www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Swallowing
and
pharyngo-esophageal
manometry
in
obstructive
sleep
apnea
夽
,
夽夽
Luciana
Almeida
Moreira
da
Paz
Oliveira
a,b,∗,
Luiz
Henrique
de
Souza
Fontes
c,
Michel
Burihan
Cahali
a,daDepartmentofOtorhinolaryngology,HospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil bHealthSciences,HospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil
cDepartmentofGastroenterology,HospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil
dDepartmentofOtorhinolaryngology,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,
SP,Brazil
Received16February2014;accepted29June2014 Availableonline30March2015
KEYWORDS Obstructivesleep apnea;
Deglutitiondisorders; Manometry;
Pharynx; Esophagus
Abstract
Introduction:Upperairwaynerveandmuscledamageassociatedwithobstructivesleepapnea mayimpairthestrengthanddynamicsofpharyngealandesophagealcontractionsduring swal-lowing.
Objective:To evaluate the presence of alterations in pharyngoesophageal manometry in patientswithobstructivesleepapneawithandwithoutoropharyngealdysphagia.
Methods:Thisstudyprospectivelyevaluated22patientswithobstructivesleepapneawithout spontaneouscomplaintsofdysphagia,usingaquestionnaire,fiberopticendoscopicevaluation ofswallowing,andpharyngoesophagealmanometry,includingmeasurementoftheupperand loweresophageal sphincterpressuresandmean pharyngealpressuresatthreelevelsduring swallowing.
Results:Thedysphagiagroupconsistedof17patients(77.3%)inwhomswallowing abnormali-tiesweredetectedonfiberopticendoscopicevaluationofswallowing(n=15;68.2%)and/orin thequestionnaire(n=7;31.8%).Thefiveremainingcasescomprisedacontrolgroupwithout oropharyngealdysphagia.Inallcasesofabnormalitiesonfiberopticendoscopicevaluationof swallowing,therewas prematurebolusleakageinto thepharynx.Therewasnostatistically significantdifferencebetweenthegroupsregardinganyofthepharyngoesophagealmanometry measurements,age,orseverityofobstructivesleepapnea.
夽
Pleasecitethisarticleas:OliveiraLA,FontesLH,CahaliMB.Swallowingandpharyngo-esophagealmanometryinobstructivesleepapnea. BrazJOtorhinolaryngol.2015;81:294---300.
夽夽
Institution:HospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil. ∗Correspondingauthor.
E-mail:[email protected](L.A.M.d.P.Oliveira).
http://dx.doi.org/10.1016/j.bjorl.2015.03.006
1808-8694/©2015Associac¸ãoBrasileiradeOtorrinolaringologia eCirurgiaCérvico-Facial. PublishedbyElsevierEditoraLtda.All rights
Conclusion: Pharyngoesophageal manometry detected no statistically significant difference betweenthegroupswithandwithoutoropharyngealdysphagia.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Apneiadosonotipo obstrutiva;
Transtornosde deglutic¸ão; Manometria; Faringe; Esôfago
Deglutic¸ãoemanometriafaringoesofágicanaapneiaobstrutivadosono
Resumo
Introduc¸ão: Lesõesneurogênicasemuscularesassociadasàapneiaobstrutivadosonopodem comprometeraforc¸aeadinâmicadascontrac¸õesfaríngeaseesofágicasduranteadeglutic¸ão.
Objetivo: Verificarseháalterac¸õesnamanometriafaringoesofágicadepacientescomapneia obstrutivadosonocomesemdisfagiaorofaríngea.
Método: Foram avaliados, prospectivamente, 22 pacientes com apneia obstrutiva do sono sem queixaespontânea dedisfagia, utilizando questionário, videoendoscopiada deglutic¸ão emanometriafaringoesofágica,commedidasdaspressõesdoesfíncteresofagianoinferiore superiorepressãomédiadafaringeemtrêsníveisduranteadeglutic¸ão.
Resultados: 17pacientes(77,3%)formaramogrupocomdisfagia,porapresentaremalterac¸ões de deglutic¸ão navideoendoscopia dadeglutic¸ão (n=15; 68,2%)e/ou noquestionário (n=7; 31,8%).Oscincorestantescompuseramogruposemdisfagiaorofaríngea.Emtodososcasos comalterac¸õesnavideoendoscopiadadeglutic¸ãohouveescapeprecocedoboloalimentarpara afaringe.Nãohouvediferenc¸asignificanteentreosgruposcomesemdisfagiaemrelac¸ãoa todasasmedidasdemanometria,idadeegravidadedaapneiaobstrutivadosono.
