REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
Substance
misuse
and
sexual
function
in
adolescents
with
chronic
diseases
Priscila
Araújo
a,
Márcio
Guilherme
Nunes
Carvalho
b,
Marlon
van
Weelden
c,
Benito
Lourenc
¸o
b,
Lígia
Bruni
Queiroz
b,
Clovis
Artur
Silva
b,∗aUniversidadeCatólicadeCampinas,Campinas,SP,Brazil
bFaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil cMedicalFaculty,Amsterdam,Netherlands
Received29July2015;accepted8October2015
Availableonline3January2016
KEYWORDS
Alcoholism; Tobacco; Illicitdrugs; Bullying; Adolescent; Chronicdisease
Abstract
Objective: Toevaluatealcohol/tobaccoand/orillicitdrugmisuseinChronicDiseases(CDs). Methods: A cross-sectionalstudy with220CDsadolescentsand110 healthycontrols includ-ing:demographic/anthropometric data; pubertymarkers; modifiedquestionnaireevaluating sexualfunction,alcohol/smoking/illicitdrugmisuseandbullying;andthephysician-conducted CRAFFT(car/relax/alone/forget/friends/trouble)screentoolforsubstanceabuse/dependence highrisk.
Results: Thefrequenciesofalcohol/tobaccoand/orillicitdruguseweresimilarinbothgroups (30%vs.34%,p=0.529),likewisethefrequenciesofbullying(42%vs.41%,p=0.905).Further analysissolelyinCDspatientsthatusedalcohol/tobacco/illicitdrugversusthosethatdidnot use showed thatthe median current age [15 (11---18)vs. 14 (10---18) years,p<0.0001] and education years[9 (5---14)vs.8(3---12)years,p<0.0001]weresignificanthigherinsubstance use group. The frequencies of Tanner 5(p<0.0001), menarche (p<0.0001)and spermarche (p=0.001)werealsosignificantlyhigherinpatientswithCDsthatusedalcohol/tobacco/illicit, likewisesexualactivity(23%vs.3%,p<0.0001).A trendofalowfrequencyofdrug therapy wasobservedinpatientsthatusedsubstances(70%vs.82%,p=0.051).A positivecorrelation wasobservedbetweenCRAFFTscoreandcurrentageinCDpatients(p=0.005,r=+0.189)and controls(p=0.018,r=+0.226).
Conclusions: AlateragewasevidencedinCDspatientsthatreportedlicit/ilicitdrugmisuse.In CDsadolescent,substanceusewasmorelikelytohavesexualintercourse.Ourstudyreinforces thatthesepatientsshouldbesystematicallyscreenedbypediatriciansfordrugrelatedhealth behavioralpatterns.
©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](C.A.Silva).
http://dx.doi.org/10.1016/j.rppede.2015.10.008
PALAVRAS-CHAVE
Alcoolismo; Tabaco; Drogasilícitas; Assédiomoral; Adolescente; Doenc¸acrônica
Usoindevidodedrogasefunc¸ãosexualemadolescentescomdoenc¸ascrônicas
Resumo
Objetivo: Avaliarousoindevidodeálcool/tabacoe/oudedrogasilícitasemDoenc¸asCrônicas (DCs).
Métodos: Estudo transversal com 220 adolescentes com DCs e 110 controles saudáveis, incluindo:dadosdemográficos/antropométricos;marcadoresdepuberdade;questionário modi-ficadodeavaliac¸ãodafunc¸ãosexual,abusodeálcool/tabagismo/drogasilícitaseassédiomoral; eousodoinstrumentoCRAFFT(car/relax/alone/forget/friends/trouble)pelomedicoparao abuso/dependênciadesubstânciasdealtorisco.
