Effects
of
glucocorticoid-induced
osteoporosis
on
bone
tissue
of
rats
with
experimental
periodontitis
Luzia
Hermínia
Teixeira
Sousa
a,
Eveline
Valeriano
Moura
a,
Ana
Larissa
Queiroz
b,
Danielle
Val
c,
Hellíada
Chaves
a,b,
Mario
Lisboa
d,
Flávia
Furlaneto
e,
Gerly
Anne
Brito
d,f,
Paula
Goes
a,g,*
aPost-graduationProgramofHealthScience,MedicalSchool,FederalUniversityofCeará
–Sobral,AvenidaComandanteMaurocelioRochaPontes,100
-Derby,Sobral,CE,62.042-280,Brazil
bSchoolofDentistry,FederalUniversityofCeará
–Sobral,R.Cel.EstanislauFrota–Centro,Sobral,CE,62.010-560,Brazil
cPostGraduationProgramRENORBIO,FederalUniversityofPernambuco,Av.ProfessorMoraisRego,1235
–CidadeUniversitária,Recife,PE,50670-901,Brazil
dPost-graduationProgramofMorphologicalScience,DepartmentofMorphology,MedicalSchool,FederalUniversityofCeará
–Fortaleza,RuaDelmirode
Farias,s/n–RodolfoTeófilo,Fortaleza,CE,60.430-170,Brazil
eDepartmentofOral&MaxillofacialSurgeryandPeriodontology,RibeirãoPretoSchoolofDentistry,UniversityofSãoPaulo,Av.doCafé,s/n
–VilaAmelia,
RibeirãoPreto,SãoPaulo,14050-904,Brazil,Brazil
fDepartmentofMorphology,MedicalSchool,FederalUniversityofCeará
–Fortaleza,RuaDelmirodeFarias,s/n–RodolfoTeófilo,Fortaleza,CE,CEP
60.430-170,Brazil
gDepartmentofPathologyandLegalMedicine,MedicalSchool,FederalUniversityofCeará
–Fortaleza,RuaMonsenhorFurtado,S/N–RodolfoTeófilo,
Fortaleza,CE,60.441-750,Brazil
ARTICLE INFO
Articlehistory:
Received31March2016
Receivedinrevisedform4January2017 Accepted17January2017
Keywords:
Periodontitis Osteoporosis Glucocorticoids Alveolarboneloss
ABSTRACT
Objective:Toevaluatetheeffectsofosteoporosisinducedbyglucocorticoid(GIOP)onbonetissueofrats withexperimentalperiodontitis(EP).
Design:48maleWistarratsdividedintogroups:Naïve,EP,GIOPandGIOP+EP.RatsofGIOPandGIOP+EP groupsreceived7mg/kgofdexamethasoneintramuscularlyonceaweekfor5weeks.Following,EPand GIOP+EP groups were subjected to ligature-induced periodontitis. Naïve group experienced no manipulation.After11days,theanimalswereeuthanizedandleftmaxillaecollectedformacroscopic, radiographic,micro-tomographicandmicroscopicanalysisofalveolarboneloss(ABL).Bloodsamples werecollected fordetermination ofbone-specific alkalinephosphatase (BALP)levelsand theright femurswereremovedforradiographicandbiomechanicalanalysis.
Results:EPcausedABLandreducedBALPlevels(p< 0,05),butitdidnotchangethearchitectureor biomechanicsoffemur,comparedtoNaïve.GIOPdidnotcauseABL,butitsignificantlydecreasedalveolar bonemineraldensity(ABMD),bonepercentageandtrabecularthickness(Tb.Th)andincreasedalveolar boneporosity(p< 0.05)andsignificantlyreducedBALPserumlevels,aswellasradiographicdensityand Young’smoduleoffemur,comparedtoNaïve.TherewasagreaterABLingroupGIOP+EPwhencompared toEP(p< 0.05).GIOP+EPcausedagreaterdecreaseonABMD,Tb.Th,bonepercentageandincreased bone porosity (p< 0.05) and also presented a significant reduction in BALP levels (p< 0.05), in radiographicdensityandinYoung’smoduleoffemurcomparedtoEP(p< 0.05).
Conclusions:GIOPcanpotentiatethedestructiveeffectsofEPonalveolarboneandalterthesystemic boneloss,bypromotingboneresorptionandreducingosteoblastactivity.
©2017ElsevierLtd.Allrightsreserved.
1.Introduction
Periodontitisisaninfectious-inflammatoryandhighly
preva-lentdisease,characterizedbydestructionofconnectivetissueand
alveolar bone loss(ABL),and itis consideredthesecondmajor
cause of tooth loss (Tatakis and Kumar, 2005). This disease is
mainlyinitiatedbyoralbiofilm,howeverthedevelopmentofan
* Corresponding author at: Federal University of Ceará – Department of Pathologyand LegalMedicine, Medical School, Rua Monsenhor Furtado,s/n 60441–750,RodolfoTeófilo,Fortaleza/CE,Brazil.
E-mailaddress:[email protected](P.Goes).
http://dx.doi.org/10.1016/j.archoralbio.2017.01.014
0003-9969/©2017ElsevierLtd.Allrightsreserved.