Conclusões: A manometria faringoesofágica não demonstrou diferenc¸a significante entreos gruposcomesemdisfagiaorofaríngea.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Neurallesionsin thesoftpalateandoropharynxaresome ofthealterations foundinpatients withobstructivesleep apnea(OSA) andprimarysnorers.1---3Some authorsbelieve that these lesions are triggered by low frequency vibra-tions producedby snoring or intermittenthypoxia related toOSA.4---6 Thesoftpalate mucosainprimarysnorerswith OSAshowsanincreasednumberofabnormalnerveendings.1 Thepalatopharyngeal muscle,both inprimarysnorersand inpatientswithOSA,showsmorphologicalalterationsthat aretypicalofperipheralnerveinjury,suchasgroupingof tis-suesbyfibertype,clustersofatrophiedareas,andfascicular atrophy.2
Thepresenceofneurologicaldisordersinthepharynxof patientswithOSAcancauseswallowingprocessdysfunction, astheinitiationoftheswallowingreflexandpropagationof the foodbolus depends onadequate sensitivity(afferent) andpharyngealfunction.Additionally,itisbelievedthatthe perpetuation ofOSA impairsneuromuscularafferent stim-ulation of the upper airways and the central integration betweenswallowingandbreathingfunctions.7---12
The evaluation ofswallowing usingvideofluoroscopyor fiberoptic nasal endoscopy shows a high prevalence of alterationsinpatients withprimarysnoringor OSA.These alterationscanbesymptomatic orasymptomatic and con-sistmostlyofprematurebolusleakage(fromtheoralcavity into the pharynx) and food residue in the pharynx after swallowing.9,10,13,14
Pharyngoesophageal manometry assesses the compres-sivemuscleforceofthepharyngealandesophagealmuscles duringswallowing,aidingintheunderstandingofthe phys-iopathologyoforopharyngealdysphagia.15---17Hypothetically, neurologicaland muscular disorders of the upper airways associatedwith OSA18 can impair theforce and dynamics ofpharyngoesophagealcontractionsduringswallowing, con-tributingtothedysphagiaobservedin manycasesofOSA. Tothebestoftheauthors’knowledge,nostudieshave per-formedmanometricevaluationsofthepharyngealphaseof swallowinginpatientswithOSA.
TheobjectiveofthisstudyofpatientswithOSA,wasto evaluatewhetherswallowingpressuresinthepharynxand esophagusarelowerinpatientswithoropharyngeal dyspha-giacomparedtothosewithoutoropharyngealdysphagia.
Methods
Subjects
thosewithclinicallyknowndysphagiawereexcluded.This studyalsoexcludedpatientswithneuromuscularor rheuma-tological disease, Downsyndrome, acquired or syndromic facialdeformities,useofdrugsthatinterferedwithmuscle tone, previous esophageal surgery, and those with symp-tomsofgastroesophagealrefluxdisease.Thisstudyispart of a research protocol to evaluate the effect of pharyn-gealsurgeryonswallowing.ItwasapprovedbytheEthics Committeeofthisinstitution (protocol003.0.388.000-10), registeredinClinicalTrials(NCT01335594),andallpatients signedaninformedconsent.
The diagnosis of OSA was based on the presence of characteristic symptoms and findings from a supervised overnight polysomnography evaluation carried out in the sleeplaboratory.Thepatientgroupconsistedof17menand fivewomen, withamean age of 48.4years (range27---62 years),bodymassindex(BMI)of29.0kg/m2(ranging from 25to35.1kg/m2),andmeanneckcircumferenceof41.5cm (range36---48cm). Six patients(27.3%) had systemic arte-rialhypertensionandthreeweresmokers(13.6%).Regarding thepharyngealanatomy,19hadgradeIorIIpalatinetonsils (8.4%)andthreehadgradeIIIorIVtonsils(13.6%).20
Themeanapnea---hypopneaindex(AHI)was40.7(range 7.2---89.4), with 16 patients (72.7%) with severe AHI (AHI >30),three(13.6%)withmoderateAHI(AHI≤15≤30),and
three(13.6%)withmildAHI(5≤AHI<15).Themean
mini-mumoxyhemoglobinsaturationwas77.6%(range51---88%). TheEpworthsleepinessscale(ESS)showedameanscoreof 15inthisseries,rangingfrom4to19,withninecases(40.9%) showingexcessivesleepiness(Epworth>10).
