revbrashematolhemoter.2015;37(5):316–319
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Frequency
of
Wr
a
antigen
and
anti-Wr
a
in
Brazilian
blood
donors
Janaína
Guilhem
Muniz
a,∗,
Carine
Prisco
Arnoni
a,
Diana
Gazito
a,
Rosangela
de
Medeiros
Person
a,
Tatiana
Aparecida
de
Paula
Vendrame
a,
Flavia
Roche
Moreira
Latini
a,
Lilian
Castilho
baAssociac¸ãoBeneficentedeColetadeSangue(Colsan),SãoPaulo,SP,Brazil
bUniversidadeEstadualdeCampinas(Unicamp),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1June2015 Accepted3July2015 Availableonline29July2015
Keywords:
Anti-Wra Wraantigen Diegobloodgroup Allelefrequency
a
b
s
t
r
a
c
t
Background:Wraisalow-incidenceantigen,whichisantitheticaltothehighprevalence
redblood cellantigen,Wrb.Anti-Wraisanaturallyoccurringantibodythatisfoundin approximately1–2%ofblooddonors.Theaimofthisstudywastodeterminethefrequency ofWraandanti-WrainBrazilianblooddonors.
Methods:Atotalof1662Brazilianblooddonorsweremolecularlyanalyzedusingthe
SNaP-shotmethodologytodeterminetheWR*A/BallelesandtopredictthefrequencyoftheWra antigen.Todetecttheanti-Wra,samplesfrom1049blooddonorswereanalyzedusinga geltestwithWr(a+)redbloodcells.Theserumwastreatedwithdithiothreitol(DTT)to determinetheimmunoglobulinclasses.Immunoglobulin(Ig)-Gisotypeclassificationwas performedinageltestusingtheIgG1/IgG3card.Amonocytemonolayerassaywasemployed topredicttheclinicalsignificanceofIgGanti-Wra.
Results:Ofthe1662donors,onlyonesamplehadtheDI*02.03alleleinheterozygous
predict-ingtheWr(a+b+)phenotype.Anti-Wrawasdetectedin34(3.24%)samples,64.7%infemales and35.3%inmales.Regardingtheimmunoglobulinclass,eight(23.5%)casesofanti-Wra wereclassifiedasIgGand26(76.5%)asIgM.OftheeightcasesofIgGanti-Wra,fourwere IgG1,twowereIgG3andthreeanti-WrawerenotIgG3orIgG1,andthusprobablyIgG2or IgG4.TheresultsofthemonocytemonolayerassayshowedthatIgGanti-Wramightbeof clinicalsignificance.
Conclusion:Thisstudyshowsaverylowfrequency(0.06%)oftheWraantigeninBrazilian
blooddonors.Additionally,itshowsthatthefrequencyofanti-Wrainthispopulationis higherthanpreviouslyreported.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:Colsan–Associac¸ãoBeneficentedeColetadeSangue,Av.Jandira1260,Indianópolis,04614-013SãoPaulo,SP,
Brazil.
E-mailaddress:[email protected](J.G.Muniz).
