.2011;2011:208–14.
47.Pagliarini-e-SilvaS,SantosBC,PereiraEM,FerreiraME, BaraldiEC,SellAM,etal.Evaluationoftheassociation betweentheJAK246/1haplotypeandchronic
myeloproliferativeneoplasmsinaBrazilianpopulation. Clinics(SaoPaulo).2013;68(1):5–9.
48.ScottLM,RebelVI.JAK2andgenomicinstabilityinthe myeloproliferativeneoplasms:acaseofthechickenorthe egg?AmJHematol.2012;87(11):1028–36.
49.KilpivaaraO,LevineRL.JAK2andMPLmutationsin myeloproliferativeneoplasms:discoveryandscience. Leukemia.2008;22(10):1813–7.
50.PassamontiF,RumiE.ClinicalrelevanceofJAK2(V617F) mutantalleleburden.Haematologica.2009;94(1):7–10.
51.ShihAH,Abdel-WahabO,PatelJP,LevineRL.Theroleof mutationsinepigeneticregulatorsinmyeloidmalignancies. NatRevCancer.2012;12(9):599–612.