Resultados: Asfrequências deuso deálcool/tabaco e/oudrogas ilícitasforamsemelhantes emambososgrupos(30%vs.34%,p=0,529),assimcomoasfrequênciasdeassédiomoral(42% vs.41%,p=0,905).Umaanálisemaisaprofundadaapenasem pacientescomDCsqueusaram álcool/tabaco/drogailícitaversusaquelesquenãousarammostrouqueaidademedianaatual [15(11-18)vs.14(10-18)anos,p<0,0001]eanosdeescolaridade[9(5-14)vs.8(3-12)anos, p<0,0001]foramsignificativamente maioresnogrupoquefaziausodassubstâncias. As fre-quênciasdeTanner5(p<0,0001),menarca(p<0,0001)eespermarca(p=0,001)tambémforam significativamentemaioresempacientescomDCsqueusaram álcool/tabaco/drogasilícitas, assimcomo aatividade sexual(23%vs.3%, p<0,0001). A tendênciade baixa frequênciade terapiacommedicamentosfoiobservadaempacientesqueusaramsubstâncias(70%vs.82%, p=0,051).Observou-se uma correlac¸ão positiva entre oscore no CRAFFT e idade atual em pacientescomDCs(p=0,005,r=+0,189)econtroles(p=0,018,r=+0,226).
Conclusões: Aidademaisavanc¸adafoidemonstradaempacientescomDCsquerelataramuso indevido dedrogas lícitas/ilícitas.Em adolescente comDCs, ousodassubstâncias resultou emmaiorpropensãoàpráticaderelac¸õessexuais.Nossoestudoreforc¸aqueessespacientes devemsersistematicamenteavaliadospelospediatrasemrelac¸ãoapadrõesdecomportamento desaúderelacionadoscomdrogas.
©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Adolescenceisadevelopmentalstagecharacterizedby bio-logicalandsocialchanges.1,2Riskpatternsmaybegininthis
periodoflife,includingsubstancemisuse(alcohol,tobacco andillicit drugs)1 andhigh-risk sexualbehaviors.3 Harmful
phenomenaofpeervictimization,suchasbullying,isalsoa relevantprobleminhealthyadolescents4andinthosewith
chronicdiseases(CDs).5
Of note, the prevalence of chronic conditions has increasedinpediatricpopulation,6and10%ofadolescents
sufferfromCDs.7However,toourknowledge,misuseof
sub-stancesevaluatedbyascreeningtool,8aswellasassessment
of bullying and sexual function, have not been simulta-neouslystudiedinanadolescentCDspopulation.
Therefore, the objectives of the present study were toevaluate alcohol, tobacco and/or illicit drug misusein adolescentCDspatientsandhealthycontrols.Thepossible associationsbetweenthesubstancemisuseinCDspatients accordingtosexual function,bullying, demographicdata, pubertymarkers,CDsgroupsanddrugtherapyusewerealso assessed.
Method
FromFebruary toDecember 2014,a cross-sectional study wascarriedoutinvolving220consecutiveoutpatient adoles-cents(current age10---19yearsaccordingto WorldHealth
Organizationcriteria)withpediatricCDs.Allofthemwere followed at the Adolescent Unit of our University Hospi-talandnoneofthemhadunwillingnesstoparticipate.The controlgroupincluded110 healthyadolescents(rate2:1), withoutCDs,consecutivelyadmittedtotheoutpatientclinic andreferred fromprimaryandsecondary healthcare ser-vices to the Adolescent Unit of our University Hospital. ThisstudywasapprovedbytheLocalEthicsCommitteeof Hospital. All adolescents and their parents signed a con-sent/assentterm.
This study included a modified questionnaire evaluat-ing sexual function,9 alcohol/tobacco/illicit drug use and
bullying was applied.The Portuguese CRAFFT (mnemonic acronym of car, relax, alone,forget, friendsand trouble) screen (CRAFFT/CEASER) version was performed in both groups.3,8 Demographic/anthropometric data and puberty
markersassessmentswerealsoevaluated.
Apilotstudy wascarriedoutin30 consecutivehealthy and adolescents withCDs, whowere tested and retested 1---2 months. The pre-test evaluated the subject compre-hensionofthequestions,theconsistencyandcoherenceof theanswersandthetimetakentoanswerthequestionnaire. Themodifiedquestionnaireincluded14questionswiththe optionofanswer ‘‘yes/no’’or age/numberoftimesabout sexualfunction,9bullyingandalcohol/tobacco/illicitdrugs
use.Sexualfunctionassessmentincluded9:ageatfirst
of sexual activity by parents and total number of sexual partners. Alcohol/tobaccoanddrugs [illicit inhalantsdrug (gluesniffing,aerosol andsolvents)andillicitdrugs [mari-juana,stimulants(cocaine,crackandspeed),poppers,LSD, opiates, heroin, crystal meth and ecstasy] use were also assessed:ageatalcoholinitiation,numberofdaysofalcohol useinthelast30days,ageatsmokinginitiation,numberof dayssmokingcigarettesinthelast30days,ageatillicitdrug initiationandnumberofdaysusingillicitdrugs inthelast 30days.Bullying,whichisdefinedasarecurrentexposure toemotionaland/orphysicalaggression,wasobtainedbya ‘‘yes/no’’answertothequestion(‘‘Haveyoueversuffered bullying?’’).Thequestionnairewasstrictlyconfidentialand wasperformedintheabsenceoflegalguardians,relatives andfriends.