http://dx.doi.org/10.1016/j.bjhh.2015.07.002
revbrashematolhemoter.2015;37(5):316–319
317
Introduction
TheDiegobloodgroupsystemiscarriedonband3,a multi-passmembraneglycoprotein,whichisencodedbytheSLC4A1
gene.TheDiegosystemiscomposedof22antigens:threepairs ofantitheticalantigens,DiaandDib,WraandWrb,Wuand DISK,and16verylowfrequencyantigens.1WraandWrb anti-gensarerelatedtoaSNPinexon16(1972G>A)thatencodesa LysineinWraoraglutamicacidinWrbataminoacidposition 658.2
TheWraantigen,firstdescribedbyHolmanin1953,hasan incidenceofaround1in1000inCaucasianpopulations,butit isnotreportedinotherethnicgroups.3AlthoughtheWra anti-genhasaverylowincidence,anti-Wraisarelativelycommon antibodysinceitisoftenanaturallyoccurringantibody.4The describedincidenceofanti-Wraintheseraofnormaldonors variesindifferentstudies;ithasbeenestimatedat1of100 inhealthyvolunteerblooddonors.5Theimmunoglobulin(Ig) classofanti-WracanbeIgM,IgGorIgMplusIgG.Alloanti-Wra israrelyinvolvedinhemolytictransfusionreactions,however therearesomecasesreportinghemolyticdiseaseofthefetus andnewborn(HDFN)causedbyanti-Wra.1
Antibodiesagainstlow-incidenceantigens,including anti-Wra,aredifficulttoidentify,becausethescreeningandpanel cellsrarelyexpresstheseantigens.6,7 Hence,littleisknown aboutthe frequencyofanti-Wra inmany populations. The knowledgeofthemolecularbasisoftheDiegobloodgroup systemandthedevelopmentofmolecularassaystoidentify theDIalleleshasallowedthefrequencyoftheseallelestobe assessedindifferentpopulations.Theaimofthisstudywas todeterminethefrequencyoftheWraantigenandanti-Wra inaBrazilianpopulationofblooddonors.
Methods
Atotalof1662bloodsampleswereobtainedfromhealthy vol-unteerBrazilianblooddonorsattheAssociac¸ãoBeneficente
deColetadeSangue(Colsan),SãoPaulo,Brazil.The popula-tionstudiedwasfromSoutheastofBrazilanditiscomposed ofahighlyadmixedpopulation.
Molecularanalysis
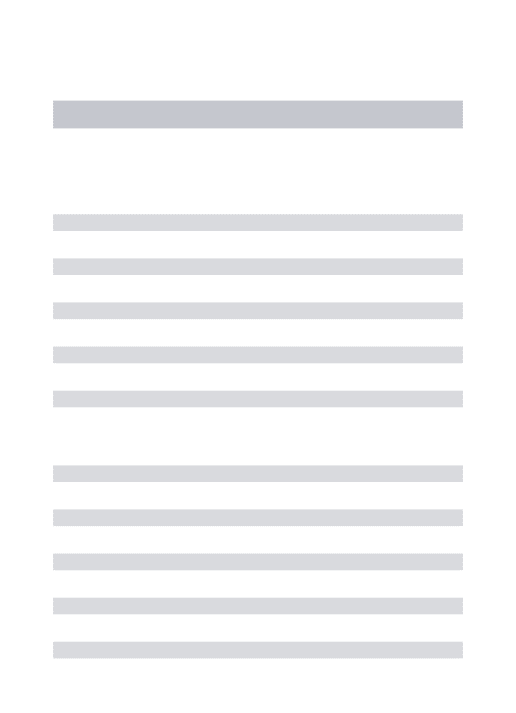
DNAwasextractedusingtheQIAmpDNAMiniKit(Qiagen® Inc. Valencia, CA, USA) according to the manufacturer’s instructions. To determine the WR*Aand WR*B alleles and predictthefrequencyoftheWraantigen,genotypingwas per-formedusingapreviousdescribedSNaPshot®protocol(Latini etal.8).Fragmentanalyseswereperformedina3500xLGenetic Analyzer(AppliedBiosystem,FosterCity,CA,USA)asshown inFigure1.
Antibodyscreening
Inordertoinvestigatetheoccurrenceofanti-Wra,serum sam-plesfrom1049blooddonors(638maleand411femaledonors) wereinitiallycross-matchedwithaWr(a+)redbloodcell(RBC) from our collection in a gel test by an automated system (WADiana® 8XT, Grifols,Barcelona,Spain). Thepresenceof anti-Wra inpositivecross-matcheswasconfirmedwithtwo sources ofWr(a+) RBCs from commercial panels(BioRad®, LagoaSanta,Brazil).
