1Serviço de Endocrinologia e M et abologia do Hospit al de Clínicas da Universidade Federal do Paraná (UFPR) Curit iba PR, Brasil; 2Depart ment s of M edicine and Pharmacology, College of Physicians & Surgeons, Columbia Universit y, New York, NY, USA; 3Serviço de Neurologia do Hospit al de Clínicas da UFPR.
Received 22 January 2004, received in f inal f orm 3 June 2004. Accept ed 19 July 2004.
Dra. Carolina Aguiar M oreira Kulak - Rua Padre Camargo 262 - 80060-240 Curit iba PR - Brazil. E-mail: [email protected]
BONE M INERAL DENSITY AND SERUM LEVELS OF 25 OH
VITAM IN D IN CHRONIC USERS OF ANTIEPILEPTIC DRUGS
Carolina A.M . Kulak
1, Vict ória Z.C. Borba
1, John P. Bilezikian
2,
Carlos E. Silvado
3, Luciano de Paola
3, César L. Boguszew ski
1ABSTRACT - The aim of this cross sectional study was to evaluate bone mineral density (BMD) and serum lev-els of 25-hydroxy vitamin D (25OHD) in a group of patients taking antiepileptic drugs (AED) for a seizure dis-order. Between May-2001 and January-2003, we evaluated 58 patients (40 women/18 men), 34.4+6 years old living in Curitiba or in its metropolitan area, on antiepileptic therapy for 2 to 38 years (10 on monotherapy /48 on multiple drugs regime). The group was matched by age, gender, and bone mass index to 29 healthy subjects (20 women/ 9 men); 34.2+5.9 years old. Medical history and physical exam were performed on all subjects with particular information sought about fractures and risks factors for osteoporosis. Blood samples were collected for total serum calcium, albumin, phosphorus, creatinine, total alkaline phosphatase, and liv-er function tests. BMD of the lumbar spine, femur and forearm was detliv-ermined by dual enliv-ergy X-ray absorp-tiometry (DXA, Hologic QDR 1000). Between February and April-2003, other blood samples were collected to measure 25OHD, intact paratohormone (PTH) and calcium. Unemployment and smoking history were more frequent among patients than among controls (p<0.05). Fifteen patients had a fracture history, all of which occurred during a seizure. The BMD of the lumbar spine (0.975+0. 13 g/cm2vs. 1.058+0.1 g/cm2; p<0.03) and
of the total femur (0.930+0.1 g/cm2vs. 0.988+0.12 g/cm2; p<0.02) was lower in patients than in controls. In
63.5% of patients and in 24.1 % of controls a T-score < -1.0 in at least one site was seen. The AED users had higher total alkaline phosphatase and lower 25OHD (p<0.02). No correlations between BMD and 25OHD were found. The use of phenytoin was correlated with a greater incidence of fractures (RR: 2.38). We conclude that patients on chronic use of AED have alterations in bone metabolism characterized in this study by low-er BMD of the lumbar spine and total femur and lowlow-er slow-erum concentrations of 25OHD.
KEY WORDS: Enzyme-inducing ant iepilept ic drugs, 25OH vit amin D, ost eomalacia.
Densidade m ineral óssea e níveis séricos de 25 OH vit am ina D em usuários crônicos de drogas ant iepilépt icas
RESUMO - O objetivo deste estudo transversal foi avaliar a densidade mineral óssea (DMO) e os níveis de 25hidroxi vitamina D (25OHD) em um grupo de pacientes com epilepsia e usuários crônicos de drogas antiepilépticas (DAE). Entre maio-2001 e janeiro-2003 avaliamos 58 pacientes (40 mulheres/18 homens) residentes em Curitiba ou região metropolitana da cidade, com média de idade 34,4+6 anos e tempo de tratamento entre 2 e 38 anos (10 em monoterapia/48 em politerapia). O grupo de pacientes foi emparelhado por idade, sexo e índice de massa corpórea com 29 indivíduos aparentemente sadios (20 mulheres/9 homens; 34,2+5,9 anos). Pacientes e controles foram submetidos a anamnese e exame clínico, com ênfase na história de fraturas e fatores de risco para osteoporose. Nas visitas foram coletadas amostras de sangue para dosagens de cálcio, albumina, fósforo, creatinina, fosfatase alcalina, transaminases e gama GT. Foi avaliada também a DMO na coluna lom-bar, fêmur e antebraço (DEXA, Hologic QDRW1000®). Entre fevereiro e abril-2003, pacientes e controles foram
chamados para nova coleta de sangue para dosagem da 25OHD e parato-hormônio (PTH) intact. Desemprego e tabagismo foram mais comuns nos pacientes do que nos controles (p<0,05). Quinze pacientes relataram fraturas durante as crises epilépticas. A DMO da coluna lombar (0,975+0,13 g/cm2vs1,058+0,1 g/cm2; p<0,03)
e do fêmur total (0,930+0,1 g/cm2vs 0,988+0,12 g/cm2; p<0,02) foi menor nos pacientes do que controles. Em
63,5% dos pacientes e em 24,1% dos controles foi registrado escore T < -1.0 desvio-padrão em pelo menos um dos sítios avaliados. Os usuários crônicos de DAE apresentaram níveis de fosfatase alcalina mais elevados (p<0,01) e níveis de 25OHD mais baixos (p<0,02 vs controles). Não houve correlação entre a DMO e os níveis de 25OHD. O uso de fenitoína correlacionou-se positivamente com maior incidência de fraturas (RR: 2,38). Concluímos que usuários crônicos de DAE apresentam importantes alterações do metabolismo mineral ósseo, demonstrada no presente estudo através de valores menores da DMO em coluna lombar e fêmur e níveis séricos diminuídos de 25OHD.