The Portuguese versionof physician-conducted CRAFFT (CRAFFT/CEASER)screenwasusedandconsistedof9 ques-tionsdevelopedtoscreenadolescentsforhigh-riskalcohol anddrugmisuse.8Thisquestionnaireisdividedintwoparts.
PartAincludesthreequestionsregardingtheuseofalcohol, marijuana/hashishoranothersubstanceinthelasttwelve months.Iftheadolescentresponded‘‘no’’toallthree ques-tions, only the question related to ‘‘car’’ of the B---part shouldbeasked.Iftheadolescentanswered‘‘yes’’tooneof theopeningquestions,allofthequestionsofpartBshould be asked.B-part containedsix questions,which are signs ofproblematicsubstanceuse.Onepointwasgiventoeach ‘‘yes’’answerintheB-partofthequestionnaire.Thescore rangedfrom0to6.Atotalscoreof≥2indicatedhighrisk forsubstanceabuse/dependenceandaneedforadditional assessment.3,8
Regarding socio-demographicandanthropometricdata, currentage,gender,yearsofeducation,weightandheight wereevaluated.Bodymassindex(BMI)wasdefinedbythe formula:weightinkilograms/heightinsquaremeters.The Braziliansocio-economicstatuswereclassifiedaccordingto theABEP(Associac¸a˜oBrasileiradeEmpresasdePesquisa).10
Secondarysexualcharacteristicswereclassified accord-ingtoTannerpubertalchanges.11Ageatfirstmenstruation
(menarche)andageatfirstejaculation(spermarche)were registeredbasedonmemoryrecollection.
Chronic diseases, with disease duration more than three months, were classified in: Allergic/Immunologic, Cardiopulmonary, Dermatologic, Endocrinologic, Gas-troenterologic, Hematologic, Neuropsychiatric, Renal and Rheumatic conditions. The use of drug therapy was also assessed.
The test---retest reliability of the modified question-nairewasverifiedfor CDspopulationandhealthycontrols using the Kappa index. Results were presented as the mean±standarddeviation(SD)or median(range)for con-tinuous and number (%) for categorical variables. Data were compared by t or Mann---Whitney tests in continu-ousvariablestoevaluatedifferencesbetweenadolescents with CDs and controls, and between subgroups. For cat-egorical variables, differences were assessed by Fisher’s exactor Pearsonchi-squaretests.Spearmanrank correla-tioncoefficient wasusedforcorrelationsbetweenCRAFFT score and age. The level of significance was set at 5% (p<0.05).
Results
Thekappaindexfortest---retestwas0.850,demonstrating excellentreliabilityfortheadolescents’responses.
The frequencies of alcohol, tobaccoand/or illicit drug useweresimilarinbothadolescentswithCDsandhealthy controls(30% vs.34%,p=0.529).The frequencyof alcohol
consumption in the past 30 days was significantly lower in adolescents with CDs compared with controls (6% vs. 27%,p=0.005).IllicitdrugswereusedbythreeCDspatients
(marijuana, cocaine and/or poppers) and three controls (marijuana)(p=0.404). Nodifferencewasobserved inthe
frequencyofsmoking(p=0.114).CRAFFTscore≥2was simi-larin bothgroups (4% vs.5%,p=0.575).The frequency of
bullying was alike in both groups (36% vs. 39%, p=0.905)
(Table 1).The median of age onsetsmokingwas14years (11---15)inadolescentswithCDsandwas14years(7---15)in healthycontrols.Themedianofageonsetilicitdrugusewas 14.5years(14---15)inadolescentswithCDsandwas14years inhealthycontrols.