ContentslistsavailableatScienceDirect
Archives
of
Oral
Biology
alteredhostresponseplaysanimportantroleontissuebreakdown (Pihlstrom,Michalowicz,&Johnson,2005).
Osteoporosisis acommondiseasecharacterizedbysystemic
bone loss and impaired bone microarchitecture. It can be a
consequenceofhormonalimbalanceinpostmenopausalwoman
(Jilka,Hangoc,Girasole,Passeri,&Williams,1992),butitalsocan
presentasecondarycause,mainlyasaresultoftheuseofsome
drugs, such as Glucocorticoids (GCs). Glucocorticoid-induced
osteoporosis (GIOP) is the most common cause of secondary
osteoporosis,thefirstcausebefore50yearsofageand thefirst
iatrogenic cause of the disease (Kok & Sambrook, 2009). In
addition,consideringthecontinuousraiseontheprevalenceofGCs
useinthecommunitypopulation(Overman,Yeh,&Deal,2013),it
seems interesting to understand the biological mechanisms
underlyingGIOP.
Intherecentdecades,numerousstudieshavefocusedonthe
associationbetweenosteoporosisand periodontitisat thebone
level.The majorityof thestudieshasfocused ontheeffects of
postmenopausalosteoporosisonthelossof periodontal
attach-ment (Hernández-Vigueras et al., 2015; Juluri et al., 2015).
However,littleisknownabouttheeffectsofGIOPonperiodontal
tissues.OnestudyshowedthatGCscaninduceanalveolarbone
lossinlong-term(28days)treatedmice(Bouvard,Gallois,Legrand,
Audran,&Chappard,2013)andanotheronereportedareductionof
bonedensityintheregionofinteralveolarsepta,insignificantbone
tissuelossofthehorizontaltypeandpathologicalteethmobilityin
periodontal tissues of patients with systemic osteoporosis
(Dmitrieva, Atrushkevich, & Pikhlak, 2006). There is no study
evaluatingtheeffectofGIOPwhentheperiodontalinflammationis
present.Inthiscontext,weaimedtoevaluatetheeffectsofGIOPon
bonetissueofratswithexperimentalperiodontitis.
2.Materialandmethods
2.1.Animalsandstudydesign
Theexperimentswereperformedonforty-eightyoungadult
male(fromtwolitters)Wistarrats(Rattusnorvegicus)fromcentral
AnimalFacilityofFederalUniversityofCeará,weighing180–220g,
keptinappropriatecageswithsixanimalseach.Theanimalswere
housed in standard conditions (12h light-dark cycles and
temperature-controlledrooms)withfood andwater adlibitum.
Theprotocolsforexperimentalproceduresandanimaltreatment
wereapprovedbyAnimalEthicsCommittee(number78/2014)of
FederalUniversityofCeará,Brazil.
Apowercalculationwas performedtodeterminethesample
size.Theanimalwasconsideredthestudyunit.Thesamplesize
wasdeterminedtoprovide80%powertorecognizeasignificant
differenceof20%amonggroupsandthestandarddeviationof15%
witha95%confidenceinterval(p=0.05),consideringthechangein
alveolar bone loss (ABL) as the primary outcome variable.
Therefore,asamplesizeof6ratspergroupwasrequired.
Aftertwoweeksofacclimationtothelaboratoryenvironment,
theratsweredivided,inablindmanner,intofourgroups(n=6):
Naïve, Experimental Periodontitis (EP), Glucocorticoid-induced
osteoporosis(GIOP)and GIOP+EP.Initially, rats fromGIOPand
GIOP+EPgroupsreceivedinjectionsof7mg/kgofdexamethasone
(Decadron,Aché1
–Guarulhos,SP,Brazil)intramuscularly,oncea
weekfor5weeks(Lucindaetal.,2012),andtheonesfromEPgroup
received0.5ml of0.9%salinesolution.Following,theratswere
anesthetized with 100mg/ml ketamine (Cetamin – Syntec1
–
SantanadeParaíba,SP,Brazil)and 20mg/mlxylazine(Xilazin–
Syntec1
–SantanadeParaíba,SP,Brazil)onthedoseof1ml/kg
intramuscularly.In ordertoinduceperiodontitis ratsof EPand
GIOP+EP groups received a sterile nylon thread ligature (3-0;
polysutureNP45330–SãoPaulo, SP,Brazil)aroundthecervical
areaoftheirmaxillaryleftsecondmolars (Bezerraetal.,2000;
Samejima, Ebisu, & Okada, 1990). After 11 days, all rats were
euthanizedwith20mg/kgthiopental(0.5gThiopentax;Cristália,
SãoPaulo,SP,Brazil).RatsofNaïveandGIOPgroupsdidnotreceive
theligature.RatsfromNaïvegroupexperiencednomanipulation.
Itwasperformed2studieswithparallelexperimentalgroups,one
formacroscopicandbiochemicalanalysesandtheotheronefor
microscopicevaluation.