The patients weredivided intotwogroups, those with dysphagiaandthosewithoutdysphagia,basedonthe assess-mentoftheswallowingquestionnaireandvideoendoscopy ofswallowing(VES).Patientswereconsideredasdysphagic whentheyshowedalterationsin thequestionnaireand/or VES.Incontrast,patientswithnormalVESandquestionnaire comprisedthegroupwithoutdysphagia.
Questionnaire
All patients answered a questionnaire13 (Table 1) that included six questions about symptoms of dysphagia perceived by the patient in the previous month. The responseswerescoredusingascaleof0---3,where0meant ‘‘never’’,1‘‘rarely’’,2‘‘often’’,and3‘‘always’’.Ascore of2or3inatleastoneofthequestionswasconsideredas indicativeofthepresenceofdysphagia.
Fiberopticendoscopicevaluationofswallowing (FEES)
VESwasperformed21inallpatients,usinga3.2-mmflexible endoscope(Pentax---Japan),introducedthroughthewider nasalcavity withouttheuseoftopicalanestheticinorder not to alter the upper airway mucosa sensitivity. The patient remained in a comfortable sitting position, with mild ventroflexion simulating a meal position, while the pharynxandlarynxwereassessed.
At the basal evaluation, the upper aerodigestive tract anatomy was assessed, as well as the presence of sali-varystasis, laryngeal sensitivity(test of glottaladduction
toendoscopetouch),mobility,andappearanceofthevocal foldsandvelopharyngealclosureduringphonationand swal-lowingofsaliva.
Under direct visualization through the endoscope, the dynamic assessment was performed for each patient dur-ingtheswallowingoffoodscoloredwithbluefoodcoloring, at room temperature, administered separately at three different consistencies (liquid,semi-solid,and solid).The completeswallowingofeachconsistencywasassessedthree times, totaling nine swallowing analyses. The liquid con-sistency comprised 5mL, 10mL, and 15mL of artificially flavoredstrawberrydrink(Clightbrandpowderedsoftdrink, strawberry flavor; Kraft Foods Brazil SA --- Curitiba, PR, Brazil)ateachtime.
The semi-solid food consisted of artificially flavored strawberry mixed with a thickening agent (BioSen NutriSenior®, Taboão da Serra, SP, Brazil), adminis-teredthreetimesusingatablespoon.Forsolidfood,three 2.5cm×2.5cmcrackersweregiventopatients.
TheexaminationswererecordedonDVDfor reanalysis. The authorsclassifiedthefollowingparametersaspresent orabsent:(a)prematureleakage:thefoodbolusleavesthe oralcavityandreachesthepharynxbeforetheswallowing reflexistriggered;(b)velopharyngealdysfunction:thesoft palatedoesnotfullyoccludethenasopharynxduring swal-lowing,allowingfoodleakage;(c)laryngealpenetration:the foodentersthelarynx,butdoesnotcrosstheglottis;(d) tra-chealaspiration:thefoodentersthelarynxandgoesthrough theglottis;(e)food residueafterswallowing:presence of somefoodinthepharynxafterthreecompleteswallowing movements.Thepresenceofprematureleakagewas consid-eredwhenitoccurredinatleasttwoofthenineswallowing analyses;asfortotheotheralterations,theiroccurrencein oneserieswassufficienttobeclassifiedaspresent.
Additionally,weevaluatedwhetherthecoughreflexwas associated with the penetration and/or aspiration events andwhetheritwaseffectiveineliminatingthepenetrated and/or aspirated content, aswell asthenumber of spon-taneousorrequestedswallowingmovementsnecessaryfor completeclearingofthefoodbolus(whichwasconsidered abnormalwhenthereweremorethanthree).
The presence of any alterationin the dynamic assess-mentplacedthepatientinthedysphagiagroup.Dysphagia severitywasnotassessed.