A positive correlation was evidenced between CRAFFT scoreandcurrentage inCDspatients(p=0.005,r=+0.189)
andhealthycontrols(p=0.018,r=+0.226),likewisebetween
CRAFFT score and education years in CDs (p=0.015,
r=+0.164) and controls (p=0.039, r=+0.197). A positive
correlation was observed between CRAFFT score and age of alcohol onset in CDs patients (p=0.021, r=+0.286)
(Table1).
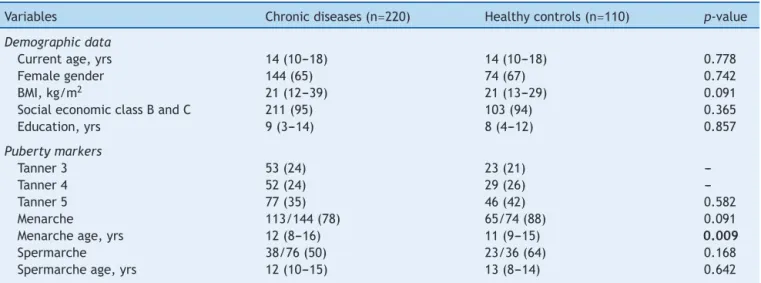
Themediancurrentagewassimilarbetweenadolescent withCDsand healthy controls [14 (10---18) vs. 14 (10---18) years,p=0.778], likewisethe frequencyof female gender
(65%vs.67%,p=0.742),yearsofeducation[9(3---14)vs.8
(4---12)years,p=0.857],Braziliansocio-economicclasses B
orC (95%vs.94%, p=0.365)and betweenTanner 3,4and
5 (p=0.582). The median menarche age was significantly
higherintheformergroup[12(8---16) vs.11(9---15) years,
p=0.009].Nodifferencewasevidencedintheageat
sper-marcheinbothgroups(p=0.642)(Table2).
Further analysis solely of patients with CDs regarding alcohol/tobacco/illicitdrugmisuseshowedthatthemedian currentage[15(11---18)vs.14(10---18)years,p<0.0001]and
educationyears[9(5---14)vs.8(3---12)years,p<0.0001]were
significanthigherinthosethatusedtheaforementioned sub-stances.ThefrequenciesofTanner5(p<0.0001),menarche
(p<0.0001)andspermarche(p=0.001)werealsosignificantly
higherintheformergroup,likewisesexualactivity(23%vs. 3%,p<0.0001)(Table3).
Of our 9 patients with CDs with CRAFFT score ≥2, rheumatic diseases were found in 8 (juvenile idiopathic arthritis in three patients, juvenile dermatomyositis in one,childhood-onsetsystemiclupuserythematosusinone, Sjögren syndrome in one, Takayasu arteritis in one and Henoch---Schönlein purpura in one)and Allergicdisease in onepatient(asthma).
The frequencies of chronic conditions in patients that usedalcohol/tobacco/illicitdrugversusthosethatdidnot use weresimilar (p>0.05). A trend of a low frequency of drugtherapywasevidencedinpatientsthatusedsubstances comparedtothosethatdidnotused(70%vs.82%,p=0.051)
Table1 Alcohol,smokingandillicitdruguse,andbullyinginadolescentswithchronicdiseasesandhealthycontrols. Variables Chronicdiseases(n=220) Healthycontrols(n=110) p-value
Alcohol,smokingand/orillicitdruguse 66(30) 37(34) 0.529
Alcoholuse 66(30) 37(34) 0.529
Ageatonsetalcohol,yrs 14(6---17) 14(7---18) 0.935
Drinkingalcoholinpast30days 4/66(6) 10/37(27) 0.005
Smokinguse 5(2) 7(6) 0.114
Illicitdruguse 3(1) 3(3) 0.404
CRAFFTscoreinthelast12months(0---6) 0(0---5) 0(0---5) 0.712
CRAFFTscore≥2 9(4) 6(5) 0.575
CRAFFTitem
Car 41(19) 17(15) 0.474
Relax 6/36(17) 5/27(19) 1.000
Alone 1/36(3) 2/27(7) 0.572
Forget 1/36(3) 4/27(15) 0.155
Familiy/friends 8/36(22) 7/27(26) 0.733
Trouble 6/36(17) 0/27(0) 0.033
Bullying 80(36) 43(39) 0.905
Sexualfunction
Sexualactivity 20(9) 16/109(15) 0.126
Firstsexualactivityage,yrs 15(8---16) 14(10---17) 0.859
Sexualintercourseinlastmonth 3/20(15) 6/16(38) 0.146
Condomatthefirstsexualactivity 19/20(95) 13/16(81) 0.303
NOralcontraceptionuseinfemales 2/13(15) 3/13(23) 1.000
Emergencycontraceptiveusea 1/13(8) 6/13(46) 0.073
Knowledgeofsexualactivitybyparents 9/20(45) 11/16(69) 0.154
Totalnumberofsexualpartner,number 1(1---16) 1(1---5) 0.586
Theresultsarepresentedinn(%)andmedian(range),CRAFFT(car,relax,alone,forget,friends,trouble)screeningtest;BMI,bodymass index.
