ABSTRACT
http://dx.doi.org/10.1590/1678-775720150421
Analysis of speech and t ongue m ot ion in norm al
and post- glossect om y speaker using cine MRI
Jinhee HA1, Iel-yong SUNG2, Jang-ho SON2, Maureen STONE3, Robert ORD4, Yeong-cheol CHO2
1- University of Ulsan, Ulsan University Hospital, College of Medicine, Department of Dentistry, Ulsan, South Korea.
2- University of Ulsan, Ulsan University Hospital, College of Medicine, Department of Oral and Maxillofacial Surgery, Ulsan, South Korea. 3- University of Maryland, Department of Oral and Craniofacial Biological Science, Baltimore, United States of America.
4- University of Maryland, Department of Oral and Maxillofacial Surgery, Baltimore, United States of America.
Corresponding address: Yeong-cheol Cho - Department of Oral and Maxillofacial Surgery - College of Medicine - Ulsan University Hospital - University of Ulsan - 290-3, Ulsan University Hospital - Jeonha-dong - Dong-gu - Ulsan City - South Korea - Phone: 82-52-250-7230 - Fax: 82-52-250-7236 - e-mail: cyc73200@naver.com
6XEPLWWHG6HSWHPEHU0RGL¿FDWLRQ-XQH$FFHSWHG-XQH
O
bj ect ive: Since t he t ongue is t he oral st ruct ure responsible for m ast icat ion, pronunciat ion, and swallowing funct ions, pat ient s who undergo glossect om y can be affect ed in various aspect s of t hese funct ions. The vow el / i/ uses t he t ongue shape, w hereas / u/ uses t ongue and lip shapes. The purpose of t his st udy is t o invest igat e t he m orphological changes of t he t ongue and t he adapt at ion of pronunciat ion using cine MRI for speech of pat ient s w ho undergo glossect om y. Mat erial and Met hods: Twent y- t hree cont rols ( 11 m ales and 12IHPDOHVDQGSDWLHQWVHLJKWPDOHVDQG¿YHIHPDOHVYROXQWHHUHGWRSDUWLFLSDWHLQWKH
experim ent . The pat ient s underwent glossect om y surgery for T1 or T2 lat eral lingual t um ors. The speech t asks “ a souk” and “ a geese” w ere spoken by all subj ect s providing dat a for t he vowels / u/ and / i/ . Cine MRI and speech acoust ics were recorded and m easured t o com pare t he changes in t he t ongue w it h vow el acoust ics aft er surgery. 2D m easurem ent s w ere m ade of t he int erlip dist ance, t ongue- palat e dist ance, t ongue posit ion ( ant erior- post erior and superior- inferior) , t ongue height on t he left and right sides, and pharynx size. Vow el
IRUPDQWV))DQG)ZHUHPHDVXUHG5HVXOWV7KHSDWLHQWVKDGVLJQL¿FDQWO\ORZHU) )UDWLRV) S DQGORZHU))UDWLRVWKDWDSSURDFKHGVLJQL¿FDQFH7KLV ZDVVHHQSULPDULO\LQWKHXGDWD3DWLHQWVKDGÀDWWHUWRQJXHVKDSHVWKDQFRQWUROVZLWK
a great er effect seen in / u/ t han / i/ . Conclusion: The pat ient s show ed com plex adapt at ion
PRWLRQLQRUGHUWRSUHVHUYHWKHDFRXVWLFLQWHJULW\RIWKHYRZHOVDQGWKHWRQJXHPRGL¿HG
cavit y size relat ionships t o m aint ain t he value of t he form ant frequencies.
Ke yw or ds: Glossect om y. Cine MRI . Tongue. Speech.
I N TROD UCTI ON
I n r ecent year s, speech adapt at ion has been st udied in pat ient s w ho have received glossect om y su r g e r y f o r o r a l ca n ce r1 5. Po st - g l o sse ct o m y
ar t iculat ion m ay be poor because of ir r egular it y
RI DLU ÀRZ DQG UHGXFHG SDODWDO FRQWDFW UHVXOWLQJ
from irregular deform at ions of t he t ongue. Pat ient s m ay also have lim it ed t ongue range of m ot ion, d ef or m at ion ab ilit y, an d f ib r osis, all of w h ich can reduce speech qualit y. St udies have isolat ed several m aj or fact or s t hat affect speech qualit y aft er glossect om y surgery. Larger t um or size has a m ore negat ive im pact on pat ient art iculat ion and
swallowing funct ion aft er surgery14,23. Tum or locat ion
also im pact s art iculat ion qualit y w it h t he ant erior t ongue having t he biggest im pact on art iculat ion qualit y and t he t ongue base hav ing t he biggest im p act on sw allow in g1 0 , 2 1. Tu m or in v asion an d
radiat ion t reat m ent also affect post - glossect om y sp eech . Pat ien t s w h o u n d er w en t su r g er y p lu s radiat ion t herapy also show ed w orse funct ion t han pat ient s w ho only underw ent surgery13.
I n order t o rest ore t he ext ensive t issue losses of t he oral cavit y w hen m id and large size t um ors are rem oved, reconst ruct ion m ay be perform ed using
DUDGLDOIRUHDUPIUHHÀDS17 or an ant erolat eral t high
XVLQJDIUHHÀDSIRUUHFRQVWUXFWLRQ5,6. Archont aki, et
al.1UHSRUWHGWKDWWKHXVHRIDIUHHÀDSZDV
t he best way t o im prove t he qualit y of life of pat ient s aft er surgery based on an assessm ent of funct ion in
SDWLHQWVZKRXQGHUZHQWIUHHÀDSUHFRQVWUXFWLRQ
Chen, et al.7 ( 2002) , however, report ed t hat pat ient s
w h o u n d er w en t h em i g l o ssect o m y an d p ar t i al
JORVVHFWRP\ GLG QRW QHHG D ÀDS UHFRQVWUXFWLRQ
in t erm s of speech. They found t hat scar t issue
EHQHDWK WKH ÀDS LQWHUIHUHG ZLWK WKHart iculat ory
m ov em en t of t h e t on g u e, an d t h at a p r im ar y cl o su r e m ad e t h e ar t i cu l at i o n m o r e accu r at e aft er hem iglossect om y and par t ial glossect om y. However, Sun, et al.21 ( 2007) report ed no difference
in t he speech degradat ion of pat ient s w ho w ere UHFRQVWUXFWHG ZLWK IUHH ÀDS YV DQ DGMDFHQW ÀDS and Nicollet t i, et al.13 ( 2004) found no difference
EHWZHHQ SULPDU\ DQG ÀDS FORVXUH ,QVWHDG WKH\ f ou n d t h at pr eser v at ion of t h e t ip w as k ey t o ret ent ion of speech qualit y, and t hat loss of t he t ip was as disrupt ive as a hem it ongue glossect om y.