Epilepsy is a chronic condit ion charact erized by recurrent clinical event s or epilept ic crises, w hich occur in t he absence of a met abolic- t oxic disease or f ever. World epidemiologic dat a place t he inciden-ce of t his disease f rom 11 t o 131/100000, individu-als per year1. To prevent seizures, ant iepilept ic or
ant iconvulsant drugs (AED) are used. The AED in common use are carbamazepine (CBZ), phenyt oin (DPH), phenobarbit one (PB), sodium valproat e (VPA), primidone (PRM ), lamot rigina (LTG) and t he benzodiazepines, clobazan (CLB) and clonaze-pan (CZP). The chronic use of AED can af f ect bone and mineral met abolism2-6. St udies indicat e t hat 20
t o 60% of AED users can develop ricket s or ost eo-malacia, especially among older and inst it ut ionali-zed pat ient s. How ever, in out pat ient populat ions, some st udies have not demonst rat ed a delet erious ef f ect of AED on bone met abolism7-9. Drugs such
as CBZ, PB, PRM and DPH are know n t o induce he-pat ic mixed f unct ion oxidase act ivit y t hroughout t he microsomal enzymes (P450) in t he liver. They are t hought t o af f ect bone and mineral met abo-lism indirect ly by increasing t he met aboabo-lism of vit a-min D, t hereby causing vit aa-min D insuf f iciency or def iciency2,3,6,10. The ot her mechanism of t he AEDs
involves a direct act ion on bone cells, increasing bone resorption and formation. In this way, the AED may influence bone turnover4,5,13. Bot h mechanisms
can be associat ed w it h a reduct ion in bone min-eral densit y (BM D)5,6,11,12. Furt hermore, DPH int erf
e-res w it h cat ion t ransport in many t issues, direct ly inhibit s int est inal calcium t ransport and t oget her w it h PB has been show n t o inhibit vit amin D-medi-at ed calcium absorpt ion. In cont rast , ot her AEDs t hat are descript ively t ermed hepat ic noninducers, do not af f ect vit amin D met abolism. Finally, VPA aff ect s bone met abolism by mechanisms t hat have not yet been ident if ied.
The most common laboratory abnormalities des-cribed in relat ion t o AED are hypocalcaemia, hypo-phosphat emia, elevat ed levels of alkaline phospha-t ase (AP), reduced levels of 25-hydroxy viphospha-t amin D (25OHD) and increased serum parat hyroid hormo-ne (PTH)3,4,10. The chronic use of AED is a well-know n
cause of secondary ost eoporosis14,15. How ever, t he
invest igat ion of pot ent ial abnormalit ies of bone mineral metabolism has not generally been empha-sized in AED users. A survey by Valmadrid et al.16,
revealed t hat only 28 and 41% of pediat ric and adults neurologists, respectively, routinely investiga-te bone metabolism in their patients who were tak-ing AEDs. M oreover, less t han 10% of physicians w ho part icipat ed in t he survey prescribed
prophy-lact ic calcium and vit amin D t o t heir pat ient s on AEDs. Since seizure disorders are chronic and per-sist t hroughout lif e, it is very import ant t o inves-t igainves-t e and preveninves-t meinves-t abolic bone disinves-t urbances in t hese individuals, part icularly since many have ot h-er risk f act ors f or ost eoporosis such as lack of physi-cal act ivit y and reduced exposure t o sunlight3. M
o-reover, increased f ract ures rat es have been descri-bed in pat ient s w it h epilepsy17,18,19.
The aim of t his st udy w as t o evaluat e serum le-vels of 25OHD and bone mineral densit y in a group of ambulat ory pat ient s on AED, living in t he cit y or environs of Curit iba, locat ed in Sout h of Brazil (25º Sout h and 49º West ).
M ETHOD
St udy design – This comparat ive, cross-sect ional st udy evaluat ed 58 pat ient s w it h epilepsy f ollow ed in t he Out -pat ient Epilepsy Clinic of t he Hospit al de Clínicas da Uni-versidade Federal do Paraná in Curit iba, bet w een M ay 2001 and January 2003. The pat ient s w ere compared t o 29 healt hy subject s, mat ched by age, gender and body mass index (BMI), recruited by advertisement and posters. This protocol was approved by the local Institutional Ethic Commit t ee in Research of Human, and inf ormed con-sent w as obt ained f rom all part icipant s.
Inclusion crit eria w ere w omen and men living in Cu-rit iba or it s environs; age equal t o or great er t han 25 years; use of AED f or at least 1 year; regular menses (f or w omen); and w illingness t o part icipat e in t he st udy. Inclusion crit eria f or t he cont rol group w ere individu-als living in Curit iba or it s environs, not t aking AED, and w illing t o part icipat e in t he st udy. Women had t o have regular menses. Each control subject was gender, age and BM I mat ched t o t w o pat ient s. Exclusion crit eria f or bot h groups w ere ment al ret ardat ion; immobilizat ion; overt bone def ormit ies and t he presence of condit ions know n t o aff ect bone met abolism such as hepat ic, hemat ologi-cal, rheumat ologic or renal disorders, hyperparat hyroi-dism, osteogenesis imperfecta, hyperthyroihyroi-dism, gastroin-t esgastroin-t inal disorders (e.g., malabsorpgastroin-t ion), hypogonadism, medicat ions know n t o aff ect bone t urnover e.g. glucort i-coids, bisphosphonat es, t hiazides, ant icoagulant s, GnRH analogues, st eroids.