aOnehealthycontrolusedoralcontraceptionbeforesexualactivity.
Table2 Demographicdataandpubertymarkersinadolescentswithchronicdiseasesandhealthycontrols.
Variables Chronicdiseases(n=220) Healthycontrols(n=110) p-value
Demographicdata
Currentage,yrs 14(10---18) 14(10---18) 0.778
Femalegender 144(65) 74(67) 0.742
BMI,kg/m2 21(12---39) 21(13---29) 0.091
SocialeconomicclassBandC 211(95) 103(94) 0.365
Education,yrs 9(3---14) 8(4---12) 0.857
Pubertymarkers
Tanner3 53(24) 23(21)
---Tanner4 52(24) 29(26)
---Tanner5 77(35) 46(42) 0.582
Menarche 113/144(78) 65/74(88) 0.091
Menarcheage,yrs 12(8---16) 11(9---15) 0.009
Spermarche 38/76(50) 23/36(64) 0.168
Spermarcheage,yrs 12(10---15) 13(8---14) 0.642
Theresultsarepresentedinn(%)andmedian(range);BMI,bodymassindex.
Discussion
Our study evaluated simultaneously adolescent’s health problems in CDspatients and healthy controls. In adoles-centswithCDs,substanceusewasobservedinlaterageand wasmorelikelytosexualintercoursecomparedtothosethat didnotuselicit/illicitdrug.
The advantage of this study was the assessment of physician-conducted CRAFFT (CEASER) screening tool for substance misuse in adolescents.3,8 The use of the
Table3 Demographicdata,pubertymarkersandbullyinginadolescentswithchronicdiseasesaccordingtoalcohol,smoking andillicitdruguse.
Variables Usealcohol,
smokingand/or illicitdrug(n=66)
Nonusealcohol, smokingand/or illicitdrug(n=154)
p-value
Demographicdata
Currentage,yrs 15(11---18) 14(10---18) <0.0001
Femalegender 43(65) 101(66) 0.951
BMI,kg/m2 21(17---38) 21(12---39) 0.275
SocialeconomicclassBandC 62(94) 149(97) 0.457
Education,yrs 9(5---14) 8(3---12) <0.0001
Pubertymarkers
Tanner3 13(20) 40(26)
---Tanner4 15(23) 37(24)
---Tanner5 36(55) 41(27) <0.0001
Menarche 42/43(98) 71/101(70) <0.0001
Menarcheage,yrs 12(9---16) 12(8---15) 0.348
Spermarche 18/23(78) 20/53(38) 0.001
Spermarcheage,yrs 12(10---14) 12.50(10---15) 0.668
Sexualfunction
Sexualactivity 15(23) 5(3) <0.0001
Firstsexualactivityage,yrs 14.50(8---16) 15(14---15) 0.702
Sexualintercourseinlastmonth 3/15(20) 0/5(0) 0.539
Condomatthefirstsexualactivity 14/15(93) 5/5(100) 1.000
NOralcontraceptionuseinfemales 2/11(18) 0/2(0) 1.000
Emergencycontraceptiveuse 1/11(9) 0/2(0) 1.000
Knowledgeofsexualactivitybyparents 6/15(40) 3/5(60) 0.617
Totalnumberofsexualpartner,number 1(1---6) 1(1---16) 1.000
Bullying 24(36) 55(36) 0.685
Theresultsarepresentedinn(%)andmedian(range);CRAFFT(car,relax,alone,forget,friends,trouble)screeningtest;BMI,bodymass index.