The present paper uses F1 and F2 values for v ow els, alon g w it h t on gu e m ot ion pat t er n s, t o evaluat e t ongue funct ion in pat ient s who underwent p a r t i a l l a t er a l g l o ssect o m y. Cen t r a l i za t i o n o f v o w e l s h a s b e e n o b se r v e d i n sp e a k e r s w i t h glossect om y using F1- F2 plot s4,22, w hich im plies
poor er ar t iculat ion accuracy and a r educt ion in int elligibilit y. Dist inct iveness am ong vow els m ay be m or e im por t an t t h an global v ow el space in GHWHUPLQLQJ YRZHO LQWHOOLJLELOLW\ VLQFH VLJQL¿FDQW expansion of vow el space area can be a product of acoust ic changes in j ust one vow el12. The vow el / i/
LVRIWHQFRQVLGHUHGYHU\GLI¿FXOWIRUJORVVHFWRP\ speakers t o execut e because it requires considerable ant er ior t ongue elevat ion and a for war d t ongue body2 2. I n an ex am inat ion of / i/ , Whit ehill and
FROOHDJXHVIRXQGQRVLJQL¿FDQWGLIIHUHQFHVLQWKH
values of F1 bet w een glossect om y pat ient s and cont rols, but pat ient s had low er F2 values.
Kaj i, et al.9 ( 2007) found differences bet w een
post- glossect om y gender differences in t he form ant frequencies of / i/ . I n fem ales, F2 and F3 values were reduced for pat ient s regarding cont rols. I n m ales, F1 values w ere higher in pat ient s t han in cont rols. They hypot hesized t hat m en and w om en process speech different ly aft er a part ial glossect om y.
I n recent years, im proved im aging m et hodology h as allow ed t h e com b in ed st u d y of st r u ct u r e a n d m o v em en t o f t h e t o n g u e. I n t h e 1 9 5 0 s
FLQHÀXRURJUDSK\ ZDV XVHG WR PHDVXUH WRQJXH
m ovem ent2, and m or e r ecent ly cineradiography
DQGYLGHRÀXRURJUDSK\KDYHEHHQXVHG+RZHYHU
t h er e a r e l i m i t a t i o n s i n cl i n i ca l u se o f X- r ay because of t he risk of radiat ion exposure8. Ot her
alt er nat iv es t o X- ray include ult rasound, w hich provides represent at ions of t he t ongue in m ot ion18
and in 3D19. The ult rasound wave does not pose
any healt h risks and can ident ify t he m orphological changes of t he t ongue during speech or swallowing. Rast adm ehr, et al.17 ( 2008) used ult rasound t o
ex am in e t on gu e v elocit y du r in g t h e speech of lat eral part ial glossect om y pat ient s and report ed t h a t a co m p e n sa t o r y m e ch a n i sm w o r k e d t o increase velocit y of t he residual t ongue14. Magnet ic
Resonance I m aging ( MRI ) has also been used t o obser ve soft t issue clinically. The use of MRI in speech research began wit h t he recording of st eady st at e vow els using st at ic MRI3. St at ic MRI reveals
t he anat om y of st ruct ures in t he vocal t ract such as t he t ongue surface and t he vocal t ract airway. But , st at ic MRI is lim it ed t o quant ifying and m odeling st at ic feat ures, and cannot be used t o t rack t ongue m ot ion during speech20. The int roduct ion of cine
MRI , w hich produces a t im e series of MR im ages, great ly enhanced t he in vivo visualizat ion of t he t ongue’s m ot ion during speech.
The purpose of t his st udy is t o invest igat e t he m or p h olog ical ch an g es of t h e t on g u e an d t h e adapt at ion of pr onunciat ion using cine MRI for speech of pat ient s w ho undergo glossect om y.
M ATERI AL AN D M ETH OD S
This was a ret rospect ive st udy, w hich exam ined d at a t h at h ad b een collect ed t o st u d y sp eech pr oduct ion in glossect om ies. The pr esent st udy focused on vowels t o ascert ain whet her sounds t hat appear t o sound norm al can show com pensat ory ar t iculat or y st rat egies, w hich ar e differ ent fr om cont r ols. This st udy used a 2x 2 fact or ial design w it h repeat ed m easures, in w hich t he t w o fact ors w ere subj ect group ( glossect om ies, cont rols) and vow el ( / i/ , / u/ ) . The repeat ed m easures w ere t he dependent variables indicat ed in “ Dat a analysis” sect ion. Occasionally, gender ( m ale, fem ale) was used as a t hird fact or, or independent variable, for som e of t he com parisons.
Su bj e ct s a n d spe e ch m a t e r ia ls
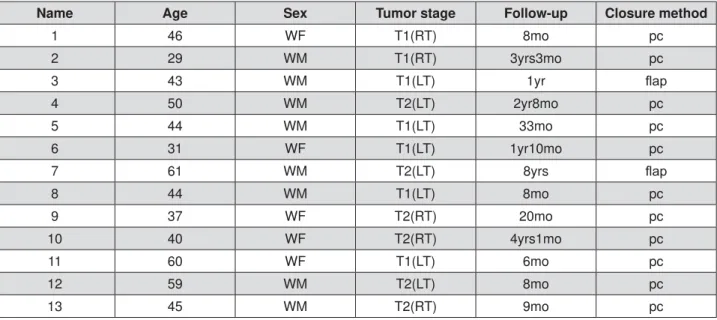
Tw en t y t h r ee n or m al con t r ols an d 1 3 p ost -glossect om y pat ient s ( Figure 1) served as volunt eers for t he st udy. All w ere nat ive speakers of Am erican English. The cont rol group consist ed of 11 m ales and 12 fem ales. The pat ient group consist ed of eight
PDOHVDQG¿YHIHPDOHV7KHDYHUDJHDJHVRIWKH
cont rol group and pat ient group w ere 39.75 years old and 45.3 years old, respect ively. All pat ient s r eceiv ed a par t ial lat er al glossect om y w it h n o subsequent radiat ion or chem ot herapy. Two pat ient s
XQGHUZHQWÀDSUHFRQVWUXFWLRQZLWKDUDGLDOIRUHDUP IUHHÀDSÀDSWKHRWKHUVZHUHVXWXUHGVKXWZLWK
or by head and neck surgeons at Johns Hopkins Hospit al. Subj ect s signed approved consent form s of t he I nst it ut ional Review Board in each locat ion.