2.2.Macroscopic,radiographicandmicro-computedtomographic(CT) analysesofalveolarbone
Formacroscopicanalysis,theexcisedmaxillaewerefixedin10%
neutralformalinfor24h.Hemi-maxillaewerethendefleshedand
stainedwith1%aqueousmethyleneblueinordertodifferentiate
bonefromteeth.Thentheywereplacedonmicroscopeslidesand
photographed.Theareaofalveolarboneloss(ABL)wasmeasuredby
atrainedandblindedobserver(LHTS),usinganimagingsoftware
(ImageJ1NationalInstitutesofHealth,Washington,DC,USA),as
previouslydescribed(Goes,Lima,Melo,Rego,&Lima,2010).
Thesamespecimensusedformacroscopicstudywere
radio-graphedusingadigitalsystem(DigoraSoredexDigitalSystem1,
Portslade-EastSussex, UK).Thespecimens wereposedoverthe
sensorandtheradiographicimageswereacquiredusing63kVp,
8mA,exposuretimeof0.06sandfocaldistanceof30mm.Bone
mineral density of the maxillae were evaluated using Image J
software,aspreviouslydescribed(Goesetal.,2010).
Thesamenon-demineralizedspecimenswerethenscannedby
a cone beam micro-CTsystem (Skyscan 1172, Bruker, Kontich,
Belgium). The x-ray generator was operated at an accelerated
potentialof50kVwithabeamcurrentof200
m
Aandanexposuretimeof560msperprojection.Imageswereproducedwithavoxel
size of 666
m
m. Using an appropriated software (DataViewer1,version1.5.0,Bruker,Kontich,Belgium),thegenerated
3 dimensionalmodelswererotatedintoa standard positionas
describedpreviously(Lisboaetal.,2015).Linearmeasurementsof
ABL were performedat 3 differentsites: buccal,furcation and
interproximal. For the interproximal site, coronal dataset was
analyzed using appropriated software (CT-Analyser1, version
1.13.5.1+,Bruker,Kontich,Belgium)(Lisboaetal.,2015).Volumetric
analyseswereperformedusingthesamesoftwareappliedforthe
analysisoftheinterproximalsite,aspreviouslydescribed(Lisboa
etal.,2015).Bonemineraldensity(BMD),bonepercentage,bone
porosity, and trabecular thickness (Tb.Th) were assessed. All
micro-CTanalyseswereperformedbyoneblindedandcalibrated
examiner(MRPL).
2.3.Microscopicanalysisofalveolarbone
Anothersetofexperimentwasperformedforhistopathological
analysis. After the euthanasia of the rats, the maxillae were
removed and fixed in 10% neutral buffered formalin and
demineralized in 10% EDTA buffered solution. After complete
decalcification,thespecimensweredehydratedandembeddedin
paraffin. Serial sections,4
m
mthick,wereobtainedinamesio-distaldirection.Thesectionswerestainedwithhematoxylinand
eosin.Sectionsrepresentingtheareabetweenthefirstandsecond
molarswereevaluatedbylightmicroscopy(40magnification).
TheparametersanalyzedwerebasedonthestudybyLeitãoetal.
(2005),using scoresvaryingfrom0 to3.The histopathological
analysiswasperformedbyacertifiedhistologist(GACB).
2.4.Serumlevelsofbone-specificalkalinephosphatase(BALP)
Bloodsampleswerecollectedfromtheorbitalplexus atthe
11thdayaftertheinductionofperiodontitis.Bone-specificalkaline
phosphatase (BALP), a thermosensible isoform of total alkaline
phosphatase, was evaluated using a thermoactivation method
(Whitby & Moss,1975). The samples wereheated to 56C for
10min. Serumlevelsof BALPwerecalculatedby thedifference
betweenheated alkalinephosphatase fromtotal alkaline
phos-phataseinserum(Labtest1
–LagoaSanta,MG,Brazil)(Goes,Melo,
Dutra,Lima,&Lima,2012;Goesetal.,2014).
2.5.Biomechanicaltestingandradiographicdensityoffemur
Therats’rightfemurswerecollectedaftereuthanasiaandfixed
in10%formaldehyde(ReagenProdutosparaLaboratóriosLtda1
–
Rio de Janeiro, RJ, Brazil) for 24h. The specimens were
radio-graphedusingDigoraSoredexSystem1(DentalImagingCompany
Ltd,Portslade-EastSussex,UK)withthesameparametersusedfor
themaxillae.TheseimageswereevaluatedbyImageJ1software.A
regionofinterest(ROI)wascreatedmeasuring0.50.5mm,inthe
formof a square, with473229pixels, and was posed in the
proximalfemurdiaphysis,and thesameevaluatordrewallROI
panels. Grey tone differences were considered the value of
radiographicdensity.
The same non-demineralized femurs were analyzed in a
materialstestingmachine(InstronE10000,InstronCorporation–
Norwood, MA, USA), using a three-point bending procedure.
Femurswerecompresseduntilfailureata displacementrateof
3mm/min (span=20mm)withthe anteriorside down,and all
forceanddisplacementdatawererecordeduntilthespecimenwas
broken.Young’smodulus(MPa) werecalculated,assumingthe
cross-sectional geometryof the femurs wereelipses (Xu etal.,
2014).