Pharyngoesophagealmanometry
Table1 Swallowingassessmentquestionnaire.Score:0=never,1=rarely,2=often,3=always.Thepresenceofscores2or3 atanyquestionsignifiesclinicallypresentdysphagia.
Questions Score
1.Doyouchokeonliquidsduringmeals? 0 1 2 3
2.Doyouchokeonsemi-solidfoodduringmeals? 0 1 2 3
3.Doyouchokeonsolidfoodduringmeals? 0 1 2 3
4.Doyoufeelthefoodwentdownthewrongplace? 0 1 2 3
5.Doyoufeelthefoodstuckinyourthroat? 0 1 2 3
6.Doyoufeelthefoodiscomingbackthroughyournose? 0 1 2 3
The catheterwasintroduced throughthenose intothe stomach,whichwaslocatedbyassessingthepressure mea-suredbythedevice.Then,theLESwasassessedusingthe slow withdrawal technique, i.e., pullingout the catheter 1cm ata timewiththenostril asthe pointof reference. The zero reference of the examination is the intragas-tricpressure, whichis thegastric baseline.The pressures increase in theLES and decreaseagain in the esophageal body(esophagealbaseline),increasingagainintheUES.The pressuresintheLESarehigherduringinspirationandlower duringexpiration.
The LES pressure, obtained in the region with higher pressures overthreetofivestablerespiratorycycles,was calculatedasthedifferencebetweentheintragastric pres-sureandthemaximumLESpressureduringexpiration,and considered by thesimple arithmeticmean of pressuresin eachofthefourchannelsonthecathetertip,yieldingthe maximalexpiratorypressure(MEP).ThemeanLESpressure betweenexpirationandinspirationcorrespondstothemean respiratory pressure (MRP).Values below the normal MEP and/or MRPvaluesindicateLES hypotonia. Therelaxation oftheLESwasassessedduringwetswallowing.22,23
For the study of UES, the authors also used the four more distal catheter radial openings and the same slow withdrawal technique. The resting pressure of the UES wasanalyzed,andrepresentedthedifferencebetweenthe esophagealbaselineandthemanometrictracing.Thiswas measuredatthepointofthehighestandmoststable pres-sure.TherelaxationoftheUESwasevaluatedatthepointof highestpressure,withthreeswallowingmovementsof5mL ofwater.24
The pharynxwasevaluatedwiththe radialchannelsin threedifferentpoints,located2cm,4cm,and6cmabove theupperborderoftheUES.Theamplitudeofpharyngeal contractionwasdetermined,whichrepresentedtothe dif-ferencebetweenthepharyngealbaselineandthemaximum wavepeakstudied.Forthatpurpose, swallowingpressure measurementswereconductedthreetimesat eachpoint, withtheintakeof5mLofwater,andconsideringthemean value of the three swallowing movements at each point (meanpharyngealpressure---MPP).
Statisticalanalysis
Spearman’s correlation was usedto study the association between quantitative variables. Regarding thequalitative variables,Fisher’sexacttestwasusedtoverifyassociations. Wilcoxon’srank-sumtestwasusedtostudytheassociation
Table 2 Alterations found in the Fiberoptic endoscopic evaluationofswallowing(FEES)inthe22 patientsstudied (totalof15caseswithalterations).
FindingsatVESS Numberofpatients(%)
Prematurebolusleakage 15(68.2) Bolusresidueinthe
pharynx
5(22.7)
Laryngealpenetration 3(13.6) Changesinanatomy
(Reinke’sedema)
1(4.5)
between qualitative and quantitative variables. The 95% confidenceintervalforproportionswascalculatedfor quali-tativevariables.Thesignificancelevelusedinthetestswas 5%,alwaysconsideringatwo-tailedalternativehypothesis.
Results
Of the 22 patients assessed, 17 (77.3%) had dysphagia; two(9.1%) due to alterations detected only in the swal-lowingquestionnaire, 10(45.5%)due toalterations inthe VES,andfive(22.7%)withalterationsinboth theVESand thequestionnaire.Thedysphagiagrouphadameanageof 48.6years,with12men(70.6%),ameanAHIof 41.7/h,a meanBMI of28.6kg/m2, anda meanneck circumference of 40.9cm. The non-dysphagia group (five cases; 22.7%) had a mean age of 47.6 years (p=0.70), with five men (100%) (p=0.29), a mean AHI of 37/h (p=1.00), a mean BMI=30.4kg/m2(p=0.32),andameanneckcircumference of43.5cm(p=0.10).