Immunoglobulinclasses
To determine the Ig classes (IgG or IgM), the serum was treatedwithdithiothreitol (DTT,Sigma-Aldrich, Brazil).The IgG isotypeclassificationwasperformedinageltestusing theIgG1/IgG3card(BioRad®,LagoaSanta,Brazil).
Monocytemonolayerassay
To predict the clinical significanceof anti-Wra, the mono-cyte monolayer assay (MMA)was performed as previously described9intwosampleswithanti-WraclassifiedasIgG1and onesampleclassifiedasIgG3.Usinganopticalmicroscopy,600
1200
DI*4
DI*3
DI*2 YT*1
CO*1 KEL*7
KEL*4 DO*2
DO*5
DO*4
Vel+ 1000
800
600
400
200
0
318
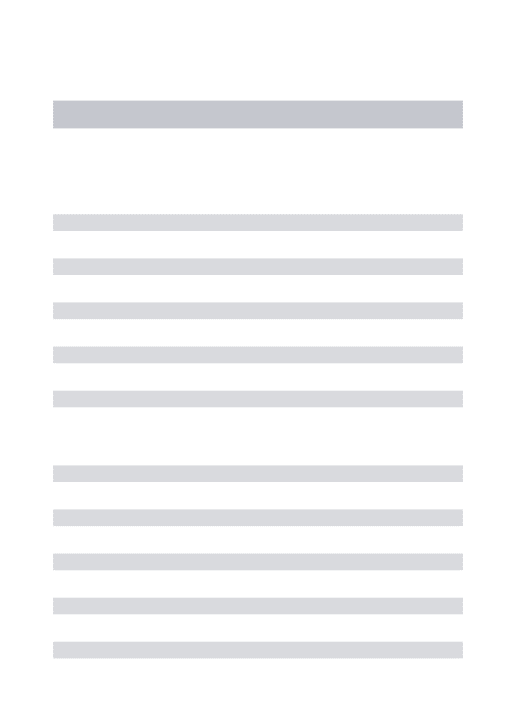
revbrashematolhemoter.2015;37(5):316–319Figure2–Monocytemonolayerassayslides(1000×).(A)Negativecontroland(B)Monocytemonolayerassaywithanti-Wra.
monocyteswerecountedtodeterminethepercentageof reac-tivemonocytes(RBCadheredandphagocytized).MMAresults <4%wereconsiderednegativewhileresults≥4%were
consid-eredpositive.
Results
Wraantigen
Ofthe1662genotypedbloodsamples,onlyonesample pre-sentedtheWR*Aalleleinheterozygous.Itwasgenotypedas
WR*A/WR*BpredictingtheWr(a+b+)phenotype.
Anti-Wra
Anti-Wra was detected in 34 samples from 1049 screened blooddonorsrepresentingafrequencyof3.24%.Regardingthe Igclasses,8/34(23.5%)wereIgGand26/34(76.5%)wereIgM.Of theeightIgGanti-Wra,fourwereclassifiedasIgG1andone wasisotypedasIgG3.Threesampleswere notclassified as IgG1orIgG3;theseareprobablyIgG2orIgG4,Igclassesthat arenotinvolvedinseveretransfusionreactions.Asshownin
Table1,ahigherfrequencyofanti-Wrawasobservedinfemale donors(p=0.0036,Fisher’sexacttest).
Table1–Frequencyofanti-Wraandimmunoglobulin(Ig)
class.
Igclass Isotype Donor Total
Female Male
IgG IgG1 3 1 4
IgG3 0 1 1
IgG2orIgG4 3 0 3
IgM – 16 10 26
Total 22 12 34
MMAresults(Figure2)showthatWraantibodiesclassified asIgGcanpotentiallybeclinicallysignificant,asIgG1 antibod-iespresented7–7.5%ofreactivemonocytesand12.7%ofIgG3 hadreactivemonocytes.