2.6.Statisticalanalysis
Thedataarepresentedasmeansstandarderrorsofthemeans
orasmedian(range),whenappropriate.Normalityand
homosce-dasticity of the data were verified. ANOVA followed by the
Bonferronitestwereusedtocomparethemeans,and Kruskal–
WallisandDunn testswereusedtocomparethemedians.The
significancelevelwassetat5%inalltests.Allcalculationswere
performedusingPrism5(GraphPadSoftwareInc.,SanDiego,CA,
USA).Allprotocolsandanalyseswereperformedbyblindedand
calibratedexaminers.
3.Results
3.1.Macroscopic,radiographicandmicro-computedtomographic(CT) analysesofalveolarbone
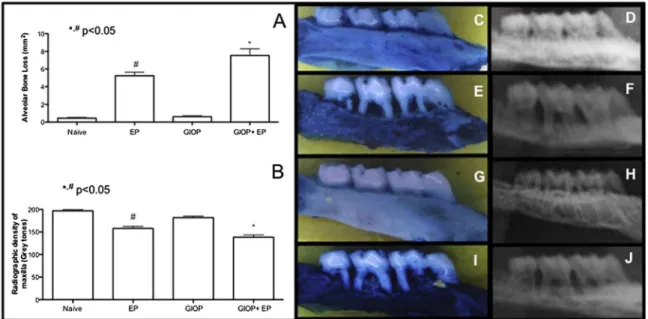
Onthemacroscopicanalysisofhemimaxillae(Fig.1A),Naïve
group(Fig.1C)presentedABLclosetozero,i.e.Ligaturesforeleven
days caused a significant (p<0.05) ABL in group EP, which
presentedfurcationlesionsandrootexposure,whencomparedto
groupNaïve(Fig.1E).TheresponseoftheratstoGIOP(Fig.1G)was
similar to that of the rats of the Naïve group. However, rats
subjectedtoGIOP+EP(Fig.1I)showedgreater(p<0.05)ABLwhen
comparedtogroupEP.
The results of the radiographic density (RD) analysis of
hemimaxillae are depicted on Fig. 1B. Radiographs of EP rats
showedreductionofRDby19%(Fig.1F)(p<0.05)whencompared
toNaïvegroup(Fig.1D).Therewerenosignificantdifferencesin
theRDofhemimaxillaebetweengroupsGIOP(Fig.1H)andNaïve.
However, hemimaxillae of the rats subjected to GIOP+EP had
lowerRD,by12%(Fig.1J)whencomparedtoEPgroup(p<0.05).
Micro-CTanalysisoflinearandvolumetricparameterscanbe
observedinFig.2.Consideringthelinearmeasurements,EPgroup
showedincreasedABLatbuccal(Fig.2A),furcation(Fig.2B)and
interproximal (Fig. 2C) sites, when compared to Naïve group
(p<0.05). GIOP did not affect the alveolar bone level when
comparedtoNaïve(p>0.05).Ontheotherhand,GIOP+EPgroup
presentedagreaterincreaseofABLwhencomparedtoEPinall
three sites analyzed (p<0.05). The assessment of volumetric
parameters revealed that EP reduced BMD (Fig. 2D), bone
percentage (Fig. 2E), trabecularthickness (Tb.Th) (Fig. 2F) and
increasedboneporosity(Fig.2G)inrelationtoNaïvegroup.No
differenceswereobservedbetweenGIOPandEPgroups(p>0.05).
However,groupGIOP+EPpresentedlowerBMD,bonepercentage
and trabecular thicknessand greaterincrease in bone porosity
whencomparedtogroupEP(p<0.05).
Fig.1.A)MacroscopicandB)Radiographicdensityanalysisofthealveolarboneofrats.BarsrepresentthemeansSEMof6animalspergroup.#Significantdifference
comparedtoNaïvegroup.*SignificantdifferencecomparedtoEPgroup(p< 0.05;ANOVAfollowedbyBonferroniTest).Macroscopicandradiographicimagesofhemimaxillae oftheanimalsfromNaïvegroup(CandD),EPgroup(EandF),GIOPgroup(GandH),andGIOP+EPgroup(IandJ).
3.2.Microscopicanalysisofalveolarbone
Periodontalhistopathologicanalysisoftheregionbetweenfirst
andsecondmolars of naïveratsshows thenormalstructure of
gingiva,periodontalligament(PDL),alveolarboneandcementum
(Fig. 3A). The periodontium of rats subjected to experimental
periodontitis(EPgroup)demonstratedaccentuatedinflammatory
cell infiltration, breakdown of alveolar bone, collagen fiber
derangementwithintheperiodontalligament,andresorptionof
cementum,receiving a medianscoreof 3(range,2–3)(Fig.3B;
Table1).TheperiodontaltissueoftheratssubjectedtoGIOPdid
notdemonstrateanychangeonthearchitecturecomparedwith
thenaïverats(Fig.3C;Table1).However,theratssubjectedto
GIOP+EP showed worse bone loss and inflammatoryinfiltrate
thangroupEP(Fig.3D;Table1).