Speech t ask s w er e “ a geese,” and “ a souk .” These t asks w ere chosen for several reasons. They can be repeat ed in less t han 1 second, w hich is w it hin t he lim it s of our MRI recording syst em . The
¿UVW 05, IUDPH LV D ³VFKZD´ ZKLFK XVHV D IDLUO\
neut ral t ongue posit ion. For “ souk ”, t he t ongue m oves int o t he / s/ and t hen prim arily backwards int o / u/ and / k/ . For “ geese”, t he t ongue m oves int o t he / g/ and t hen prim arily forwards int o / i/ and / s/ . The w ords use very lit t le j aw opening, so t ongue deform at ion is t he m ain com ponent of m ot ion and bot h vowels are bounded by a velar st op ( / k/ or / g/ ) and a linguo- alveolar fricat ive ( / s/ ) . One pat ient
7ÀDS GLG QRW KDYH DFRXVWLF GDWD IRU X DQG
had no dat a at all for / i/ , since he only recorded “ a souk”. One cont rol did not have acoust ic dat a for
HLWKHUYRZHOGXHWRGDWDFROOHFWLRQGLI¿FXOWLHVEXW
did have MRI dat a. These dat aset s w ere excluded from t he relat ed st at ist ical analyses.
I n st r u m e n t s a n d r e cor din g pr oce du r e
Subj ect s w ere posit ioned in a supine posit ion in t he MRI scanner w it h t he neck coil posit ioned t o im age t he area from t he low er nasal cavit y t o t he upper t rachea.
Au dio r e cor din gs
7ZRDXGLRUHFRUGLQJVZHUHPDGH7KH¿UVWZDV
m ade prior t o t he MRI scan t o provide good qualit y acoust ic dat a for form ant analysis. The subj ect was posit ioned supine in a dent al chair t o sim ulat e t he MRI recording posit ion. The subj ect repeat ed each MRI w ord seven t im es and t hese recordings w ere
XVHG WR PHDVXUH WKH ¿UVW WKUHH IRUPDQWV RI WKH
vow els / i/ and / u/ . The recording was m ade w it h a head m ount ed short- range, unidirect ional, dynam ic m icrophone (Audiot echnica, I nc, Model AT857AMa, Tokyo, Japan) connect ed t o an Olym pus WS- 500M digit al voice recorder. The second recording was m ade inside t he MRI scanner. Subj ect s spoke t he speech t asks t o a m et ronom e before and during MRI scanning. This recording was used t o segm ent t he vowels and ident ify t he MRI t im e- fram es of int erest .
$¿EHURSWLFVXEWUDFWLRQPLFURSKRQH2SWRDFRXVWLFV
Or Yeh u d a , I sr a el ) ca p t u r ed t h e sp eech a n d passively subt ract ed t he MRI noise before recording t he waveform ont o an Olym pus WS- 500M digit al voice recorder. Bot h t he m et ronom e beat s and t he speech w ere recorded.
7KHPHWURQRPHFRQWDLQHGIRXUEHDWV7KH¿UVW
t w o w ere used for t he t w o syllables of t he t ask ( a souk or a geese) and t he second t w o w ere used t o t im e an inhalat ion and exhalat ion. This cont rolled all m ot ion during t he MRI recording. The m et ronom e was also used t o t rigger t he MRI scanner so t he
UHFRUGLQJEHJDQDWWKHWLPHRIWKH¿UVWEHDW7KLV
syst em was based on t he one developed by Masaki, et al.11 ( 1999) .
Cin e M RI r e cor din gs
Cine MRI dat aset s w er e collect ed in m ult iple plan es, w h ile t h e su bj ect r epeat ed t h e speech t asks t o t he beat of t he m et ronom e. Because soft t issue produces a w eak signal and t he t im e fram es ar e shor t ( 38 m sec) , m ult iple r epet it ions of t he w ord w ere collect ed and averaged t o produce a single m ovie. To collect a com plet e dat aset , t he su b j ect r ep eat ed each sp eech t ask f iv e t im es
per slice. A 3-Tesla MR syst em ( Magnet om Tr io, Siem ens Medical Solut ions, Er langen, Ger m any ) was used w it h an eight channel head and neck
Name Age Sex Tumor stage Follow-up Closure method
1 46 WF T1(RT) 8mo pc
2 29 WM T1(RT) 3yrs3mo pc
3 43 WM T1(LT) 1yr ÀDS
4 50 WM T2(LT) 2yr8mo pc
5 44 WM T1(LT) 33mo pc
6 31 WF T1(LT) 1yr10mo pc
7 61 WM T2(LT) 8yrs ÀDS
8 44 WM T1(LT) 8mo pc
9 37 WF T2(RT) 20mo pc
10 40 WF T2(RT) 4yrs1mo pc
11 60 WF T1(LT) 6mo pc
12 59 WM T2(LT) 8mo pc
13 45 WM T2(RT) 9mo pc
Figure 1- Summary of patient data
coil. The param et ers w ere: FOV= 240 m m , voxel size= 1.87x1.87x6.0 m m , t im e- fram es= 26. St acks of Cine MRI im ages w ere recorded in t he sagit t al, coronal and axial planes ( Figure 2) . Depending on t he size of t he subj ect ’s t ongue, t he sagit t al st ack
FRQWDLQHG EHWZHHQ ¿YH DQG QLQH VOLFHV DQG WKH
axial st ack cont ained bet w een 10 and 14 slices. Measur em ent s w er e m ade fr om t he m idsagit t al slice and t he cor onal slice t hat int er sect ed t he second m olar, since t his was encom passed by t he resect ed region.
