rev bras reumatol.2017;57(1):82–84
ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Paraneoplastic
necrotizing
myopathy
–
a
case
report
Miopatia
necrosante
paraneoplásica
–
relato
de
caso
Alberto
Pereira
Ferraz
∗,
Fabio
Freire
José
UniversidadeFederaldeSãoPaulo(UNIFESP),DivisãodeMedicinaInterna,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received30July2013 Accepted16October2013
Availableonline26November2014
Introduction
Immune-mediated necrotizing myopathy is a rare and recentlydescribed formofidiopathicinflammatory myopa-thy,characterizedasanecrotizingmyopathywithminimalor noinflammatoryinfiltrateonmusclebiopsy.Theclinical fea-turesofsymmetricalproximalmuscleweaknessandacuteor subacuteonsetmaybemisunderstoodwithpolymyositisor dermatomyositis.Thisconditionhasawiderangeofreported outcomes,fromfastprogressionwithnoremissionto com-pleterecovery.Tothebestofourknowledgeuptodatethere isnocasereportedinBrazilofimmune-mediatednecrotizing myopathy,andnooneinLatinAmericarelatedtocancer.Here wedescribedacaseofparaneoplasticnecrotizingmyopathy secondaryatubo-ovarianadenocarcinoma.
Case
report
A 61-year-old woman, married, white, was admitted with thechiefcomplaintofpainandprogressiveweaknessofthe lowerlimbs,withascensiontouppermembers,of4weeksof
∗ Correspondingauthor.
E-mail:[email protected](A.P.Ferraz).
development,associatedwithdysphagiaanddysphonia.She alsoreportedweightlossof10kginthatperiod.She previ-ouslyhadhypertensionandhypothyroidism.Sheunderwent atotalhysterectomy21yearsagoduetouterine leiomyomato-sis.Shealsounderwentbariatricsurgery,abdominoplastyand mammaplastyforabout9years.Therewasnohistoryof alco-holism,smokingoruseofrecreationaldrugs.Thefamily his-torywaspositiveforacutemyocardialinfarctionandstroke.
On physical examination the patient was afebrile and appeared well. The pulse was 68bpm, the blood pressure 130×85mmHg, breathing frequency of 20 incursions per minute.Thelungsandheartwerenormal.Therewasa pres-enceofamedianscaronabdomen.Edemaoflowerlimbsand plastering ofcalveswere absent. Neurologicalexamination showedaweaknessofproximalmusclesgraduatedin2and weaknessofdistalmusclesgraduatedin4onascaleof0–5. Thedeeptendonreflexesweregraduatedin1onascaleof0–4. Theplantarcutaneousreflexwasinflexionbilaterally.There werenootherabnormalitiesonneurologicalexamination.
Additionallaboratoryevaluationshowedacreatinekinase of7874U/l(normalrange:26–192),lacticaciddehydrogenase 1350U/l(reference: <50),aspartateaminotransferase 452U/l
http://dx.doi.org/10.1016/j.rbre.2013.10.007
rev bras reumatol.2017;57(1):82–84
83
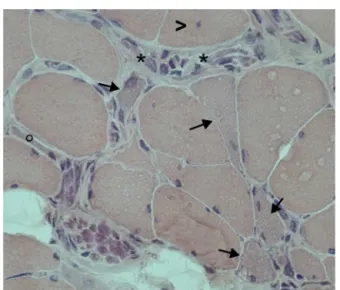
Fig.1–Necrosiswithmacrophagy(asterisk),nuclear centralization(arrowhead),regeneratingfibers(arrows)and atrophicfiber(circle),intheabsenceofinflammatory infiltrate.HEX250.GivenbyDr.BenySchmidt,associate professorofpathologicalanatomy,chiefofthe
NeuromuscularLaboratory–UNIFESP.