All pat ient s provided inf ormat ion about t ime of diag-nosis and t reat ment of epilepsy, f requency of seizures, t ype and dose of AED and previous f ract ures. A ques-t ionnaire assessing ques-t he risk f acques-t ors of osques-t eoporosis such as smoking, alcohol use, calcium and caff eine int ake, lack of physical act ivit y, f amily hist ory of ost eoporosis w as recorded f or all subject s. A complet e medical hist ory and physical exam was performed. BMI was calculated by w ei-ght in kilograms (kg) divided by t he heiei-ght in square met ers (m2).
egori-zed into three tertiles: < 400 mg, 400-800 mg, and >800mg. Because caf f eine cont ent of brew ed beverages varies w idely, t he caf f eine cont ent of 8 ounces of cof f ee, t ea, and cola drinks w as set at 100 mg, 47 mg, and 40 mg, respect ively (20). Average daily caf f eine int ake w as cat -egorized as low (<200 mg), medium 200-400 mg and high (>400 mg). Physical act ivit y w as considered moderat e w hen it w as perf ormed on a regular basis at least t hree hours per w eek.
On the same day of the interview, blood samples were collect ed f or measurement of albumin, phosphorus, cre-at inine, AP, and liver f unct ion t est s. At t he same visit , BM D measurement s of t he lumbar spine, f emur and f o-rearm (DXA, Hologic QDR 1000) w ere made. Bet w een February and April-2003, more blood samples w ere ob-t ained in order ob-t o measure 25OHD, ob-t oob-t al ob-t esob-t osob-t erone, int act PTH and calcium, t o account f or a possible seaso-nal variat ion in serum 25OHD levels.
Biochemical measurement s – Int act parat hyroid hor-mone w as measured in duplicat e by immunochemilu-minescent assay (DPC, Los Angeles, USA). The det ect ion limit w as 1 pg/ml. Int ra-assay variabilit y w as less t han 5.7% w it hin t he concent rat ions range of 72 - 662 pg/ml (normal range, 7 - 53 pg/ml). The 25OHD w as measured in duplicat e by radioimmunoassay (RIA; DiaSorin, M inne-sot a, USA). The det ect ion limit w as 5 ng/ml. The int ra-assay variabilit y w as less t han 12.5% w it hin t he concen-t raconcen-t ions range of 8.6 concen-t o 49 ng/ml (normal range, 9 concen-t o 37 ng/ml). In t his prot ocol, vit amin D def iciency w as def ined by serum levels of 25OHD less than 10 ng/ml. Insufficiency was defined as a 25OHD between 10 and 20 ng/ml21. Total
serum testosterone was measured in duplicate by electro-chemiluminescent assay (Roche Diagnost ics GmbH, M an-nheim, Germany). The det ect ion limit w as 0.02 ng/ml (0.069nmol/l). Int ra-assay variabilit y w as low er t han
4.6% w it hin t he concent rat ions range 0.24 - 3.45 ng/ml (normal range, 280- 880 ng/ml).
Bone mineral densit y – BM D w as perf ormed by dual-energy X-ray absorpt iomet ry on a Hologic QDR - 1000 W (Hologic, Inc., Walt ham, M A). All t est s w ere perf or-med by t he same t echnician. The coeff icient of variabili-t y w as 0.46% avariabili-t variabili-t he lumbar spine and 0.52% avariabili-t variabili-t he proximal f emur. BM D w as expressed as g/cm2and as T
and Z scores. The World Health Organization (WHO) defi-nes ost eoporosis as a T- score < -2.5 and ost eopenia as a T-score bet w een -1.0 and -2.49. Subject s w it h T-scores >-1.0 are considered t o have normal BM D. These crit e-ria have been est ablished only f or Caucasian post meno-pausal w omen, but w e and ot her have applied t hese WHO crit eria also t o premenopausal w omen and men22.
Sit es analyzed w ere lumbar spine (L1 t o L4), proximal f emur (f emoral neck and t ot al hip) and f orearm (ult ra dist al, t ot al radius and dist al 1/3 radius sit e).
St at ist ical analysis – The pat ient s and cont rols w ere mat ched 2:1, w here one healt hy subject present ed w it h age, gender and BM I similar t o t w o pat ient s of t he epi-lepsy group. This correlat ion, 2 cases by 1 cont rol, w as sufficient to maintain statistical power. The variables were analyzed init ially by normalit y t est s, covariat es and his-t ogram analyses. Dishis-t ribuhis-t ion curves w ere expressed as means±SD. Asymmet ric dist ribut ion w as expressed as median values. In t he univariat e analyses, f or cont inu-ous variables, normal dist ribut ion used paramet ric t est s: Student’s t-test and ANOVA were used for repetitive mea-surement s. For t he variables t hat displayed asymmet ric dist ribut ion, non-paramet ric t est s w ere applied: Wil-coxon, Fisher and M cNemar t est s w it h calculat ion of t he odds rat io. The X2t est w as used in t he evaluat ion
of intake of calcium and caffeine, which were established
Table 1. Clinical charact erist ics and risk f act ors t o ost eoporosis in pat ient s and cont rols.