Acou st ic a n a lyse s
7KH¿UVWWKUHHIRUPDQWV))DQG)ZHUH
m easured for t he / i/ and / u/ in each subj ect using t he form ant t racker of Wavesurfer program . The aut om at ically ext ract ed form ant t raj ect ories w ere visually com pared wit h spect rogram s and m anually correct ed if any errors w ere det ect ed. The linear
SUHGLFWLRQ FRHI¿FLHQWV /3& RUGHU IRU IRUPDQW
t r ack in g w as 1 2 an d t h e an aly sis w in dow size was 50 m s w it h a shift size of 10 m s. The m iddle w indow in each vow el segm ent was used for t he form ant m easurem ent . Each subj ect produced “ a geese” and “ a souk” seven t im es, and t he average form ant values for each subj ect and vow el w ere used in t he analyses.
Cin e M RI a n a lyse s
Th e t ar get v ow el fr am e for / i/ an d / u / w as
GH¿QHGIRUHDFKVXEMHFWDVWKHPLGVDJLWWDOWLPH
fram e w it h t he sm allest t ongue palat e const rict ion occurring wit hin t he acoust ic durat ion of t he vowel. A coronal slice locat ed at t he second m andibular PRODUPHVLDOHGJHZDVLGHQWL¿HGIRUHDFKYRZHO and t he t im e- fram e com parable w it h t he sagit t al slice was chosen for m easur em ent . The second m olar was chosen because lat eral t ongue cancers occur in t his region and it is also t he locat ion of t he high part of t he palat al vault . Measurem ent s were m ade fr om landm ar ks in Figur e 2 using cust om soft ware w rit t en in Mat lab.
Fr om t he landm ar k point s in Figur e 3A, t he follow ing dist ances and lengt hs w ere m easured:
APt ng: ant erior- t o- post erior t ongue lengt h on t he PP’ line: a – c;
APTOT: d ist an ce f r om t h e t on g u e t ip t o t h e post erior pharyngeal wall on t he PP’ line: a – d;
Dpha: dist ance bet w een ant erior and post erior pharyngeal walls on t he PP’ line: c – d;
SIt ng: superior- t o- inferior t ongue height : b – e; Dlip: dist ance bet w een upper and low er lip at m inim um const rict ion;
DTP: dist ance bet w een t ongue and palat e at t he m inim um const rict ion for / i/ and / u/ . For / u/ t he const rict ion locat ion was m ore post erior t han for / i/ .
From t he coronal landm arks ( Figure 3B) , t he follow ing dist ances w ere com put ed:
Sm : t he dist ance bet w een palat al m ucosa and t he m ost upper point of t ongue perpendicular t o t he PPline, m ade on t he side w it h t he sm aller t ongue-palat e dist ance;
Lg: t he dist ance bet w een palat al m ucosa and t he m ost upper point of t ongue at perpendicular t o t he PPline, m ade on t he side w it h t he lar ger t ongue- palat e dist ance.
I n som e st at ist ical analyses, rat ios w ere used t o represent im port ant relat ionships. These w ere:
Dlip/ DTP.: The rat io of lip const rict ion t o t ongue-palat e const rict ion was st udied t o see if t radeoffs w ere m ade in const rict ion size, especially during t he / u/ , w hich uses t w o const rict ions;
Dlip/ Dpha: The rat io of lip dist ance t o pharynx size was st udied t o see if t radeoffs w ere m ade bet w een t he lip and pharynx regions of t he vocal t ract ;
SIt n g/ APt n g: Th e r at i o b et w een v er t i cal an d horizont al t ongue shape was com put ed t o det erm ine w h et h er p at ien t t on g u e sh ap es in d icat ed t h at d if f er en t m u scles w er e u sed f or t on g u e b od y elevat ion from cont rols;
APt ng/ APTOT: The rat io bet w een AP t ongue lengt h and t ongue- plus- pharynx lengt h was m easured t o det erm ine w het her pat ient s had a m ore post erior t ongue posit ion due t o t he m issing t issue;
Sm / Lg: Sym m et ry of sm all- t o- large side t ongue-palat e dist ances was m easured t o corroborat e t hat t he left / right t ongue size asym m et ry creat ed by t he surgical resect ion was absent in t he cont rols.
D a t a a n a lysis
St a t i st i ca l a n a l y si s w a s p e r f o r m e d u si n g SPSS. Gr oup, gender, and vow el w er e assigned
as in d ep en d en t v ar iab les, an d t h e d ep en d en t variables w ere F2/ F1, F3/ F2, F3/ F1, Dlip/ DTP, APTOT/ APt n g, SI / APt n g, Dlip/ Dph a, an d Sm / Lg r at io. Tw o-way Analyses of Variance ( ANOVA) w ere used t o com pare t he effect of group and w ord, in form ant values and int er lip dist ance. Thr ee- way ANOVAs w ere perform ed t o see t he effect s of group, w ord, an d gen der on t on gu e posit ion , t on gu e sh ape,
DQGDLUZD\VL]H7KHOHYHORIVLJQL¿FDQFHZDVVHW
t o p,QDGGLWLRQ3HDUVRQ3URGXFW0RPHQW
&RUUHODWLRQ FRHI¿FLHQWV ZHUH FDOFXODWHG EHWZHHQ
Dlip, Dpha, DTP, SIt ng, APt ng, and APTOT.
RESULTS
Ef f ect of su b j ect g r ou p an d v ow el t y p e on form ant values
7KHSDWLHQWVKDGVLJQL¿FDQWO\ORZHU))UDWLRV
( F= 5.911, p= 0.018) , and low er F3/ F1 rat ios t hat
DSSURDFKHGVLJQL¿FDQFH) S VHH
Tables 1, 2) . The rat io differences occurred because t he F2 and F3 values w ere slight ly sm aller in t he p at ien t s t h an t h e con t r ols ( see Tab le 2 ) . Th is difference was seen prim arily in t he / u/ dat a. Vowel
W\SHZDVVLJQL¿FDQWO\GLIIHUHQWIRUDOOWKUHHUDWLRV
( p< .05) due t o t he low er F2 and F3 for / u/ . The
JURXS[YRZHOLQWHUDFWLRQDSSURDFKHGVLJQL¿FDQFH IRU))S DQGZDVQRWVLJQL¿FDQWIRU)
F1 ( p= 0.849) or F3/ F1 ( p= 0.204) .