(<32),alanineaminotransferase679U/l(<33).Serologicaltests forhepatitisBandCandforHIVwerenegative.In immuno-logicalparameters,theantinuclearfactorwaspositivewith a speckled pattern, titer of 1/160, but anti-JO and anti-nativeDNAantibody,anti-ribonucleoprotein,anti-Ro,anti-La, anti-SCL70 were negative. Cerebrospinal fluid analysiswas positiveforneoplasticcells.ThelevelofCA125wasincreased: 6013U/mL(reference:<35).
Electromyography showed a pattern of predominantly proximalmyopathy,polyphasicmotorunitpotentialsreduced in amplitude and duration. Biopsy of the deltoid muscle revealedatrophyofmusclefibers,withhomogeneousnecrosis and the presenceof macrophagy, with absence of inflam-matory infiltrate (Fig. 1). The search for malignancies of gastrointestinal tract by upper gastrointestinal endoscopy andcolonoscopyresultednegative.Screeningforbreast can-cerwithmammography and researchoftumormarker CA 15.3wasnegative.Computed tomography(CT)ofthechest showed bilateral pulmonary thromboembolism, reinforcing the ideaofunderlying malignancyneoplasia (Fig. 2). ACT of the abdomen and pelvis showed retroperitoneal lym-phadenopathy involving the chain interaortocaval, pelvic lymphadenopathyandlymphonodesaroundthebladder.MRI oftheabdomenandpelvisshowedthepresenceof retroperi-tonealnode6centimetersoflargerdiameterandthepresence ofvascularizedsolidnoduleintherightovary.Magnetic reso-nanceimagingoftheskullandspineshowednoneoplastic focus. White matter ofthe brain hemispheres had foci of ischemia,whilecolumnshoweddegenerativechanges,aswell asatrophyoftheposteriorparaspinal musclegroups, with replacementofmusclefibersbyfat,especiallyinthelumbar spine.
Thebiopsyoftheretroperitonealmassshowed adenocar-cinomainfiltration.Thepatientthenunderwentexploratory laparotomy with bilateral oophorectomy, resection of
Fig.2–Fillingdefectsofsegmentalbranchesoftheright lowerlobeandleftlowerlobeduetopulmonary thromboembolism.
paraaortic mass, omentectomy and pelvic lymphadenec-tomy. Thestudy byimmunohistochemistryconcluded that it was a right tubo-ovarian high-grade serous carcinoma withmetastasistotheleftovary,periaorticlymphonodesand omentum.Thepatientdied2weeksaftersurgeryduetosepsis afterseverepancytopenia,possiblyduetoneoplasticmarrow infiltration, althoughbone marrow biopsyfor confirmation wasnotperformed.
Discussion
Immune-mediatednecrotizingmyopathyisnowrecognized as partof thegroup ofIdiopatic Inflammatory Myopathies that includepolymyositis, dermatomyositis,sporadic inclu-sionbodymyositis,juveniledermatomyositisandamyopathic andhypomyopathicdermatomyositis.Thisuncommon condi-tionisfrequentlyconfusedwithpolymyositisbecauseoftheir symptomsofweaknessofproximalmusclesandhighlevels ofcreatinekinase.1 Itmayoccurinseveralsettings, includ-ingviruses,connectivetissuediseases,inassociationwiththe useofcertaindrugs,includingstatinsandasaparaneoplastic disorder.