3.3.SerumbiochemicalanalysisofBALP
Serum dosage of BALP was analyzed (Fig. 4). EP caused a
significantdecrease,by27%,onBALPserumlevels(21.642.48U/
L)whencomparedtoNaïve(29.525.14U/L;p<0.05).GIOPalso
causedareductionby41%(17.42.65U/L)onBALPserumlevels
compared to Naive (p<0.05). GIOP+EP group presented a
reductionby55% (13.252.11U/L)onBALPserum levelswhen
comparedtoEP(p<0.05).
3.4.Biomechanicaltestingandradiographicdensityoffemur
AssessingRDoffemur(Fig.5E),thoseratsundergoingonlyEP
(Fig.5B)showednosignificantdifferencewhencomparedtothe
ratsofNaïvegroup(Fig.5A).GIOPcausedasignificantreductionof
RDoffemur(Fig.5C)whencomparedtoNaïveandEPgroups.In
thegroupofratssubmittedtoGIOP+EP,therewasareductionof
RDof femur(Fig.5D)when compared toNaïve and EPgroups
(p<0.05).
We further checked the effects of GIOP and experimental
periodontitisonfemurbiomechanical properties(Fig.5F).After
11daysofligature,groupEPdidnotshowdifferenceonYoung’s
moduluswhencomparedtothefemursofNaïvegroup(p>0.05).
TherewasasignificantdecreaseinYoung’smodulusinthegroup
subjectedtoGIOPwhencomparedtoNaïvegroup,aswellasinthe
groupGIOP+EPwhencomparedtoEPgroup(p<0.05).
4.Discussion
Therehas beenan increase in the useof animal modelsin
studies of initiation and progression of bone diseases, such as
osteoporosis and periodontal disease. The ligature-induced
periodontitis model has been used extensively as a highly
Fig.2. Micro-CTanalysisoflinearandvolumetricparametersofthealveolarboneofrats.A)Buccalsite,B)Furcationsite,C)Interproximalsite,D)BoneMineralDensity (BMD),E)BonePercentage,F)TrabecularThickness(Tb.Th),G)BonePorosity.BarsrepresentthemeansSEMof6animalspergroup.#Significantdifferencecomparedto
Naïvegroup.*SignificantdifferencecomparedtoEPgroup(p < 0.05;ANOVAfollowedbyBonferroniTest).
Fig.3. Microscopicanalysisoftheperiodontaltissuesintheregionbetweenthefirstandsecondmolarsofrats.A)Naïve,B)EP,C)GIOP,D)GIOP+EPgroups.Dentin(d); Cementum(c);AlveolarBone(ab);Gingiva(g);PeriodontalLigament(pdl).Inflammatoryinfiltrate(*)andboneresorption(!).Bars–500mm.Hematoxylin&eosin(H&E). (40magnification).
Table1
Histopathologicalanalysisoftheperiodontaltissuesofhemimaxillaeofrats.
Naïve EP GIOP GIOP+EP Histopathological
Analysis (Scores)
0(0–0)a 3(2
–3) 0(0–0) 3(3–3)a
Dataarepresentedasmedians(extremevalue).
EP=experimentalperiodontitis;GIOP=glucocorticoid-inducedosteoporosis;
a SignificantcomparedtoEP(KruskalWallisfollowedbyDunn
reproduciblemodelthatevaluatestheprogressionofperiodontitis (Bezerraetal.,2000;Goesetal.,2014;Leitãoetal.,2005).Aswith
humanperiodontitis,experimentallyinducedperiodontitisinrats
involves inflammatorycell recruitment with overproduction of
proinflammatory cytokinesand osteolytic enzymes,with
osteo-clast activation, and ultimately leads toalveolarbone and soft
tissueattachmentloss(Bezerraetal.,2000;Bezerra,Brito,Ribeiro,
&Rocha,2002;Goesetal.,2010;Goesetal.,2012,2014;Leitão etal.,2005;Limaetal.,2004;Lisboaetal.,2015;Messoraetal., 2016;Ozdemiretal.,2012;deLimaetal.,2000).Ontheotherhand,
consistentwithourfindings,thereisnoevidencethat
periodonti-tisbyitselfcanprovokesystemicboneloss(Xuetal.,2014).
Systemicriskfactorsmaydetermineaccelerationoftheonsetof
periodontaldiseases(Borrell&Papapanou,2005;Kornman,2008),
as well as increase in the rate of progression and severity of
periodontitis(Genco&Borgnakke,2013).Amongtheseriskfactors,
osteoporosisis consideredone ofthesix mainsystemic factors
(Genco & Borgnakke, 2013). Therefore, using reproducible
experimentalmodels,thepresentstudyinvestigatedtheinfluence
of glucocorticoid-induced osteoporosis on bone tissue of rats
subjectedtoexperimentalperiodontitisassessingdifferentaspects
ofthealveolarboneandfemuraswellastheosteoblasticactivity.
Osteoporosis is mainly caused by postmenopausal estrogen
deficiencyanditsassociationwithperiodontitisitwelldescribed
inliterature(Hernández-Viguerasetal.,2015;Julurietal.,2015).