Effe ct of su bj e ct gr ou p, w or d, a n d ge n de r on t on gu e posit ion a n d sh a pe
Le ft t o r igh t t on gu e - pa la t e r a t ios ( Sm / Lg)
For pat ient s, t he side in w hich t he glossect om y was perform ed had t he bigger dist ance t o t he palat e in t he coronal plane, alt hough som e asym m et ry was seen in t he cont rols as w ell. Sm / Lg rat ios for / u/ w ere 0.8± 0.31 and 0.5± 0.22 in cont rols and
Group- Vowel
F1 (Hz) F2 (Hz) F3 (Hz) DLip/DTP Sm/Lg* APtng/ APTOT
SI/APtng DLip/Dpha
CL - u mean 359 1746 2561 1.31 0.8 0.8 0.33 0.28 sd 52 265 263 0.68 0.31 0.06 0.07 0.15 PT - u mean 355 1541 2470 1.28 0.5 0.82 0.29 0.33 sd 39 226 189 0.48 0.22 0.05 0.05 0.42 CL - i mean 298 2497 3106 4.58 0.51 0.78 0.38 0.47 sd 41 272 255 3.33 0.42 0.05 0.07 0.78 PT - i mean 310 2388 2928 3.93 0.46 0.77 0.35 0.39 Sd 39 251 268 3.13 0.3 0.03 0.06 0.62
7ÀDSGLGQRWVD\³DJHHVH´DQGGLGQRWKDYHPHDVXUDEOHDFRXVWLFGDWD
Table 1- Results of the formants and anatomical measurements in controls (CL) and patients (PT) for the vowels /u/ and /i/
A B
Figure 3- Landmarks in (A) the midsagittal plane and (B) the coronal plane at the second molar. Landmarks are based on the palatal plane (PP) and a line parallel to PP intersecting tongue tip (PP’). Tissue points used as landmarks include
WKHWRQJXHWLSDWKHLQWHUVHFWLRQRIDSHUSHQGLFXODUOLQHGUDZQIURPSRLQW³H´WRWKH33¶OLQHEWKHPRVWSRVWHULRUSRLQW
of tongue on the PP’ line (c), the intersection point of the pharynx with the PP’ line (d), the most upper point of tongue (e),
pat ient s, respect ively. For / i/ , Sm / Lg rat ios w ere 0.51± 0.42 and 0.46± 0.3 in cont rols and pat ient s, r esp ect iv ely. Th e / u / w as m or e sy m m et r ic in cont rols during / u/ t han / i/ ; pat ient s w ere equally asym m et ric for bot h vowels. These differences were
VWDWLVWLFDOO\VLJQL¿FDQWIRUJURXS6P/J)
p= 0.039) and w ord ( Sm / Lg, F= 4,253, p= 0.043) ( Table1) .
Ton gu e sh a pe ( SI / APt n g)
Lar ger SI / AP rat ios indicat ed a m or e ver t ical t ongue shape t han sm aller rat ios. The rat ios w ere slight ly higher for cont rols t han pat ient s in bot h
YRZHOV DQG DSSURDFKHG VLJQL¿FDQFH )
p= 0.087) . For / u/ , m eans and st andard deviat ions w e r e 0 . 3 3 ± 0 . 0 7 i n co n t r o l s a n d 0 . 2 9 ± 0 . 0 5 in pat ien t s. For / i/ , t h ey w er e 0 . 3 8 ± 0 . 0 7 an d 0.35± 0.06, respect ively. The rat io difference was
prim arily due t o a low er b – e dist ance ( SIt ng) in
WKH SDWLHQW JURXS 7KH UDWLR ZDV VLJQL¿FDQW IRU
w ord ( F= 8.086, p= 0.006) . Gender did not show
DQ\ VWDWLVWLFDO VLJQL¿FDQFH ) S
( Table 2) .
Effe ct of su bj e ct gr ou p, w or d, a n d ge n de r on voca l t r a ct a ir w a y m e a su r e m e n t s
Ph a r yn x siz e ( APt n g/ APTOT, Dlip/ Dph a)
To evaluat e t he Pharynx size, APt ng/ APTOT and Dpha w ere obt ained. Pharynx size show ed t he relat ive evaluat ion about ant erior and post erior m ovem ent of t ongue upon pronunciat ion. Upon pronunciat ion of / u/ , APt ng/ APTOT was 0.80± 0.06 and 0.82± 0.05 i n co n t r o l s a n d p a t i e n t s, r e sp e ct i v e l y. Up o n pronunciat ion of / i/ , APt ng/ APTOT was 0.78± 0.05 and 0.77± 0.03 in cont rols and pat ient s, respect ively. I n
Group F2/F1 F3/F2 F3/F1 Dlip/DTP Sm/Lg APtng/
APTOT
SItng/APtng Dlip/Dpha
groupxword Group 0.018 0.195 0.067 0.555 0.039 0.448 0.087 0.739 word 0 0 0 0 0.043 0.008 0.006 0.006 Group word 0.849 0.09 0.204 0.589 0.139 0.206 0.177 0.121 groupxwordxgender group 0.701 0.499 0.087 0.892 word 0 0.009 0.006 0.004
Table 2- Statistical analyses and p values
DliP Dpha DTP SItng APtng
Dlip pearson correlaton 1 .294* .-306** .454** -0.076 Sig.(2-tailed) 0.013 .010* .000* 0.531
N 71 71 71 71 71
Dpha pearson correlaton 294* 1 -0.059 0.022 -0.177 Sig.(2-tailed) 0.013 0.623 0.858 0.141
N 71 71 71 71 71
DTP pearson correlaton .-306** -0.059 1 -.258* 0.07 Sig.(2-tailed) 0.01 0.623 0.03 0.563
N 71 71 71 71 71
SItng pearson correlaton 454** 0.022 -0.258 1 .242* Sig.(2-tailed) 0 0.858 0.03 0.042
N 71 71 71 71 71
APtng pearson correlaton -0.076 -0.177 0.07 .242* 1 Sig.(2-tailed) 0.531 0.141 0.563 0.042
N 71 71 71 71 71
APTOT pearson correlaton 0.118 475** 0.025 0.23 .782** Sig.(2-tailed) 0.326 0 0.837 0.054 0
N 71 71 71 71 71
FRUUHODWLRQLVVLJQL¿FDQWDWWKHOHYHO FRUUHODWLRQLVVLJQL¿FDQWDWWKHOHYHO
pat ient s, APt ng/ APTOT was som ewhat bigger, because APTOT was shown short ly and it im plied t hat ant erior an d post er ior m ov em en t of t on gu e w as sm all.