Pat ient s Cont rols
(N = 58) (N = 29) p value
Age (years) 34.6 ±6.1 34.2 ±5.9 NS*
Gender (F/M ) 40/18 20/9 NS* *
BM I (kg/m2) 24.3 ±3.7 24.3 ±4.0 NS*
Unemployement (% ) 53.4 0 p <0.01* *
Smoking (% ) 29.3 6.8 p <0.01* *
Alcohol (% ) 1.7 0 NS* *
Physical act ivit y (% ) 25,8 44.8 NS* *
Low int ake of calcium 60.3 37.9 NS* * *
(<400mg/day) (% )
High int ake of caf f eine 8.6 6.8 NS* * *
(>400mg/day) (% )
Family hist ory of 24.1 31 NS* *
ost eoporosis (% )
Table 2. ASD t herapeut ic regime used by t he pat ient s.
Number Durat ion M edian Average
of pat ient s of drug durat ion of dose per (N=58) exposure (yr) exposure (yr) day (mg)
Carbamazepine 50 1 - 23 7 927.0
Phenobarbit one 36 1 - 20 4 129.1
Phenyt oin 36 1 - 13 4 268.7
Sodium valproat e 28 1 - 14 5 1301
Lamot rigine 16 1 - 5 1,5 233
Clobazan 19 1 - 5 3 20
Clonazepan 05 1 - 4 4 1.8
Table 3. Biochemical evaluat ion of pat ient s and cont rols.
Pat ient s Cont rols
N=58 N=29 p value
Calcium (mg/dl) 8.91±0.38 9.09±0.34 NS*
Phosphat e (mg/dl) 3.67±0.59 3.82±0.64 NS*
Albumin (g/dl) 4.28±0.44 4.34±0.45 NS*
M agnesium (mg/dl) 1.91±0.24 2.01±0.21 NS*
Creat inine (mg/dl) 0.74±0.1 0.81±0.1 NS*
Alkaline phosphat ase (U/l) 144.72±49.30 111.48±32.78 < 0,01* Transaminase oxalalic (U/l) 29.91±7.42 18.40±7.89 NS* Transaminase pyruvat e (U/l) 20.29±8.33 19.34±3.91 NS*
Gama GT U/l # 56.79 (9-180) 19 (6-51) < 0.01* *
PTH (pg/ml) 39.87±17.88 32.58±11.67 NS*
25-OH vit amin D (ng/ml) 28.25±10.34 34.44±12.76 < 0.02* Tot al t est ost erone (ng/dl) ## 373.05±163.7 450.66±179.46 NS* #value is given as median and range; ## in men, 18 pat ient s and 9 cont rols; * t -t est e f or dependent samples; * * Wilcoxon mat ched pair t est .
Table 4. Bone mineral densit y of lumbar spine, f emur and radius.
Sit e Pat ient s Cont rols
(N=58) (N=29) p value
Lumbar spine (g/cm2) 0.975
±0.13 1058±0.10 <0.03 Tot al f emur (g/cm2) 0.930
±0.10 0.988±0.12 <0.02 Femur neck (g/cm2) 0.867
±0.09 0.889±0.12 NS Tot al radius (g/cm2) 0.609
±0.07 0.624±0.09 NS Ult ra-dist al (g/cm2) 0.512±0.06 0.537±0.06 NS Radius (1/3 sit e) (g/cm2) 0.684±0.08 0.690±0.05 NS t -t est f or dependent sample.
as graded values. Correlations among two continuous va-riables w ere run by t he Pearson t est and in t he mult iple-variable analysis, models of logist ic regression, mult iple regression and discriminat e analysis w ere used. Signif i-cance w as set at p < 0.05.
RESULTS
Group epilepsy – A t ot al of 58 pat ient s, 40 (69% ) w omen and 18 men (31% ), 25-47 years old (34.4±6) w ere st udied (Table 1). Thirt y one (53.4% )
pat ient s (3.5% ) w ere not ident if ied as being par-t ial or generalized23. Regarding t he classif icat ion
of seizures, f if t y f our pat ient s (93% ) had simple or complex part ial seizure or part ial seizure t hat are secondarily generalized, f our (7% ) had primarily generalized t onic-clonic seizures and t w o (3.5% ) had a typically juvenile myoclonic epilepsy, presenti-ng w it h myoclonic and t onic-clonic seizures24. Wit h
regard of cont rol of crises, a median of 4 episodes a mont h (0-60) w as relat ed by t he pat ient s.
Cont rol group – Tw ent y nine healt hy subject s
(20 w omen and 9 men), mean age, 34.2 ±5.9 years
(25-45), matched to the epilepsy group were includ-ed in the study. In this group, all the participants w e-re Caucasians and everyone w as employed.
Risk f act ors t o ost eoporosis – Among risk f ac-tors for osteoporosis, the only one that differed was smoking, w it h a great er incidence in t he epilepsy group (Table 1).