However,osteoporosismayalsopresentasecondarycause,related
to the long-term use of glucocorticoids (GCs). Considering the
periodontaltissues,tothebestofourknowledge,thisthefirsttime
thattheeffectsofGIOPareevaluatedonexperimental
periodonti-tisinrats.
OurresultsshowedthatGIOPworsenstheABLinratswithEP.
GCsadverselyaffectbonetissueinanumberofways(Compston,
2010).Notably,afterinitiationofGCstherapy,thereisanearlyand
transient increase in bone resorptionin patients withmultiple
sclerosis(Dovioetal.,2004;Teitelbaum,2015).GCsincreasethe
expressionofthemacrophagecolonystimulatingfactor(M-CSF)
and RANKL, and decrease the expression of its soluble decoy
receptor, osteoprotegerin, in stromal and osteoblastic cells
(Canalis, Mazziotti, Giustina, & Bilezikian, 2007; Compston,
2010). It leads toosteoclastogenesis and a prolongation of the
lifespanofosteoclasts(Compston,2010).Inaddition,ithasbeen
reportedthat,wheninflammatorydisorderssuchasperiodontitis
arepresent,GCsmaypotentiatetheresorptiveprocess.Patients
with rheumatoid arthritis showed increased bone degradation
Fig.4.SerumbiochemicalanalysisofBALP.BarsrepresentthemeansSEMof6animalspergroup.#SignificantdifferencecomparedtoNaïvegroup.*Significantdifference
comparedtoEPgroup(p< 0.05;ANOVAfollowedbyBonferroniTest).
Fig.5.Biomechanicaltestingandradiographicdensityanalysesofthefemurofrats.RadiographicimagesofthefemurofanimalsfromA)Naïvegroup,B)EPgroup,C)GIOP group,D)GIOP+EPgroup.E)RadiographicdensityoffemurandF)Young’smodulus(MPa)offemur.BarsrepresentthemeansSEMof6animalspergroup.#Significant
duringthefirstthreemonthsoftherapywithGCswhencompared
tohealthyindividuals(Hall,Spector,Griffin,Jawad,Hall,&Doyle,
1993). This initial rapid and greater bone loss can reflect
persistenceof theprior effects ofinflammatory cytokines, such
as TNF-
a
and IL-1, as wellas the osteoclastic cytokine RANKL(Teitelbaum, 2015). Therefore, these findings can explain the
greaterABLandtheworsemicroarchitectureofthealveolarbone
observedinGIOP+EPratsinthepresentstudy.
GIOP is characterized by increased apoptosisof osteoblasts.
Thereis evidence that GCs decreaseosteoblastogenesis, impair
osteoblastic differentiation and maturation and decrease the
number and function of osteoblasts (Canalis et al., 2007).GCs
alsofavorthedifferentiationofbonemarrowstromalcellstoward
cellsoftheadipocytelineageinsteadoftheosteoblasticlinageby
blockingWnt/
b
-cateninsignalingpathway(Canalisetal.,2007;Compston,2010).Inaddition,whenassociatedwithinflammatory
bonedisorders,suchasperiodontitis,theosteoblasticactivitymay
alsobesuppressedinagreaterway(Algate,Haynes,Bartold,Crotti,
&Cantley,2016).TNF-
a
,IL-1,6and17canperturbtheWntandbonemorphogeneticprotein(BMP)signalingpathways,leadingto
lowerosteoblastdifferentiationandactivity(Walsh&Gravallese,
2010). TNF-
a
can also induce osteoblasts apoptosis (Jilka,Weinstein,Bellido,Parfitt,&Manolagas,1998;Wei,Kitaura,Zhou, Ross,&Teitelbaum, 2005).Thus, thesefindings can justify the
decreasein BALP serum levelsobserved inGIOP and GIOP+EP
groups,sinceBALPisahomodimericglycoproteinthatisanchored
tothemembraneofosteoblastsandconsequentlyitisconsidereda
general indicator of the bone formation rate in skeletal tissue
(Sardiwal,Magnusson,Goldsmith,&Lamb,2013).
5.Conclusion
Insummary,withinthelimitsofthepresentstudy,weconclude
thatGIOPcanpotentiatethedestructiveeffects ofexperimental
periodontitisonalveolarboneofratsandaltertheirsystemicbone
loss, by promoting bone resorption and reducing osteoblast
activity. Nevertheless, more studies are necessary in order to
betterunderstandthebiochemical mechanismsof GCsin bone
cellsduringinflammatoryconditions.
Conflictofinterests
Theauthorshavenoconflictofinteresttodisclose.
Fundings
ThisstudywassupportedbygrantsfromCNPqandFUNCAPand
bytheauthorsthemselves.
Ethicalapproval
Theexperimentalproceduresdescribedherewereapprovedby
theInstitutionalAnimalCareandUseCommittee(#78/2014)and
performed in accordance with the Animal Care Standards of
FederalUniversityofCeará.
Acknowledgments
The authors gratefully thank Socorro França Monte of the
DepartmentofMorphology,FacultyofMedicine,Federal
Universi-tyofCeará,Ceará,Brazil,fortechnicalassistance.