+RZHYHULQVWDWLVWLFDOVLJQL¿FDQFHDQDO\VLVWKHUH
ZDVQRVWDWLVWLFDOVLJQL¿FDQFHLQJURXS$3t ng/ APTOT,
) S EXW WKHUH ZDV VLJQL¿FDQW LQ
word ( APt ng/ APTOT, F= 7.602, p= 0.008) . There was no
VWDWLVWLFDOVLJQL¿FDQFHLQJHQGHUFODVVL¿FDWLRQ$3t ng/
APTOT, F= 0 . 3 5 9 , p= 0 . 5 5 7 ) . Upon pr on u n ciat ion of / u / , Dlip/ Dph a w as 0 . 2 8 ± 0 . 1 5 an d 0 . 3 3 ± 0 . 4 2 i n co n t r o l s a n d p a t i e n t s r e sp e ct i v e l y. Up o n pronunciat ion of / i/ , Dlip/ Dpha was 0.47± 0.78 and 0.39± 0.62 in cont rols and pat ient s, respect ively.
,Q VWDWLVWLFDO VLJQL¿FDQFH DQDO\VLV WKHUH ZDV QR
VWDWLVWLFDOVLJQL¿FDQFHLQJURXS'lip/ Dpha, F= 0.112,
S EXWWKHUHZDVVLJQL¿FDQWLQZRUG'lip/
Dpha, F= 8.164, p= 0.006) ( Tables 1 and 2) .
Dlip a n d t on gu e m idsa git t a l dist a n ce s ( Dlip/ DTP)
Dlip and DTP w ere m easured in t he m idsagit t al p l a n e a n d t h e m e a n w a s c a l c u l a t e d . Up o n pr onunciat ion of / u/ , t he values of Dlip and DTP in con t r ols w er e 3 . 9 1 ± 1 . 4 9 m m an d 3 . 2 1 ± 0 . 9 m m , r espect iv ely. The values of Dlip and DTP in pat ient s w ere 3.6± 1.15 m m and 3.05± 0.93 m m , respect ively. Upon pronunciat ion of / i/ , t he values of Dlip and DTP in cont rols w ere 7.64± 2.6 m m and 2.06± 0.86 m m , respect ively. The values of Dlip and DTP in pat ient s w ere 6.4± 2.26 m m and 2.0± 0.69 m m , r espect ively. I n general, values of Dlip and DTP show ed a slight ly higher value in cont rols, but
WKHUHZDVQRVWDWLVWLFDOO\VLJQL¿FDQWYDOXHV'lip/ DTP,
F= 0.352, p= 0.555) in group. How ever, in t erm s of
ZRUGWKHUHZDVVWDWLVWLFDOO\VLJQL¿FDQWYDOXH'lip/
DTP) S UHÀHFWLQJDVPDOOHUOLS
opening for / u/ ( Tables 1 and 2) .
D I SCUSSI ON
When t he part of t ongue was rem oved due t o t ongue cancer, t he shape of t ongue was changed and volum e of t ongue, w hich account ed for oral cavit y, would be changed. The changed t ongue will affect t he pr onunciat ion. Som e st udies r epor t ed t hat t he dam aged t issues induced t he change of
YRFDORUJDQVDIWHUSHUIRUPLQJJORVVHFWRP\DQGÀDS
reconst ruct ion got bet t er in order t o com pensat e
LW+RZHYHURWKHUVWXGLHVUHSRUWHGWKDWWKHVHÀDSV LQGXFHG ¿EURVLV DQG WKHQ LQWHUIHUHG ZLWK WRQJXH
m ovem ent7. I n t his st udy, t hese w er e only t w o
ÀDS SDWLHQWV 7KHLU VSHHFK ZDV QRW QRWLFHDEO\
w orse t han t he prim ary closure pat ient s, alt hough p h y sically, t h e lon g b ack cav it y an d sh or t lip
SURWUXVLRQ RI 7ÀDS ZHUH DPRQJ WKH H[WUHPHV RIWKHSDWLHQWV%HFDXVHÀDSVDUHRIWHQDERYHWKH
upper surface of t he t ongue, as was t he case w it h bot h pat ient s, t he t ongue occupies m ore vert ical
space an d m ay len gt h en t h e or al cav it y. Bot h
ÀDSSDWLHQWVKDGORQJEDFNFDYLWLHVIRUXRQO\
four cont rols and one prim ary closure pat ient had equivalent or longer back cavit y lengt hs. How ever,
WKHUHDUHQRWHQRXJKÀDSSDWLHQWVLQWKLVVWXG\WR
conclusively det erm ine differences in t he effect s of closure procedure.
For st udies on pr onunciat ion of pat ient s w ho u n d er w en t g lossect om y, sp eech in t ellig ib ilit y, a r t i cu l a t i o n , f o r m a n t , a n d v o w el sp a ce w er e prim arily used. However, because t hese approaches w ere evaluat ions on pronunciat ion funct ion aft er t h e su r ger y, t h er e w er e lim it at ion s f or st u dies on how t he shape of t ongue was changed aft er t h e su r g er y or h ow t h e t on g u e w as ch an g ed upon t he pronunciat ion. The present st udy uses Cine MRI , in w hich k- space dat a is collect ed over m ult iple repet it ions of t he speech ut t erance and an ensem ble com binat ion of t he dat a produces a cine series of im ages. From m idsagit t al Cine MRI , one can m easure t he progression of t ongue, lip, laryngeal, and velar m ot ion by t racking t he edges of t hese vocal t ract st ruct ures. From t hese prim ary 2D m easurem ent s ot her useful quant it ies can be calculat ed, such as cavit y lengt hs and m idsagit t al
FRQVWULFWLRQGLVWDQFHV9RZHOVSHFL¿FWLPHIUDPHV
select ed from Cine MRI sequences should reveal t he st rat egies and effect iveness of t ongue m ot ion adapt at ions in post - glossect om y pat ient s, w hen com pared w it h t he acoust ic out put .