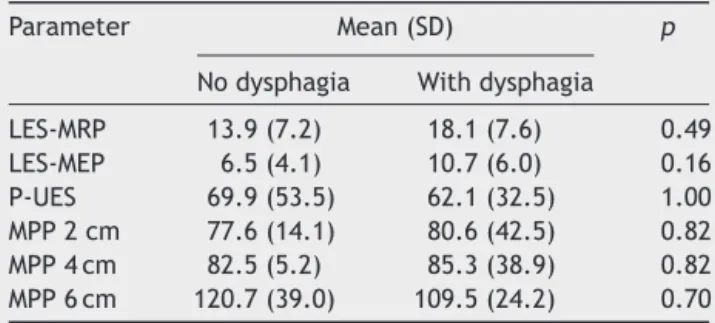
Table3 Comparisonbetweengroupswithandwithout dys-phagia regarding manometric measurements inthe lower esophageal sphincter (LES), upper esophageal sphincter (UES),andthepharynxatthelevelsof2cm;4cm,and6cm abovetheUES.
Parameter Mean(SD) p
Nodysphagia Withdysphagia
LES-MRP 13.9(7.2) 18.1(7.6) 0.49 LES-MEP 6.5(4.1) 10.7(6.0) 0.16 P-UES 69.9(53.5) 62.1(32.5) 1.00 MPP2cm 77.6(14.1) 80.6(42.5) 0.82 MPP4cm 82.5(5.2) 85.3(38.9) 0.82 MPP6cm 120.7(39.0) 109.5(24.2) 0.70
LES,loweresophagealsphincter;MRP,meanrespiratory pres-sure;MEP,maximalexpiratorypressure;P,pressure;UES,upper esophageal sphincter; MPP, mean pharyngeal pressure; SD, standarddeviation.
pharyngoesophageal manometry measurements (Table 3). Thedysphagia grouphad eightcases(47.1%)of LES hypo-tonia,twocases(11.8%) of UES hypertonia,andone case (5.9%) of UES hypotonia, but with normal UES relaxation and coordinated with the pharynx in all cases. In the non-dysphagia group, there were four cases (80%) of LES hypotonia(p=0.32) andonecase (20%)of UEShypertonia (p=1.00),alsowithnormalUESrelaxationandcoordinated withthepharynxinallcases.
The correlation between the variablesUES, LES, mean pharyngeal pressure, questionnaire results, and VES find-ings, aswell asbetween them and the variablesage and AHIwereassessed.Theonlystatisticallysignificantfinding wasthecorrelationbetweenlaryngealpenetrationandage. Patientswithlaryngeal penetrationwereolder (meanage 60 years, SD=0.00) compared to those without laryngeal penetration(meanage46.5years,SD=9.7;p=0.01).
Discussion
In this series of consecutive cases, a high frequency of dysphagia in the group of adult patients with OSA that weresnorers wasobserved, with31.8%of patients repor-tingsymptomsofdysphagiaand45.5%showingalteredVES without clinicalsymptoms. All68.2% ofcases with abnor-malVEShadprematureleakageofthefoodbolusbetween theoralcavityandthepharynx.Thismaysuggestan impair-mentintheafferentsensoryfunctionoftheoropharyngeal mucosaororalphasedysfunction,attheapproximationof theposteriorpartofthetonguewiththesoftpalate.
Whenprematureleakageoccurs,masticationand breath-ingarenotinhibited,andthus, thereis arisk oftracheal penetrationoraspiration.25Thepharyngealandesophageal manometryshowednodifferencesbetweenthegroupswith andwithoutdysphagia,aswellasthedemographic, anthro-pometric,andpolysomnographicdata.Thesefindingsseem tofavortheroleofneurogenicalterationsasthecauseof oropharyngealdysphagiainOSA,tothedetrimentoftherole ofpharyngealmusclealterations.1,2Totheauthors’ knowl-edge,thisis thefirststudy thatmeasured thepharyngeal pressureofswallowinginpatientswithOSA.