Table4 Adolescentchronicdiseasesanddrugtherapyaccordingtoalcohol,smokingandillicitdrugusetheresultsarepresented inn(%).
Variables Usealcohol,
smokingand/or illicitdrug(n=66)
Nonusealcohol, smokingand/or illicitdrug(n=154)
p-value
Adolescentchronicdiseases
Immunologic 3(5) 2(1) 0.160
Dermatologic 3(5) 3(2) 0.367
Endocrinologic 12(18) 33(21) 0.715
Gastroenterologic 2(3) 11(7) 0.352
Neuropsychiatric 7(11) 20(13) 0.822
Allergic/cardiopulmonary 9(14) 23(15) 1.000
Renal 5(8) 5(3) 0.170
Rheumatic 46(70) 112(73) 0.743
Hematologic 0(0) 1(1) 1.000
Drugtherapyforchronicdiseases 46(70) 126(82) 0.051
observed in our study, since these data were previously relatedwithbullyingandsubstancemisuse.1,3,12,13
Alcoholintakewasreportedbyapproximatelyonethird of our CDs patients, even though a low intakefrequency in the last month. The prevalence of alcohol use in ado-lescentsvariesfrom7.8%to78.9%12,14,15 aroundtheworld
and from 26% to 71% in Brazil.16---21 There are studies in
adolescentswithspecificCDs,generallywithsmallsamples and variablefrequencies of alcohol use (4.8%---70%), such asjuvenileidiopathicarthritis,22obesityandoverweight,23
asthma,24 cystic fibrosis and sickle cell disease.25 This
Importantlyin the evaluation of only adolescents with CDs,we observed that use of alcohol, tobacco and illicit drugsoccurredin CDspatientsthat presentedhigherage, higher education background and post pubertal markers. Theavoidanceofsubstanceuseinearlyadolescencemaybe relatedtooverprotectionofparentsandprimarycaregivers. Incontrast,amoreliberalparentalattitudemaycontribute toanincreaseinsubstancemisuselateroninlife.Moreover, severeCDsthatrequiredhigherfrequenciesofmedication mayhavecontributedtothelowuseofillicitandlicitdrugs. The adolescents may develop a drinking pattern that is socially acceptable and a small group of CDs patients’ misused alcohol more frequently. We applied a screening procedureforsubstancemisuseand4%ofourCDspatients hadahigherriskforsubstanceabuse/dependence.A posi-tivecorrelationwasalsoevidencedbetweenCRAFFTscore andcurrent age, indicating a higherrisk for harmful sub-stancemisuseinolderCDsadolescents.
Smokingwasreportedonlyby2%ofourCDspatients.This aspecthasalsobeenobservedinadolescentsofour conti-nentalcountryduetobanonsmokingadvertising,26useof
warningsoncigarettespackages27andprohibitioninpublic
places.28 The use of any illicit drug (marijuana, solvents,
cocaineorcrack)wasreportedin2.8%ofadolescentsina Braziliansurvey,21andthisresultwashigherthaninourCDs
patients.
Interestingly,CDssubstanceusersengagedmoreinsexual activity,andmaypresentahigherriskforsexually transmit-ted diseases, unwanted pregnancy and low contraceptive use.29,30Thisfindingmayalsoberelatedtothefactthatthe
patientswereolderandprobablyhadhighersexualmaturity. However,thisstudydidnotevaluateifdrinkinginfluenced high-risksexualbehaviorinCDspatients.
In addition, bullying was frequently reported in CDs and seems not to be linked to substance use. Ado-lescents with CDs may suffer from this victimization,4,5
mayinduceanxiety-depressivedisorderandinterferewith properadherence to medication use. Aprospective study evaluatingprevalence and intensity of bullying in a large sampleofCDspatientswillberequired.