References
Algate,K.,Haynes,D.R.,Bartold,P.M.,Crotti,T.N.,&Cantley,M.D.(2016).The
effectsoftumournecrosisfactor-aonbonecellsinvolvedinperiodontal
alveolarboneloss;osteoclasts,osteoblastsandosteocytes.JournalofPeriodontal
Research,51(5),549–566.
Bezerra,M.M.,deLima,V.,Alencar,V.B.,Vieira,I.B.,Brito,G.A.,Ribeiro,R.A.,etal.
(2000).Selectivecyclooxygenase-2inhibitionpreventsalveolarbonelossin
experimentalperiodontitisinrats.JournalofPeriodontology,71(6),1009–1014.
Bezerra,M.M.,Brito,G.A.,Ribeiro,R.A.,&Rocha,F.A.(2002).Low-dosedoxycycline
preventsinflammatoryboneresorptioninrats.BrazilianJournalofMedicaland
BiologicalResearch,35(5),613–616.
Borrell,L.N.,&Papapanou,P.N.(2005).Analyticalepidemiologyofperiodontitis.
JournalofClinicalPeriodontology,32(Suppl.6),132158.
Bouvard,B.,Gallois,Y.,Legrand,E.,Audran,M.,&Chappard,D.(2013).
Glucocorticoidsreducealveolarandtrabecularboneinmice.JointBoneSpine,80
(1),77–81.
Canalis,E.,Mazziotti,G.,Giustina,A.,&Bilezikian,J.P.(2007).
Glucocorticoid-inducedosteoporosis:Pathophysiologyandtherapy.OsteoporosisInternational,
18(10),1319–1328.
Compston,J.(2010).Managementofglucocorticoid-inducedosteoporosis.Nature
ReviewsRheumatology,6(2),82–88.
Dmitrieva,L.A.,Atrushkevich,V.G.,&Pikhlak,U.A.(2006).Periodontaltissuesstate
inpatientswithsystemicosteoporosis.Stomatologiia(Mosk),85(5),17–19.
Dovio,A.,Perazzolo,L.,Osella,G.,Ventura,M.,Termine,A.,Milano,E.,etal.(2004).
Immediatefallofboneformationandtransientincreaseofboneresorptionin
thecourseofhigh-dose,short-termglucocorticoidtherapyinyoungpatients
withmultiplesclerosis.JournalClinicalEndocrinologyandMetabolism,89,4923–
4928.
Genco,R.J.,&Borgnakke,W.S.(2013).Riskfactorsforperiodontaldisease.
Periodontology2000,62(1),5994.
Goes,P.,Lima,A.P.S.,Melo,I.M.,Rego,R.O.,&Lima,V.(2010).Effectofatorvastatin
onligature-inducedperiodontitisinWistarrats:Radiographicandmacroscopic
analysis.BrazilianDentalJournal,21(3),193–198.
Goes,P.,Melo,I.M.,Dutra,C.S.,Lima,A.P.S.,&Lima,V.(2012).Effectofalendronate
onbone-specificalkalinephosphataseonperiodontalbonelossinrats.Archives
ofOralBiology,57(11),537–544.
Goes,P.,Melo,I.M.,Silva,L.M.C.M.,Benevides,N.M.B.,Alencar,N.M.,Ribeiro,R.A.,
etal.(2014).Low-dosecombinationofalendronateandatorvastatinreduces
ligature-inducedalveolarbonelossinrats.JournalofPeriodontalResearch,49(1),
45–54.
Hall,G.M.,Spector,T.D.,Griffin,A.J.,Jawad,A.S.,Hall,M.L.,&Doyle,D.V.(1993).
Theeffectofrheumatoidarthritisandsteroidtherapyonbonedensityin
postmenopausalwomen.ArthritisandRheumatism,36(11),1510–1516.
Hernández-Vigueras,S.,Martínez-Garriga,B.,Sánchez,M.C.,Sanz,M.,
Estrugo-Devesa,A.,Vinuesa,T.T.,etal.(2015).Oralmicrobiota,periodontalstatusand
osteoporosisinpostmenopausalwomen.JournalofPeriodontology,15,1–15.
Jilka,R.L.,Hangoc,G.,Girasole,G.,Passeri,G.,Williams,D.C.,Abrams,J.S.,etal.
(1992).Increasedosteoclastdevelopmentafterestrogenloss:Mediationby
interleukin-6.Science,257(5066),88–91.
Jilka,R.L.,Weinstein,R.S.,Bellido,T.,Parfitt,A.M.,&Manolagas,S.C.(1998).
Osteoblastprogrammedcelldeath(apoptosis):Modulationbygrowthfactors
andcytokines.JournalofBoneandMineralResearch,13(5),793–802.
Juluri,R.,Prashanth,E.,Gopalakrishnan,D.,Kathariya,R.,Devanoorkar,A.,
Viswanathan,V.,etal.(2015).Associationofpostmenopausalosteoporosisand
periodontaldisease:Adouble-blindcase-controlstudy.JournalofInternational
OralHealth,7(9),119–123.