TheImmune-mediatednecrotizingmyopathythatoccurs inassociationwithuseofstatinspersistsdespitedrug dis-continuation,unlikethemoretypicalstatin-relatedmyopathy thatresolvesafterdrugdiscontinuation.Incomparisontothe toxicmyopathy, thecourseofanecrotizingmyopathy may beself-limited,and recoverymayoccuraftertheoffending agent is discontinued, occasionally over weeksto months. Likepolymyositisand dermatomyositis,itmayprecede the identification of a tumor. The most common cancers are gastrointestinal tumors, small cell lung cancer,and breast cancer.2
84
rev bras reumatol.2017;57(1):82–84lowamplitude withincreasedinsertionaland spontaneous activitywithfibrillationpotentials,sharpwaves,orrepetitive discharges and to target a muscle forbiopsy. It is recom-mendedthatthesame muscleontheoppositesideshould bechosenforbiopsy.1
The pathophysiology of this disease is still incom-pletelyunderstood.Statin-inducednecrotizingmyopathyhas been associatedwithanantibodyagainstthe 3-hydroxy-3-methylglutaryl-coenzymeAreductase(HMGCR)proteinthat isupregulatedinregeneratingmusclefibers.1Tcell-mediated immune responses as well as humoral factors may be involved.Thesmallnumberofinflammatorycellsinmuscle specimensofpatientswithnecrotizingmyopathyraisesthe possibilityofatoxicmoleculemediatingthesyndrome,but theresponsetosteroidsorimmunoglobulinsismore compat-iblewithanimmune-mediatedprocess.3
Histopathologically, in paraneoplastic necrotizing myopathiesanheterogeneouspatternofnecrosisarefound, rangingfromsparse,segmentalnecrotic lesionstomassive necrosis.2,4,5 Macrophages surround necrotic muscle fibers, andatrophic andregenerating fibersare present. Immuno-stainingrevealsTlymphocytes(CD3)andmacrophages(CD68) aroundnecroticandregeneratingmusclefibers.1
Despite the new evidences, it has recentlybeen shown how rheumatologists and neurologists often differin clas-sificationofmyopathies.Whileneurologists arespecialized indiagnosis utilizing electromyographyand muscle biopsy interpretation, rheumatologists, on the contrary, are typi-cally trainedin making aclinical diagnosis,understanding theroleofautoantibodyassociation.6Nevertheless,effective communication and synergy between subspecialists, using bothstrategiestomakediagnosisandtoclassify,isnowadays requiredtoimprovecommunicationandachieveconsistent conclusioninclinicaltrials.
Conclusion
Immune-mediatednecrotizingmyopathysecondarytostatin hasalreadybeenreportedinLatinAmericabyOpazoetal,7but untilourpresentknowledgethisisthefirstcaseof immune-mediatednecrotizingmyopathyreportedinBrazilandthefirst relatedtoneoplasiainLatinAmerica.
This case report emphasizes the need for clinical sus-picion of cancer in patients with idiopathic inflammatory myopathiesandhighlightstheimmune-mediatednecrotizing myopathy,oneofitsmorerecentlydescribedclinicalforms. Thecaseshowedgoodcorrelationwithwhatisfoundinthe lit-eratureregardingtheclinicalmanifestations.Ovariancancer isnottheneoplasmmostcommonlyfoundin paraneoplas-ticnecrotizingmyopathies.Therefore,thiscasedemonstrates the needto investigateother sitesbeyondgastrointestinal, lung and breast. Therecovery ofthe symptoms ofmuscle weaknessaftertreatmentoftheunderlyingcancercouldnot beassessedduetotheadvancedcancerstageofthepatient.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ErnstFC,ReedAM.Idiopathicinflammatorymyopathies: currenttrendsinpathogenesis,clinicalfeatures,and up-to-datetreatmentrecommendations.MayoClinProc. 2013;88:83–105.
2.WegenerS,BremerJ,KomminothP,JungHH,WellerM. Paraneoplasticnecrotizingmyopathywithamild inflammatorycomponent:acasereportandreviewofthe literature.Oncology.2010;3:88–92.
3.BronnerIM,HoogendijkJE,WintzenAR,VanderMeulenMF, LinssenWH,WokkeJH,etal.Necrotisingmyopathy,an unusualpresentationofasteroid-responsivemyopathy.J Neurol.2003;250:480–5.
4.SmithB.Skeletalmusclenecrosisassociatedwithcarcinoma.J Pathol.1969;97:207–10.
5.UrichH,WilkinsonM.Necrosisofmusclewithcarcinoma: myositisormyopathy?JNeurolNeurosurgPsychiatry. 1970;33:398–407.
6.Christopher-StineL.NeurologistsarefromMars
RheumatologistsarefromVenus:differencesinapproachto classifyingtheidiopathicinflammatorymyopathies.CurrOpin Rheumatol.2010;22:623–6.