Themainlimitationofthepresentstudywastheuseof aconveniencesampleforCDspatientsinatertiary Univer-sityHospital,predominantlyofrheumatic,endocrinologic, allergicandcardiopulmonarydiseases.Asmallsamplemay alsohavereducedourpowertodetectdifferencesbetween thetwogroupsandthecrosssectionaldesignnatureofour studydidnotallowtheevaluationoftemporalitybetween exposureandoutcome.Wedidnotevaluatediseaseactivity criteriaforallCDs,andindeedthisfindingmaymodifythe behavior.Moreover, thehealthy controlsand CDspatients werereferredtotheadolescentclinicofourUniversity Hos-pitaltoguidanceabout sexualfunctionand birthcontrol, emotionalproblemsanddrugsissues.
Aneedforadditionalassessmentandtherapeutic inter-ventionwithamultidisciplinaryandmultiprofessionalteam is required for CDs adolescents and families at risk for substance misuse. Confidential discussion of illicit and licitdrugsand other potentially riskybehaviorsshouldbe includedintheroutinecareofclinicsthatfollowed-upCDs patients.
Inconclusion,alateragewasevidencedinCDspatients thatreportedlicit/ilicitdruguse.CDssubstanceuserswere
morelikelytohavesexualintercourse.Ourstudyreinforces that these patients should be systematically screened by pediatricians for sexual, alcohol and drug related health behavioralpatterns.
Funding
This study was supported by grants from Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo (FAPESP 2009/51897-5, 2011/12471-2 and 2014/14806-0 to CAS), Conselho Nacional de Desenvolvimento Científico e Tec-nológico(CNPQ302724/2011-7toCAS),FedericoFoundation (toCAS),andNúcleodeApoioàPesquisa‘‘SaúdedaCrianc¸a edoAdolescente’’daUSP(NAP-CriAd)toCAS.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
We thank Dr. JR Knight and Dr. P Schram for supplying the Portugueseversion ofCRAFFT screen(CEASER) instru-ment,BostonChildren’sHospital,Mass,USA.Ourgratitude toUlyssesDoria---Filhoforthestatisticalanalysis.
References
1.SawyerSM,AfifiRA,BearingerLH,BlakemoreSJ,DickB,Ezeh AC,etal.Adolescence:afoundationforfuturehealth.Lancet. 2012;379:1630---40.
2.JanniniSN,Dória-FilhoU,DamianiD,SilvaCA.Musculoskeletal paininobeseadolescents.JPediatr(RioJ).2011;87:329---35. 3.LevyS,SherrittL,GabrielliJ,ShrierLA,KnightJRJr.Screening
adolescentsforsubstanceuse---relatedhigh-risksexual behav-iors.JAdolescHealth.2009;45:473---7.
4.SentenacM,GavinA,ArnaudC,MolchoM,GodeauE,Nic Gab-hainnS.Victimsofbullyingamongstudentswithadisabilityor chronicillnessandtheirpeers:across-nationalstudybetween IrelandandFrance.JAdolescHealth.2011;48:461---6. 5.PittetI,BerchtoldA,AkréC,MichaudPA,SurísJC.Are
adoles-centswithchronicconditionsparticularlyatriskforbullying? ArchDisChild.2010;95:711---6.
6.NgM,FlemingT,RobinsonM,ThomsonB,GraetzN,Margono C,et al. Global, regional, and nationalprevalence of over-weightand obesityin childrenandadultsduring1980---2013: asystematicanalysisfor theGlobalBurdenofDiseaseStudy 2013.Lancet.2014;384:766---81.
7.SurisJC,MichaudPA,VinerR. Theadolescentwithachronic condition. Part I: Developmental issues. Arch Dis Child. 2004;89:938---42.
8.Knight JR, Schram P. Portuguese version of CRAFFT screen (CEASER). Available from: http://www.ceasar-boston.org/ CRAFFT/pdf/CRAFFTPortuguese.pdf[cited19.01.15]. 9.FebronioMV,PereiraRM,BonfaE,TakiutiAD,PereyraEA,Silva
CA.Inflammatorycervicovaginalcytologyisassociatedwith dis-easeactivityinjuvenilesystemiclupuserythematosus.Lupus. 2007;16:430---5.
10.ABEP [homepage on the Internet]. São Paulo: Associac¸ão BrasileiradeEmpresasdePesquisas[cited19.01.15].Available from:www.abep.org.br.