Although nodifferences were found regarding the age of patients with and without alterations in VES, those withlaryngeal penetrationwere older thanthosewithout it. Swallowing assessment through videofluoroscopy with barium showed that among snoring patients with OSA, dysphagia appeared in older patients, regardless of OSA severity.10 Studies in healthy individuals have shown that aging is associated with a higher frequency of penetra-tionandaspirationcomparedtoyoungadults,butwithout excludingpatientswithsnoringandapnea.26,27One hypoth-esis that could be raised is that older patients have had a longer exposure tovibration trauma caused by snoring, resultinginmoresevereswallowingalterations.
Although the present study favorsthe hypothesis of a peripheralcausefor dysphagiainOSA,thissubjectis con-troversialintheliterature.Teramotoetal.showedthatthe latencyofthepharyngealswallowingreflexwasincreased, which required alargervolume offood inthe pharynxto triggerthereflexinpatientswithOSA.7Jobinetal.founda significantreductionintheswallowingreflexlatencyinOSA, suggesting theimpairmentoftheinhibitorymodulation of thereflexandcentralcontrolofswallowing.8
Snorers without9,10 and with OSA9,10,14 show subclini-calswallowingalterations between52% and64%of cases, comparabletothe45.5%foundinthepresentstudy. Appar-ently,theriskofdysphagiainsnorersdoesnotcorrelatewith the presence or severity of OSA,10 indicating the harmful roleoftissuevibrationcausedbysnoring,leadingtonerve damage in the upper airways, which would contribute to dysphagia.28Therewasnocorrelationbetweentheseverity ofOSAandthepresenceofdysphagiainthepresentstudy.
Itwasobserved that,ingeneral,the complaintof dys-phagiawasnotspontaneously mentionedby patientswith OSA,butwhenperceived,italertedpatientstoother poten-tial impacts of OSA on their quality of life, acting asan additionalmotivatorforseekingandadheringtotreatment. This aspect is often ignored in the management of OSA; specific treatments for swallowing, such as the teaching ofmaneuvers,posturaladjustments,facilitationtherapies, and changes in diet consistency can also have a positive impactonqualityoflifeofthesepatients,similartowhat occursinpatientswithdysphagiasecondary toParkinson’s disease.29,30
Amongthe 31.8%cases withdysphagia complaints, the majority(27.3%)reportedhavingthesensationoffoodstuck in thethroat. Inclinical practice,this symptomis usually attributed to pharyngolaryngeal reflux. However, pharyn-geal dysphagia is often a slowly progressive disorder, in which the individual develops compensatory mechanisms suchasdietchangesormasticationvelocity.Thus,the symp-tomsmayappearonlywhenthecompensatorystrategiesno longerovercometheintensityofthedisorder.Priortothat, anactivemedicalinterventioncanalreadydetectimpaired swallowing.31 Thus, the early and adequate treatment of snoringandOSAcanpreventthedevelopmentofpharyngeal dysphagia.Theliteraturehasareportoftwocasesofsevere OSAthatshowedimprovementofdysphagiaafteroneyear oftreatmentwithcontinuousnasalpositiveairwaypressure (CPAP)andweightloss.32
completion of the swallowing movement and resumption ofbreathing,possiblyindicatingalterationsinperistalsisor pharynxelevation,astheUESrelaxationwasnotdifferent between the groups. To the best of the authors’ knowl-edge, the normal values for pharyngeal pressure in this populationareunknown,althoughthereareinitialstudies withtheJapanesepopulation.33Asmuchofthepharyngeal swallowing pressure is exerted by the tongue, whose electromyographicactivityisincreasedduringwakefulness inpatientswithOSA,34itisconsideredunlikelythat pharyn-geal manometry willshow alterations infuture studiesof OSA cases,unlike previous studieswith myastheniagravis andHuntington’sdisease,whicharecharacterizedbymajor alterationsinmusclestrength.35,36
Esophagealpressuremeasuresdidnotdifferbetweenthe groupswithandwithoutdysphagia.ThefindingofLES hypo-tonia,whichcanbeassociatedwithgastroesophagealreflux disease(GERD),37waspresentinbothgroups(p=0.32),but sinceitwasanexclusioncriteria,ourpatientshadno symp-toms suggestive of the disease. The association between GERDandOSAhasbeendescribedintheliterature,38,39but wasnotevaluatedinthisstudy.