Discussion
Thisstudyshowsnovelinformationregardingthepresenceof anti-WrainaBrazilianpopulationofblooddonors.Although thefrequencyoftheWra antigen(1:1662)islowerthanthat previouslyreportedinEuropeans(1:1000),3theoccurrenceof anti-Wra washigher(1:31)whencomparedtootherstudies whereitrangedfrom1in80to1in200.Thefrequencyof anti-WrafoundinthisstudyissimilartothatfoundinSpain(1:37), howeverthepresenceoftheantigeninSpanishpopulationis around2-times(1:785)6thefrequencyfoundinBrazilians.
Themechanismsinvolvedinanti-Wraproductionarestill unclear. Some authors believe that, besidesthe alloimmu-nization in response to antigenexposure, certain proteins
that can cross-react with the Wra antigen are formed
whentheimmunesystembecomesmoreactive.7Situations described to beinvolved inanti-Wra alloimmunization are also related to immune system activation, including
preg-nancy, autoimmune hemolytic anemia and patients with
otherRBCantibodies.7Therefore,ourhypothesisisthatthe differenceinanti-Wradistributionbetweengenderscouldbe associatedto pregnancy, asanti-Wra was foundin5.2%of
womenand1.8%ofmen.
revbrashematolhemoter.2015;37(5):316–319
319
canbeofclinical significance.Due tothelow incidenceof theWraantigenand the lowriskofhemolytictransfusion reaction,theuseofscreeningpanelscontainingWr(a+)RBCs isnotrequired. TherebyWra incompatibletransfusion can occur,but fewcasesofhemolytictransfusionreactionwere described,beenestimatedtobe1in500,000.11
Insummary,theWraantigenhasaverylowfrequencyin Brazilianblooddonorsandanti-Wrahasahigherfrequency thanreportedinotherpopulations.Consideringthelow fre-quencyoftheantigenandthefewcasesofmildHDFNrelated toanti-Wra,clinicalimpactisdiscussableaswellthe require-mentofRBCreagenttoidentifythem.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. ReidME,Lomas-FrancisC,OlssonML.Thebloodgroup antigenfactsbook.ThirdEditionElsevier:AcademicPress; 2012.
2. BruceLJ,RingSM,AnsteeDJ,ReidME,WilkinsonS,TannerMJ. ChangesinthebloodgroupWrightantigensareassociated withamutationataminoacid658inhumanerythrocyte
band3:asiteofinteractionbetweenband3andglycophorin Aundercertainconditions.Blood.1995;85(2):541–7.
3.DanielsG.Humanbloodgroups.2nded.Bristol:Blackwell Science;2002.
4.WallisJP,HedleyGP,CharltonD,ParkerPC,ScottY,Chapman CE.Theincidenceofanti-WraandWraantigeninblood donorsandhospitalpatients.TransfusMed.1996;6(4):361–4.
5.GarrattyG.ScreeningforRBCantibodies-whatshouldwe expectfromantibodydetectionRBCs.Immunohematology. 2002;18(3):71–7.
6.ArriagaF,LlopisF,delaRubiaJ,CarpioN,MoscardóJ,Marty ML.IncidenceofWraantigenandanti-WrainaSpanish population.Transfusion.2005;45(8):1324–6.
7.SchonewilleH,vanZijlAM,WijermansPW.Theimportance ofantibodiesagainstlow-incidenceRBCantigensincomplete andabbreviatedcross-matching.Transfusion.
2003;43(7):939–44.
8.LatiniFR,GazitoD,ArnoniCP,MunizJG,deMedeirosPerson R,CarvalhoFO,etal.Anewstrategytoidentifyrareblood donors:singlepolymerasechainreactionmultiplexSNaPshot reactionfordetectionof16bloodgroupalleles.Blood Transfus.2014;12Suppl.1:s256–63.
9.NanceSJ,ArndtP,GarrattyG.Predictingtheclinical significanceofredcellalloantibodiesusingamonocyte monolayerassay.Transfusion.1987;27(6):449–52.
10.HoffmannJJ.Anti-Wr(a):toscreenornottoscreen? Transfusion.2007;47:948–9,discussion9.