12.AtilolaO,StevanovicD,BalharaYP,AvicennaM,KandemirH, KnezR,etal.Roleofpersonalandfamilyfactorsinalcoholand substanceuseamongadolescents:aninternationalstudywith focusondevelopingcountries.JPsychiatrMentHealth Nurs. 2014;21:609---17.
13.MoreiraTC,BelmonteEL,VieiraFR,NotoAR,FerigoloM,Barros HM.Communityviolenceandalcoholabuseamongadolescents: asexcomparison.JPediatr(RioJ).2008;84:244---50.
14.Seil KS, Desai MM, Smith MV. Sexual orientation, adult con-nectedness,substanceuse,andmentalhealthoutcomesamong adolescents:findingsfromthe2009NewYorkCityYouthRisk BehaviorSurvey.AmJPublicHealth.2014;104:1950---6. 15.PoelenEA,ScholteRH,EngelsRC,BoomsmaDI,WillemsenG.
Prevalenceandtrendsofalcoholuseandmisuseamong adoles-centsandyoungadultsintheNetherlandsfrom1993to2000. DrugAlcoholDepend.2005;79:413---21.
16.MaltaDC,MachadoIE,PortoDL,daSilvaMM,deFreitasPC,da CostaAW,etal.AlcoholconsumptionamongBrazilian Adoles-centsaccordingtotheNationalAdolescentSchool-basedHealth Survey(PeNSE2012).RevBrasEpidemiol.2014;17:203---14. 17.MaltaDC,BernalRT.Comparisonofriskandprotectivefactors
forchronicdiseasesinthepopulationwithandwithouthealth insuranceintheBraziliancapitals,2011. RevBrasEpidemiol. 2014;17:241---55.
18.BarbosaFilhoVC,CamposW,LopesAdaS.Prevalenceof alco-holandtobaccouseamongBrazilianadolescents:asystematic review.RevSaudePublica.2012;46:901---17.
19.DuailibiLB,RibeiroM,LaranjeiraR.Profileofcocaineandcrack usersinBrazil.CadSaudePublica.2008;24:s545---57.
20.MaltaDC,MascarenhasMD,PortoDL,DuarteEA,SardinhaLM, BarretoSM,et al. Prevalence of alcoholand drug consump-tionamongadolescents:dataanalysisoftheNationalSurvey ofSchoolHealth.RevBrasEpidemiol.2011;14Suppl.1:136---46.
21.MadrugaCS,LaranjeiraR,CaetanoR,PinskyI,ZaleskiM,Ferri CP.UseoflicitandillicitsubstancesamongadolescentsinBrazil ---anationalsurvey.AddictBehav.2012;37:1171---5.
22.NashAA,BrittoMT,LovellDJ,PassoMH,RosenthalSL.Substance use among adolescents with juvenile rheumatoid arthritis. ArthritisCareRes.1998;11:391---6.
23.TerresNG,PinheiroRT,HortaBL,PinheiroKA,HortaLL. Preva-lence and factors associated to overweight and obesity in adolescents.RevSaudePublica.2006;40:627---33.
24.KimO,KimBH.Associationofasthmasymptomswithcigarette smokingandalcoholconsumptioninKoreanadolescents.Nurs HealthSci.2013;15:65---72.
25.Britto MT, Garrett JM, Dugliss MA, Daeschner CW Jr, John-sonCA,LeighMW,et al.Riskybehavior inteens withcystic fibrosisorsicklecelldisease:amulticenterstudy.Pediatrics. 1998;101:250---6.
26.Galduróz JC, Fonseca AM, Noto AR, Carlini EA. Decrease in tobacco use among Brazilian students: a possible conse-quence of the ban on cigarette advertising? Addict Behav. 2007;32:1309---13.
27.NascimentoBE,OliveiraL,VieiraAS,JoffilyM,GleiserS,Pereira MG,etal.Avoidanceofsmoking:theimpactofwarninglabels inBrazil.TobControl.2008;17:405---9.
28.SilvaST,MartinsMC,FariaFR,CottaRM.Combatingsmoking inBrazil:thestrategicimportanceofgovernmentactions.Cien SaudeColet.2014;19:539---52.
29.Araujo DB, Borba EF, Abdo CH, Souza Lde A, Goldenstein-SchainbergC,ChahadeWH,etal.Sexualfunctioninrheumatic diseases.ActaReumatolPort.2010;35:16---23.