I n t his st udy, Cine MRI was used in order t o invest igat e t he changed shape of t ongue and how t he com pensat ory m echanism of t ongue occurred upon pronunciat ion. The subj ect s w ere induced t o m ake pronunciat ion and Cine MRI was recorded. The part icular pronunciat ion was capt ured and t he t hr ee- dim ensional st r uct ur e of t ongue occur r ed upon pr onunciat ion. We supposed t hat phar y nx size was different bet w een t w o groups in analysis of MRI , but t here was alm ost no change in fact . Changes caused by glossect om y w ere Sm / Lg and SIt ng of t ongue. Changes of Sm / Lg w ere, of course, caused by glossect om y and SIt ng was show n less in t he group of pat ient s. Less SIt ngLPSOLHGÀDWWHU t ongue. Therefore, in form ant analysis, F2 and F3 of group of pat ient s showed low and t he pronunciat ion of v ow el w as dist or t ed. Th er e w as st at ist ically
VLJQL¿FDQFH LQ )) DQG )) YDOXHV EHWZHHQ
groups ( p= 0.018, p= 0.067) . Upon pronunciat ion of / i/ in group of pat ient s, t he t ongue t ended t o be
ÀDWDQGOLSWHQGHGWREHFORVHG
of m ale pat ient s, F1 w as incr eased m or e upon pr onunciat ion of / i/ and it w as consist ent w it h st udies of Kaj i, et al.9 ( 2007) . I n pr onunciat ion
of / u / , Dlip, SIt n g, an d DTP d id n ot sh ow m u ch differences bet w een group of pat ient s and cont rol gr oup, but in pr onunciat ion of / i/ , Dlip and SIt ng were different . Since t he t ongue should m ove m ore upon pronunciat ion of / i/ , a group of pat ient s was m ore affect ed. Pronunciat ion and shape of t ongue w as ch an ged du e t o glossect om y in t h e gr ou p of pat ien t s. Th er ef or e, t h er e w er e st at ist ically
VLJQL¿FDQFHVLQ))))6P/JDQG6,t ng/ APt ng
bet w een t w o groups.
$QRWKHU LPSRUWDQW ¿QGLQJ RI WKLV VWXG\ ZDV
t o quant ify t he r elat ionship am ong t ongue, lip, an d p h ar y n x u p o n p r o n u n ci at i o n . I n Pear so n correlat ion analysis, Dlip, DTP, SIt ng, and Dpha show ed
VWDWLVWLFDOO\VLJQL¿FDQWFRUUHODWLRQ7DEOH7KHUH
w as cor r elat ion in Dlip an d DTP ( p = 0 . 0 1 ) , SIt n g and DTP ( p= 0.030) , Dlip and SIt ng ( p= 0.000) , and Dlip an d Dph a ( p= 0 . 0 1 3 ) . As Dlip w as in cr eased, DTP w as decr eased. As SIt ng w as incr eased, Dpha was decr eased. As SIt ng was incr eased, DTP was decreased. As DTP was increased in group of pat ient , SIt ng had a t endency t o be decreased. I t im plied t hat a group of pat ient s had adapt at ion funct ion upon pr onunciat ion, and changes of anat om ical st ruct ures affect ed t he form ant .
The front vow el / i/ and t he back vow el / u/ bot h r equir e t ongue body elevat ion, but t he cont act w it h t he palat e is furt her forward for / i/ t han / u/ ,
DQGWKHUHIRUHLPD\EHDPRUHGLI¿FXOWVRXQGIRU
post - glossect om y pat ient s t o produce. The / i/ also requires m ore lat eral cont act bet w een t he t ongue and palat e and lat eral glossect om y pat ient s ar e m issing one side of t he t ongue, m aking t his t ask
PRUH GLI¿FXOW 7KH K\SRJORVVDO QHUYH HQWHUV WKH
t ongue from t he rear, and divides int o branches t hat course ant eriorly. I f a branch is cut , t he funct ion an t er ior t o t h e cu t is disabled. For / i/ a m or e ant erior part of t he t ongue is elevat ed t han for / u/ . I n addit ion, t he / i/ ut ilizes m ore palat al coverage t h an / u / as sh ow n in it s t y pical t on gu e- palat e cont act pat t ern. Since lat eral glossect om y pat ient s ar e m issin g t issu e on on e side of t h e t on gu e,
DGHTXDWHFRYHUDJHPD\EHPRUHGLI¿FXOWIRUL 7KHPLGOLQHGDWHFDQQRWUHÀHFWJURXSGLIIHUHQFHV
t hat result from lat eral feat ures, such as degree of elevat ion in t he lat eral port ions of t he t ongue, and lat eral t ongue- palat e cont act . I t can, how ever, present differences in lip closure bet w een t he t w o vow els. The sound / i/ uses an open lip posit ion and t he sound / u/ uses prot ruded lips. The prot ruded lips cause a const r ict ion t hat is an int egral par t of t he / u/ gest ure and cont rolled t o alt er t he F2 frequency. The lips and t ongue can t rade off in such a way t hat m ore prot ruded lips can com pensat e for a less high t ongue body in / u/ . The result s show ed
t hat lip prot rusion was t he only m idline variable t hat dist inguished pat ient s from cont rols. Therefore,
LW LV SRVVLEOH WKDW SDWLHQWV KDYH PRUH GLI¿FXOW\
w it h / i/ because t hey are unable t o use t he lips t o com pensat e for inadequat e t ongue body height . This st udy is int erest ed in t he t rade- offs bet w een t he lips and t ongue during t hese t w o vow els.
Alt hough t he st udy was lim it ed by t he sm all
QXPEHU RI SDWLHQWV LQ SDUWLFXODU RQO\ WZR ÀDS
r econ st r u ct ion p at ien t s, it p r ov id ed n ew d at a
WKDW TXDQWL¿HG WKH PRUSKRORJLFDO FKDQJHV SRVW
glossect om y sur ger y, and t he adapt at ion of t he t ongue and vocal t ract during speech.