We recognize that this study has some limitations. A largerpatientgroupwithoutdysphagiaperhapscouldhave revealedsomestatisticaldifferencesthatwerenot demon-stratedinthisanalysis.Additionally,theinclusionofagroup ofprimarysnorersandacontrolgroupneithersnored snor-ersnorhadOSApatientswouldhelptoclarifytherolesof OSAandsnoringinthedysphagiathesepatientsexhibited, perhaps demonstratingdifferencesinpharyngeal swallow-ingpressures between thegroups. The use of avalidated questionnaire would be more appropriate, but the study was based on a simpler questionnaire used in a similar studysincethesepatientsdidnothavemanycomplaintsof dysphagia.Anotherlimitationwasthefactthatsolid-state esophageal manometry which is superior when assessing rapid high-pressure events that occur in the pharynx was notavailable.15,33However,theperfusionmethodwas per-formedbyanexperiencedgastroenterologistwhopersonally conductedtheexaminationinallpatients.
Conclusion
ThisstudyfoundthatamongpatientswithOSA,therewasno significantdifferenceinswallowingpressuresofthepharynx and esophagus between subjects with and without orop-haryngealdysphagia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FribergD,GazeliusB,HökfeltT,NordlanderB.Abnormal affer-entnerveendingsinthesoftpalatalmucosaofthesleepapneics andhabitualsnorers.RegulPept.1997;71:29---36.
2.FribergD,AnsvedT,BorgK,Carlsson-NordlanderB,LarssonH, SvanborgE.Histologicalindicationsofprogressivesnorers dis-easeinanupperairwaymuscle.AmJRespirCritCareMed. 1998;157:586---93.
3.KimoffRJ,SforzaE,ChampagneV,OfiaraL,GendronD.Upper airwaysensationinsnoringandobstructivesleepapnea.AmJ RespirCritCareMed.2001;164:250---5.
4.SchaferJ.Howcanonerecognizeavelumsnorer. Laryngorhi-nootologie.1989;68:290---4.
5.Takeuchi T, Futatsuka M, Imanishi H, Yamada S. Pathologi-cal changes observed in the finger biopsy of patients with vibration-inducedwhitefinger.Scand JWorkEnvironHealth. 1986;12:280---3.
6.PlowmanL,LauffDC,Berthon-JonesM,SullivanCE.Wakingand genioglossusmuscleresponsestoupperairwaypressure oscil-lationinsleepingdogs.JApplPhysiol.1990;68:2564---73.
7.TeramotoS,SudoE,MatsuseT,OhgaE,IshiiT,OuchiY,etal. Impairedswallowing reflexinpatientswithobstructivesleep apneasyndrome.Chest.1999;116:17---21.
8.JobinV,ChampagneV,BeauregardJ, CharbonneauI, McFar-land DH, Kimoff RJ. Swallowing function and upper airway sensationinobstructivesleepapnea.JApplPhysiol.2007;102: 1587---94.
9.Jäghagen EL, Berggren D, Isberg A. Swallowing dysfunction relatedtosnoring:avideoradiographicstudy.ActaOtolaryngol. 2000;120:438---43.
10.JäghagenEL,FranklinKA,IsbergA.Snoring,sleepapnoeaand swallowingdysfunction:avideoradiographicstudy. Dentomax-illofacialRadiol.2003;32:311---6.
11.BroussardDL,AltschulerSM.Centralintegrationofswallowand airway-protectivereflexes.AmJMed.2000;108:62S---7S.
12.ErtekinC,AydogduI.Neurophysiologyofswallowing.Clin Neu-rophysiol.2003;114:2226---44.
13.Jäghagen EL, Berggren D, Dahlqvist A, Isberg A. Pre-diction and risk of dysphagia after uvulopalatopharyngo-plasty and uvulopalatoplasty. Acta Otolaryngol. 2004;124: 1197---203.
14.ValbuzaJS,deOliveiraMM,ZancanellaE,ContiCF,PradoLBF, CarvalhoLBC,etal.Swallowingdysfunctionrelatedto obstruc-tivesleepapnea:anasalfibroscopypilotstudy.SleepBreath. 2011;15:209---13.
15.Kelly JH.Use ofmanometry in theevaluation ofdysphagia. OtolaryngolHeadNeckSurg.1997;116:355---7.
16.KomiyamaS,YamashitaH,Miyazaki H,MasudaT. Pharyngoe-sophagealpressureinpatientswithswallowingdisorders.Eur ArchOtorhinolaryngol.1994;251:100---3.