Biochemical measurement s – The result s of bio-chemical measurement s of t he st udy group are shown in Table 3. Mean results of routine biochemi-cal testing (total biochemi-calcium, albumin, phosphorus, mag-nesium, creat inine, AP, t ransaminases, and PTH w e-re normal and did not diff er st at ist ically. In t he ma-le group, no st at ist ical diff erence in serum ma-levels of t est ost erone w as f ound. How ever, 8 (44.4% ) pa-t ienpa-t s and 2 (6.8% ) subjecpa-t s f rom pa-t he conpa-t rol group had serum levels low er t han 280 mg/dl. AP w as hi-gher in t he epilept ic group t han t he cont rol (144.7
±49.3U/l vs 111.4±32.7 U/l; p = 0.01), as w as t he case f or gamma GT levels (46.5 ±37.2 U/I vs 19.0± 10.6; p = 0.001). In contrast, AED users had lower
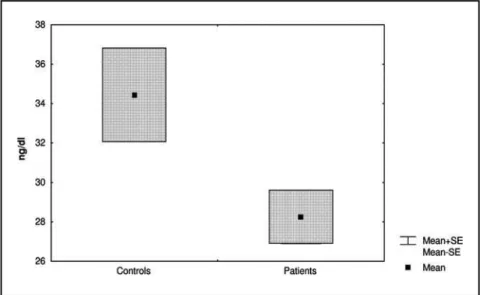
lev-els of 25OHD (28.2 ± 10.3 ng/ml vs 34.4 ± 12.7
ng/ml; p = 0.02) (Fig 1). Tw ent y pat ient s (34.4% ) and two controls (6.8%) had levels of 25OHD below 20 ng/dl (10-20 ng/dl), indicating a greater incidence of vit amin D insuf f iciency in t he AED users t han in t he cont rol group (p=0.01). Alt hough no subject s in t he st udy had levels of vit amin D below t he lo-w er limit of t he ref erence range (i.e., < 10 ng/ml), t he physiological low er limit of normal (< 20 ng/ml) w as f ound f requent ly in t he st udy subject s. Low er levels of 25OHD correlat ed w it h absence of w ork (p= 0.04).
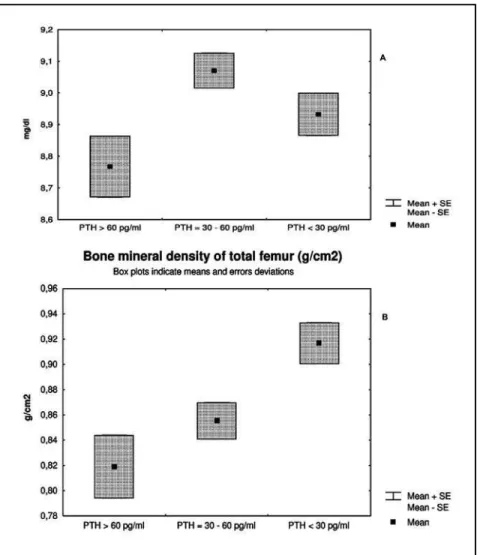
In t he pat ient group, t he mean serum level of PTH w as 39pg/ml (18-88). No correlat ion w as f ound between the PTH and BMD, serum levels of 25OHD, or calcium. How ever, w hen t he pat ient s w ere divided int o t ert iles of PTH [a. > 60 (n= 10), b. PTH bet -w een 30 and 60 (n=26), and c. PTH < 30 pg/ml (n=22)], it w as observed t hat pat ient s in t he highest t ert ile had low er levels of calcium (p <0.03) (Fig 2a). Pat ient s in t his highest t ert ile of PTH show ed BM D of t he proximal f emur t hat w as in t he low er t ert ile (p<0.02 f emur neck, p< 0.03 t ot al f emur) (Fig 2b).
Bone mineral densit y – There w as no correla-t ion becorrela-t w een BM D acorrela-t all sicorrela-t es measured and correla-t he t ime of t reat ment w it h AED. Similarly, no correla-t ion w as f ound becorrela-t w een BM D and serum levels of 25OHD w it h t he except ion of a w eak correlat ion at t he f emoral neck (RR: 0.53). The absolut es
val-Fig 1. Serum levels of 25OHD in pat ient s (n= 58) and Cont rols (n= 29). Box plot s indicat e mean
ues of BM D are show n in Table 4. When WHO cri-teria were applied, osteopenia (T-score -1.0 to -2.49) of at least 1 sit e w as diagnosed at 31 pat ient s (53.4% ) as compared t o only 7 cont rols (24.1% ). Os-t eoporosis by T-score (&lOs-t;-2.5) w as observed Os-t o occur in 7 pat ient s (10.3% ), and no cases w as diagnosed in t he cont rol group. Lumbar spine BM D w as sig-nif icant low er in pat ient s t han in cont rol subject s (0.975±0.13 g/cm2vs 1058
±0.1 g/cm2; p = 0.03).
Tw ent y one pat ient s (36.2% ) and 2 cont rols (6.9% ) had ost eopenia at t his sit e. Ost eoporosis w as diag-nosed in 5 pat ient s (8.6% ). Similarly, t ot al f emur BM D of pat ient s w as signif icant ly low er t han BM D of t he subject s f rom t he cont rol group (0.930 ±0.1 g/cm2vs 0.988
±0.12 g/cm2; p = 0.02). Ost eopenia
of t his sit e w as f ound in 12 pat ient s (17.2% ) but in only 2 cont rols (6.9% ), w hile ost eoporosis w as diagnosed in one pat ient . At t he f emoral neck, no
diff erence bet w een t he groups w as observed BM D of f orearm w as similar bet w een bot h groups.
Types of AED and abnormalit ies of bone met ab-olism – The PTH levels of pat ient s w ho had been exposed t o DPH and PB w ere signif icant ly higher t han t he levels of PTH in pat ient s w ho never had used t hese AEDs. The t ot al f emoral BM D w as signi-f icant low er in t hose pat ient s w ho had used PB (p= 0.03).