Kok,C.,&Sambrook,P.N.(2009).Secondaryosteoporosisinpatientswithan
osteoporoticfracture.BestPractice&ResearchClinicalRheumatology,23(6),769–
779.
Kornman,K.S.(2008).Mappingthepathogenesisofperiodontitis:Anewlook.
JournalofPeriodontology,79(Suppl.8),15601568.
Leitão,R.F.,Ribeiro,R.A.,Chaves,H.V.,Rocha,F.A.,Lima,V.,&Brito,G.A.(2005).
Nitricoxidesynthaseinhibitionpreventsalveolarboneresorptionin
experimentalperiodontitisinrats.JournalofPeriodontology,76(6),956–963.
Lima,V.,Vidal,F.D.,Rocha,F.A.,Brito,G.A.,&Ribeiro,R.A.(2004).Effectsoftumor
necrosisfactor-alphainhibitorspentoxifyllineandthalidomideonalveolar
bonelossinshort-termexperimentalperiodontaldiseaseinrats.Journalof
Periodontology,75(1),162–168.
Lisboa,R.P.,Gondim,D.V.,Ervolino,E.,Vale,M.L.,Frota,N.P.,Nunes,N.L.,etal.
(2015).Effectsofelectroacupunctureonexperimentalperiodontitisinrats.
JournalofPeriodontology,86(6),801–811.
Lucinda,L.M.F.,Aaresturup,B.J.V.,Peters,V.M.,Reis,J.E.P.,deOliveira,R.S.M.F.,&
Guerra,M.O.(2012).TheeffectoftheGinkgobilobaextractintheexpressionof
bax,bcl-2andbonemineralcontentofWistarratswithglucocorticoid-induced
osteoporosis.PhytotherapyResearch,27(4),515–520.
Messora,M.R.,Pereira,L.J.,Foureaux,R.,Oliveira,L.F.,Sordi,C.G.,Alves,A.J.,etal.
(2016).FavourableeffectsofBacillussubtilisandBacilluslicheniformison
experimentalperiodontitisinrats.ArchivesofOralBiology,66,108–119.
Overman,R.A.,Yeh,J.Y.,&Deal,C.L.(2013).Prevalenceoforalglucocortidoidusage
intheUnitedStates:Ageneralpopulationperspective.ArthritisCare&Research,
65(2),294–298.
Ozdemir,S.P.,Kurtiş,B.,Tüter,G.,Bozkurt,Ş.,Gültekin,S.E.,Sengüven,B.,etal.
(2012).Effectsoflow-dosedoxycyclineandbisphosphonateclodronateon
alveolarbonelossandgingivallevelsofmatrixmetalloproteinase-9and
interleukin-1binratswithdiabetes:Ahistomorphometricand
immunohistochemicalstudy.JournalofPeriodontology,83(9),1172–1182.
Pihlstrom,B.L.,Michalowicz,B.S.,&Johnson,N.W.(2005).Periodontaldiseases?
Lancet,366(9499),1809–1820.
Samejima,Y.,Ebisu,S.,&Okada,H.(1990).EffectofinfectionwithEikenella
corrodensontheprogressionofligature-inducedperiodontitisinrats.Journalof
PeriodontalResearch,25(5),308–315.
Sardiwal,S.,Magnusson,P.,Goldsmith,D.J.,&Lamb,E.J.(2013).Bonealkaline
phosphataseinCKD-mineralbonedisorder.AmericanJournalofKidneyDisease,
62(4),810–822.
Tatakis,D.N.,&Kumar,P.S.(2005).Etiologyandpathogenesisofperiodontal
diseases?DentalClinicsofNorthAmerica,49(3),491–516.
Teitelbaum,S.L.(2015).Glucocorticoidsandtheosteoclast.ClinicalandExperimental
Rheumatology,33(4(Suppl.92)),37–39.
Walsh,N.C.,&Gravallese,E.M.(2010).Boneremodelinginrheumaticdisease:A
questionofbalance.ImmunologicalReviews,233(1),301–312.
Wei,S.,Kitaura,H.,Zhou,P.,Ross,F.P.,&Teitelbaum,S.L.(2005).IL-1mediates
TNF-inducedosteoclastogenesis.JournalofClinicalInvestigation,115(2),282–290.
Whitby,L.G.,&Moss,D.W.(1975).Analysisofheatinactivationcurvesofalkaline
phosphataseisoenzymesinserum.ClinicaChimicaActa,59(3),361–367.
Xu,X.C.,Chen,H.,Zhang,X.,Zhai,Z.J.,Liu,X.Q.,Qin,A.,etal.(2014).Simvastatin
preventsalveolarbonelossinanexperimentalratmodelofperiodontitisafter
ovariectomy.JournalofTranslationalMedicine,12,284.
deLima,V.,Bezerra,M.M.,deMenezesAlencar,V.B.,Vidal,F.D.,daRocha,F.A.,de
CastroBrito,G.A.,etal.(2000).Effectsofchlorpromazineonalveolarboneloss
inexperimentalperiodontaldiseaseinrats.EuropeanJournalofOralScience,108
(2),123–129.