17.KahrilasPJ,LogemannJA,LinS,ErgunA.Pharyngealclearance during swallowing:a combined manometric and videofluoro-scopicstudy.Gastroenterology.1992;103:128---36.
18.Dantas DAS, Mauad T, Silva LFF, Lorenzi-Filho G, Formigoni GGS, CahaliMB.Theextracellularmatrixofthelateral pha-ryngeal wall in obstructive sleep apnea. Sleep. 2012;35: 483---90.
19.Cahali MB. Lateral pharyngoplasty: a new treatment for obstructive sleep apnea hypopnea syndrome. Laryngoscope. 2003;113:1961---8.
20.CahaliMB,SoaresCFP,DantasDAS,FormigoniGGS.Tonsil vol-ume, tonsil grade and obstructivesleep apnea:is thereany meaningfulcorrelation?Clinics.2011;66:1347---51.
21.Langmore S, Schatz K, Olson N. Fiberopticendoscopic eval-uation of swallowing safety: a new procedure. Dysphagia. 1988;2:216---9.
22.CastellDO,RichterJE,DaltonCB.Esophagealmotilitytesting. NewYork:ElsevierSciencePublishingCo.,Inc.;1987.
23.Richter JE, Wu WC, Johns DN, Blackwell JN, Nelson JL 3rd, CastellJA, et al. Esophageal manometry in 95healthy adult volunteers. Variability of pressures with age and fre-quency of ‘‘abnormal’’ contractions. Dig Dis Sci. 1987;32: 583---92.
25.Dodds WJ, Logemann JA, Stewart ET.Radiologic assessment ofabnormaloraland pharyngealphasesofswallowing.AmJ Roentgenol.1990;154:965---74[Reviewarticle].
26.ButlerSG,StuartA,KempS.Flexibleendoscopicevaluationof swallowinginhealthyyoungandolderadults.AnnOtolRhinol Laryngol.2009;118:99---106.
27.Butler SG, Stuart A, Markley L, Rees C. Penetration and aspiration in healthy older adults as assessed during endo-scopic evaluation of swallowing. Ann Otol Rhinol Laryngol. 2009;118:190---8.
28.FribergD.Heavysnorer’sdisease:aprogressivelocal neurop-athy.ActaOtolaryngol.1999;119:925---33.
29.Baijens LWJ, Speyer R. Effects of therapy for dyspha-gia in Parkinson’s disease systematic review. Dysphagia. 2009;24:91---102.
30.NagayaM,KachiT,YamadaT.Effectofswallowingtrainingon swallowing disorders in Parkinson’s disease. Scand J Rehabil Med.2000;32:11---5.
31.BuchholzDW,BosmaJF,DonnerMW.Adaptation,compensation and decompensationof thepharyngealswallow.Gastrointest Radiol.1985;10:235---9.
32.Okada S,Ouchi Y,TeramotoS. Nasalcontinuouspositive air-way pressure and weight loss improve swallowing reflex in patientswithobstructivesleepapneasyndrome.Respiration. 2000;67:464---6.
33.Takasaki K, Umeki H, Enatsu K. Investigation of pharyngeal swallowingfunctionusinghigh-resolutionmanometry. Laryngo-scope.2008;118:1729---32.
34.MezzanotteWS,TangelDJ,WhiteDP.Wakinggenioglossal elec-tromyogram in sleep apnea patients versus normal controls (a neuromuscular compensatory mechanism). J Clin Invest. 1992;89:1571---9.
35.OdaAL,ChiappettaALML,AnnesM,MarchesanIQ,OliveiraASB. Clinical, endoscopical and manometrical evaluation of swal-lowinginpatientswithmyastheniagravis.ArqNeuropsiquiatr. 2002;60:986---95.
36.LeeTH,LeeJS,KimWJ.Highresolutionimpedancemanometric findingsindysphagiaofHuntington’sdisease.WorldJ Gastroen-terol.2012;18:1695---9.
37.Mello M, Gyawali CP. Esophageal manometry in gastro-esophageal reflux disease. Gastroenterol Clin North Am. 2014;43:69---87.
38.KarkosPD,LeongSC,BentonJ,SastryA,AssimakopoulosDA, IssingWJ.Refluxandsleepingdisorders:asystematicreview.J LaryngolOtol.2009;123:372---4.