AED users and previous f ract ures – Fif t een pa-t ienpa-t s (25.8% ) of pa-t he epilepsy group, f ive men and 10 w omen, w it h mean age of 36.3 years and mean BM I of 23.5 kg/m2, report ed f ract ures relat ed t o a
seizure episode. No associat ion w as observed be-t w een be-t he presence of f racbe-t ures and be-t ype of seizu-res, nor w it h risk f act ors f or ost eoporosis. DPH w as
Fig 2. Pat ient s divided int o t ert iles of PTH levels: > 60 pg/ml (10); 30- 60 pg/ml (26); < 30 pg/ml
(22). 2A: Serum levels of calcium (mg/dl) and PTH 2B: Bone mineral densit y of t ot al f emur
t he most f requent AED among t hese pat ient s {rela-t ive risk=2.38 (1.31- 4.34)}. No signif ican{rela-t diff erence was observed between the BMD of the patient with hist ory of f ract ure t han t he pat ient w it hout a f rac-t ure; how ever 11 (73.3% ) w irac-t h previous f racrac-t ures present ed T score < -1.0 at t he lumbar spine.
The serum levels of 25OHD t ended t o be low er in t he group w ho sust ained f ract ures (p=0.08), w i-t h an incidence of 33% of vii-t amin D insuf f iciency in t his group.
DISCUSSION
Our st udy has evaluat ed 58 young adult s w it h epilepsy and on chronic AEDs. We have demonst ra-t ed signif icanra-t abnormalira-t ies of bone mera-t abolism, charact erized by reduced BM D, reduced 25OHD, and increased AP. Previous studies have related the-se f indings t o chronic uthe-se of AEDs5,6,11,12. Serum
le-vels of calcium and PTH w ere normal and similar t o t he cont rol group. In f act , hypocalcaemia and se-condary hyperparathyroidism, abnormalities initial-ly described as part of a pict ure of ant iconvulsant ricket s or ost eomalacia2,3,10, w ere not observed in
our study. However, when we separated the patients int o subgroups as a f unct ion of PTH levels, a prof i-le of secondary hyperparat hyroidism w it h low er BM D at t he proximal f emur emerged (Fig 2b). The-se data indicate that variable degrees of abnormali-ties in bone metabolism are present in users of AED. On t he ot her hand, t he majorit y of t he pat ient s w i-t h hypovii-t aminosis D preseni-t ed w ii-t h normal levels of PTH t hat may be explained, in part , by an eleva-t ed ineleva-t ake of calcium of eleva-t hese individuals or due eleva-t o abnormal parat hyroid gland responsiveness caused by t he AED.
A relevant f inding of t his st udy w as t he signif i-cant reduction of BMD in the lumbar spine and total femur when compared to the control group. Accor-ding t o WHO crit eria, 63, 5% of t he pat ient s had a diagnosis of ost eopenia / ost eoporosis in at least one of t he sit es measured. This incidence is higher t han uncont rolled st udies report ed in t he lit era-t ure6,11,12. Because of t he cross-sect ional nat ure of
t he present st udy, it w as not possible t o know if t he bone loss is specif ically relat ed t o t he use of AEDs or if t here are ot her reasons f or t he diff eren-ces appreciat ed in t his st udy. Andress et al.11
eval-uat ed t he BM D of a group of AED users prospec-t ively and demonsprospec-t raprospec-t ed a raprospec-t e of bone loss of 1.8% per year.
The great est import ance of a reduct ion BM D is
as a predict or of f ract ure incidence, a point w ell do-cument ed in t he lit erat ure25. Ot her st udies,
espe-cially in inst it ut ionalized pat ient s, have demonst ra-t ed increased f racra-t ure rara-t es in para-t ienra-t s w ira-t h epilep-sy17,18,19. In our st udy, 25.8% of t he pat ient s report
-ed seizure-relat -ed f ract ures, w hich w as not surpris-ingly as many of our pat ient s had uncont rolled sei-zures and required mult iple drugs regime w it h hi-gh doses of AEDs, w hich are risk f act ors f or f alls and f ract ures. One of t he know n ef f ect s of AEDs (DPH, PB and CBZ) on t he liver is t o alt er met abo-lism of vit amin D leading t o a reduct ion in 25OHD f ormat ion. Reduct ions in vit amin D can result in malabsorption of calcium and a secondary hyperpa-rat hyroidism. In t he present st udy, w e demonst ra-t ed low er levels of 25OHD among para-t ienra-t s w ira-t h an incidence of 34.4% of vit amin D insuf f iciency. In order t o improve calcium absorpt ion w hen t he 25-OH Vit amin D level is low, 1,2525-OHD is increased, a conversion st ep mediat ed by PTH. Elevat ion of t he act ive met abolit e of vit amin D, 1,25OHD, can st imulat e bone resorpt ion t hrough of t he recep-t or acrecep-t ivarecep-t ed NF-KB ligand (RANKL), promorecep-t ing maturation of osteoclasts26. Perhaps this mechanism
can cont ribut e t o t he decreased BM D observed in some pat ient s of t his st udy.