CON CLUSI ON
Ch an ges in lip con st r ict ion an d back cav it y len gt h ar e lik ely t o be com pen sat or y, w h er eas m idline t ongue shape could be com pensat ory or due t o post - surgical lim it at ions. Form ant changes
ZHUH VLJQL¿FDQW EXW LQDXGLEOH VXJJHVWLQJ WKDW FRPSHQVDWLRQ ZDV VXI¿FLHQW &ORVXUH SURFHGXUH
appeared t o have an effect on back cavit y lengt h.
REFEREN CES
1 - Ar ch on t ak i M, At h an asiou A, St av r ian os SD, Kor k olis DP, Farat zis G, Papadopoulou F, et al. Funct ional result s of speech
DQGVZDOORZLQJDIWHURUDOPLFURYDVFXODUIUHHÀDSUHFRQVWUXFWLRQ
Eur Arch Ot orhinolaryngol. 2010; 267: 1771- 7.
2- Ardran GM, Kem p EH. A radiographic st udy of m ovem ent s of t he t ongue in swallow ing. Dent Pract .1955; 5: 252- 61.
3- Baer T, Gore JC, Boyce S, Nye PW. Applicat ion of MRI t o t he analysis of speech product ion. Magn Reson I m aging. 1987; 5( 1) : 1- 7.
4- Baken RJ, Orlikoff RF. Sound spect rography. I n: Baken RJ, edit or. Clinical m easurem ent of speech and voice. San Diego: Singular; 2000. p.258- 66.
5- Borggreven PA, Verdonck- de Leeuw I , Rinkel RN, Langendij k JA, Roos JC, David EF, et al. Swallowing aft er m aj or surgery of t he oral cavit y or oropharynx: a prospect ive and longit udinal assessm ent of pat ient s t reat ed by m icrovascular soft t issue reconst ruct ion. Head Neck. 2007; 29: 638- 47.
6- Bressm ann T, Sader R, Whit ehill TL, Sam m an N. Consonant i n t el l i g i b i l i t y a n d t o n g u e m o b i l i t y i n p a t i en t s w i t h p a r t i a l glossect om y. J Oral Maxillofac Surg. 2004; 62( 3) : 298- 303. 7 - Ch u an j u n C, Z h iy u an Z , Sh aop u G, Xin g u an J, Z h ih on g Z. Speech aft er par t ial glossect om y ; a com par ison bet w een reconst ruct ion and nonreconst ruct ion pat ient s. J Oral Maxillofac Surg. 2002; 60: 404- 7.
8- Hiiem ae KM, Crom pt on AW. Mast icat ion, food t ransport and swallowing. I n: Hildebrand M, Bram ble D, Liem K, Wake D, edit ors. Funct ional ver t ebrat e m or phology. Cam br idge; Belk nap Pr ess, Harvard Universit y Press; 1985. p. 262- 90.
9- Kazi R, Prasad VM, Kanagalingam J, Georgalas C, Venkit aram an R, Nut t ing CM, et al. Analysis of form ant frequencies in pat ient s w it h oral or oropharyngeal cancers t reat ed by glossect om y. I nt J Lang Com m Dis. 2007; 42( 5) : 521- 32.
10- Logem ann JA, Pauloski BR, Radem aker AW, McConnel FM, Heiser MA, Cardinale S, et al. Speech and swallow funct ion aft er t onsol/ base of t ongue resect ion w it h prim ary closure. J Speech Hear Res. 1993; 36: 918- 26.
1HHO$79RZHOVSDFHFKDUDFWHULVWLFVDQGYRZHOLGHQWL¿FDWLRQ
accuracy. J Speech Lang Hear Res. 2008; 51: 574- 85.
13- Nicolet t i G, Sout ar DS, Jackson MS, Wrench AA, Robert son G, Robert son C. Obj ect ive assessm ent of speech aft er surgical t reat m ent for oral cancer; experience from 196 select ed cases. Plast Reconst r Surg. 2004; 113: 114- 25.
14- Rast adm ehr O, Bressm ann T, Sm yt h R, I rish JC. I ncreased m i d sa g i t t a l t o n g u e v e l o ci t y a s i n d i ca t i o n o f a r t i cu l a t o r y com pensat ion in pat ient s w it h lat eral part ial glossect om ies. Head Neck. 2008; 30: 718- 26.
1 5 - Schliephak e H, Neuk am FW, Schm elzeisen R, Var oga B, Schneller H. Long- t er m qualit y of life aft er ablat iv e int raoral t um our surgery. J Craniom axillofac Surg. 1995; 23: 243- 9.
6RQJ<*&KHQ*=6RQJ</7KHIUHHWKLJKÀDSDQHZIUHH ÀDSFRQFHSWEDVHGRQWKHVHSWRFXWDQHRXVDUWHU\%U-3ODVW6XUJ
1984; 37: 149- 59.
17- Sout ar DS, Scheker LR, Tanner NS, McGregor I A. The radial
IRUHDUPÀDSDYHUVDWLOHPHWKRGIRULQWUDRUDOUHFRQVWUXFWLRQ%U
J Plast Surg.1983; 36( 1) : 1- 8.
18- St one M. A 3- dim ensional m odel of t ongue m ovem ent based on ult rasound and x- ray m icr obeam dat a. J Acoust Soc Am . 1990; 87: 2207- 17.
19- St one M, Lundber g A. Thr ee- dim ensional t ongue sur face shapes of English consonant s and vow els. J Acoust Soc Am . 1996; 99: 3728- 37.
20- St ory BH, Tit ze I R, Hoffm an EA. Vocal t ract area funct ions from m agnet ic resonance im aging. J Acoust Soc Am . 1996; 10: 537- 54. 21- Sun J, Weng Y, Li J, Wang G, Zhang Z. Analysis of det erm inant s on speech funct ion aft er glossect om y. J Oral Max illofac Sur g. 2007; 65: 1944- 50.
22- Whit ehill TL, Ciocca V, Chan CT, Sam m an N. Acoust ic analysis of vow els follow ing glossect om y. Clin Linguist Phon. 2006; 20( 2-3) : 135- 40.