Besides drug-induced int erf erence of vit amin D met abolism, geographic f act ors like seasons and lat it udes also are import ant in t he et iology of hy-povit aminosis D. Holick27 demonst rat ed t hat in
the city of Boston (latitude 44 N), there is a decrease in t he skin conversion of 7-dehydrocholest erol t o pre vit amin D, during t he f all and almost absent in t he w int er mont hs. Ot her st udies in more sun-ny regions, w here t he dermal product ion of t he vit amin D precursor w as normal, show ed neit her hypovitaminosis D nor abnormalities of bone meta-bolism in epilept ic pat ient s9,28. For example, male
AED users in Campinas (latitude 20 - 24 degrees Sou-t h) show ed no dif f erence beSou-t w een BM D, 25OHD and 1,25OHD of pat ient s w hen compared t o a cont rol group mat ched by age and BM I9. How ever,
t he simplist ic relat ionship bet w een sunny lat it udes and t he incidence of hypovit amosis D is not alw ays valid. For example, in Recif e, Brasil (lat it ude 10 -12 degrees Sout h), Bandeira et al.29observed t hat
30% of w omen had hypovit aminosis D. Similarly, a study performed with a group of epileptic patients living in Lebanon, show ed an incidence of vit amin D def iciency close t o 50%6. vit amin D def iciency is
also common in Saudi Arabia30. These conf lict ing
of pat ient s w it h epilepsy can inf luence 25OHD le-vels. This w as clearly t he case w it h our pat ient s, in w hom t he incidence of Vit amin D insuf f iciency w as 34% . This w as part icularly not ew ort hy consi-dering t hat subject s had t heir blood collect ed in Curit iba (lat it ude 24-26 degrees Sout h) at t he end of the summer and beginning of fall, a period w hen concentrations of 25OHD are greatest31. Several
stu-dies also have demonst rat ed a decrease of 25OHD serum levels in adult and pediat ric pat ient s3,4,6. As
w as t he case in our st udy, ot hers have not f ound a correlat ion bet w een low er levels of 25OHD and BM D6. We believe t hat ot her causes of bone loss
more specif ic t o epilept ic pat ient s, independent of vit amin D levels, are involved. In our st udy, smok-ing as w ell as unemployment , t he last associat ed w it h a reduct ion of non programmed physical act i-vit ies, are of int erest as possible ot her mechanisms. It is important to emphasize that the high incidence of unemployment f ound is a common f inding in pat ient s w it h chronic act ive epilepsy.
The normal range of serum levels of 25OHD f or most assays is 10 t o 20 ng/ml. How ever, M alabanan et al.32suggested a normal range of 25OHD greater
t han 20 ng/ml just if ied by t he f act t hat levels below 20 ng/ml, are t ypically associat ed w it h elevat ed le-vels of PTH. Anot her st udy has suggest ed a serum level of 25OHD of 30 ng/ml as more appropriat e low er limit of normal33. The import ant point here
is t hat pat ient s can be vit amin D def icient w hile t heir 25OH D levels are st ill w it hin t he laborat ory ref erence range. Such is t he case w it h t he pat ient s report ed in t his st udy.
The f inding of low levels of vit amin D in t his pa-t ienpa-t populapa-t ion has opa-t her implicapa-t ions relapa-t ed pa-t o f ract ure risk, besides bone mineral densit y per se. Vit amin D is increasingly being implicat ed in ot her physiological processes. For example, body sway has been shown to be greater in individuals whose vita-min D levels are low. It is possible, t heref ore, t hat at t he same bone densit y, individuals w it h epilep-sy are at increased risk of f ract ure because t hey are at increased risk of f alling. Anot her int erest ing f in-ding of t he present st udy w as t he higher incidence of low serum levels of total testosterone among ma-le pat ient s. No correlat ion w as observed bet w een t his sex st eroid hormone and BM D. How ever, as hy-pogonadism can lead to bone loss, this finding could be an aggravat ing f act or.
The result s of t his present st udy call at t ent ion t o t he f act t hat pat ient s w it h epilepsy w ho are on
AEDs of t en demonst rat e abnormalit ies in mineral metabolism. We were unable to identify which drug w as more delet erious t o bone met abolism, proba-bly because t here w ere a great number of pat ient on mult iple drugs regimen and a small number of pat ient s t aking t he class of no inducing AED. There w ere 2 point s t hat w e could relat ed signif icant ly to the type of AED. One was the BMD of femur neck w hich w as low er in t he group of pat ient s t hat had t aken PB; and second, t he prevalence of DPH users among t he pat ient s w it h hist ory of f ract ures. These t w o f indings may be explained by t he f act t hat t hese t w o AED have been described t o present a greater number of actions on the bone metabolism. Prevent ive t herapy should be considered f or pa-t ienpa-t s w ho are inipa-t iapa-t ing pa-t reapa-t menpa-t w ipa-t h AED, espe-cially in children and teenagers, where an adequat e amount of calcium and vit amin D is f undament al t o t he accrual of bone peak mass. Finally, a plan t o t reat pat ient s w ho already have lost bone mass and/or w ho have become vit amin D def icient must be implement ed. Such t herapeut ic maneuvers are likely t o avoid f ract ures in t he f ut ure.
In conclusion, w e have show n t hat pat ient s w i-t h epilepsy i-t aking AED and w ho reside in Curii-t iba, Brazil, have decreased BM D at t he lumbar spine and t ot al f emur and a subst ant ial incidence of vi-t amin D insuf f iciency.
Acknow ledgm ent s - We w ould like t o t hank t he
medicine st udent s, Carolina Ferraz da Silva and Daniel F. de Toledo f or t heir help in get t ing some pat ient s in t he Out pat ient s Epilepsy Clinic and f or review ing t heir records.
REFERENCES
1. Engel JJ. Epileptic syndromes. In Seizures and epilepsy: Philadelphia: Davis, 1989:195-201.
2. Christiansen C, Rodbro P, Lund, M. Incidence of anticonvulsant osteoma-lacea and effect of vitamin D; controlled therapeutic trial. Br Med J 1973;4:695-701.
3. Hahn TJ, Hendin BA, Scharp CR, Boisseau VC, Haddad JG. Serum 25-hydroxycalciferol levels and bone mass in children on chronic anticonvul-sivant therapy. N Engl J Med 1975;292:550-554.
4. Valimaki MJ, Tiihonen M, Laitinen K, et al, Bone mineral density measu-red by dual-energy X-ray absorptiometry and novel markers of bone formation and resorption in patients on antiepileptic drugs. J Bone Mi-ner Res 1994;9:631-637.
5. Sato Y, Kondo I, Ishida S, et al. Decreased bone mass and increased bone turnover with valproate therapy in adults with epilepsy. Neurology 2001;57:445-449.
6. Farhat G, Yamout B, Mikati MA, et al. Effect of antiepileptic drugs on bone density in ambulatory patients. Neurology 2002;58:1348-1353. 7. Stephen LJ, McLellan AR, Harrison JH. Bone density and
antiepilep-tic drugs: a case controlled study. Seizure 1999;8:339-342.
8. Kafali G, Erselcan T, Tanzer F. Effect of antiepileptic drugs on bone mine-ral density in children between ages 6 and 12 years. Clin Pediatr 1999;38:93-98.
density, vitamin D and anticonvulsant therapy. Arq Neuropsiquiatr 2000;58:616-620.
10. Bouillon R, Reynaert J, Claes JH, Lissens W, De Moor P. The effect of an-ticonvulsant therapy on serum levels of 25-hydroxy-vitamin D, calcium, and parathyroid hormone. J Clin Endocrinol Metab 1975;41:1130-1135. 11. Andress DL, Ozuna J, Tirschwell D, et al. Antiepileptic drug-induced bone loss in young male patients who have seizures. Arch Neurol 2002;59:781-786.
12. Pack AM, Olarte LS, Morrel MM, Flasher E, Stanley RR, Shane E. Bone mineral density in an outpatient population receiving enzyme-induci-ng antiepileptic drugs. Epilepsy Behav 2003;4:169-174.
13. Verrotti A, Greco R, Latini G, Morgese G, Chiarelli F. Increased bone turnover in prepubertal, pubertal, and postpubertal patients receiving carbamazepine. Epilepsia 2002;43:1488-1492.
14. Thome JF, Cosman F, Lindsay R. Osteoporosis. In Becker KL (ed). Prin-ciples and practice of endocrinology and metabology. 2 Ed. Philadelphia: Lippincott, 1995:567-585.
15. Mulder JE, Kulak CAM, Shane E. Secondary osteoporosis. In Seibel MJ, Robins SP, Bilezikian JP (eds) Dynamics of bone and cartilage metabo-lism. New York: Academic Press 1999;527-545.
16. Valmadri C, Voorhees C, Litt B, Schneyer C. Practice patterns of neuro-logists regarding bone and mineral effects of antiepileptic drug thera-py. Arch Neurol 2001;58:1369-1374.
17. Desai KB, Ribbans WJ, Talor GJ. Incidence of five common fracture types in an institutional epileptic population. Injury 1996;27:97-100. 18. Nilsson OS, Lindholm TS, Elmestedt E, Lindback A, Lindholm TC.
Frac-ture incidence and bone disease in epileptics receiving long-term anti-convulsant drug treatment. Arch Orthop Trauma Surg 1986;105:146-149. 19. Vestergaard P, Tigaran S, Rejnmark L. Fracture risk is increased in
epi-lepsy. Acta Neurol Scand 1999;99:269-275.
20. Lloyd T, Rollings N, Eggli DF, Kieselhorst K, Chinchilli VM Dietary caf-feine intake and bone status of postmenopausal women. Am J Clin Nutr 1997;65:1826-1830.
21. McKenna MJ, Freaney R. Secondary hyperparathyroidism in the
elder-ly; means to defining hypovitaminosis D. Osteoporosis Int 1998;8:S3-S6. 22. Kanis JA, Melton LJ III, Christiansen C, Johnston CC, Khaltaev N. The
diagnosis of osteoporosis. J Bone Miner Res 1994;9:1137-1141. 23. Commission on Classification and Terminology of the International
Lea-gue Against Epilepsy. Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsy 1989;30:389-399.
24. Commission on Classification and Terminology of the International Lea-gue Against Epilepsy. Proposal for revised clinical e electroencephalogra-phic classification of epileptic seizures. Epilepsy 1981;22:489-501. 25. Marshall D, Johnell O, Wedel H. Meta-analysis of how well measures
of bone mineral density predict occurrence of osteoporotic fractures. Br Med J 1996;312:1254-1259.
26. Yasuda H, Shima N, Nakagawa N. Osteoclast differentiation factor is a ligand for osteoprotegerin/osteoclastogenesis-inibitory factor and is identical to TRANCE/RANKL. Proc Natl Acad Sci 1998;95:3597-3602. 27. Holick MF. Vitamin D: new horizons for the 21stcentury. Am J Clin Nutr
1994;60:619-630.
28. Williams C, Netzloff M, Folkerts L, Vargas A, Garnica A, Frias J. Vitamin D metabolism and anticonvulsant therapy: effect of sunshine on inciden-ce of osteomalacia. South Med J 1984;77:834-842.
29. Bandeira FA, Bandeira CH, Freese EC. Occult vitamin D deficiency, and its relationship with bone mineral density, among post menopausal wo-men in Recife, Brazil. J Bone and Miner Res 2003;18:(Suppl 2):5407. 30. Fonseca V, Tongia R, El-Hazmi M, Abu-Aisha H. Exposure to sunlight
and vitamin D deficiency in Saudi Arabian women. Postgrad Med J 1984;60:(707):589-591.
31. Barger-Lux MJ, Heaney RP. Effects of above average summer sun expo-sure on serum 25-hydroxyvitamin D and calcium absorption. J Clin En-docrinol Metab 2002;87:4952-4956.
32. Malabanan A, Veronikis IE, Holick MF. Redefining vitamin D insufficien-cy. Lancet 1998;351:805-806.