w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Anti-CCP
antibodies
are
not
a
marker
of
severity
in
established
rheumatoid
arthritis:
a
magnetic
resonance
imaging
study
夽
Lílian
Santuza
Santos
Porto
a,b,∗,
Wilson
Campos
Tavares
Júnior
c,d,
Dário
Alves
da
Silva
Costa
e,f,
Cristina
Costa
Duarte
Lanna
g,
Adriana
Maria
Kakehasi
gaSantaCasadeBeloHorizonte,Servic¸odeReumatologia,BeloHorizonte,MG,Brazil
bUniversidadeFederaldeMinasGerais(UFMG),FaculdadedeMedicina,ProgramadeSaúdedoAdulto,BeloHorizonte,MG,Brazil
cUniversidadeFederaldeMinasGerais(UFMG),Servic¸odeRadiologiadoHospitaldasClínicas,BeloHorizonte,MG,Brazil
dUniversidadeFederaldeMinasGerais(UFMG),ProgramadeCirurgiaeOftalmologia,BeloHorizonte,MG,Brazil
eUniversidadeFederaldeMinasGerais(UFMG),FaculdadedeMedicina,ObservatóriodeSaúdeUrbanadeBeloHorizonte,Belo
Horizonte,MG,Brazil
fUniversidadeFederaldeMinasGerais(UFMG),ProgramadeSaúdePública,BeloHorizonte,MG,Brazil
gUniversidadeFederaldeMinasGerais(UFMG),FaculdadedeMedicina,DepartamentodoAparelhoLocomotor,BeloHorizonte,MG,
Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received28February2015 Accepted17July2015
Availableonline2December2015
Keywords:
Anti-CCP Diseaseactivity Functionalcapacity Structuraldamage
a
b
s
t
r
a
c
t
Introduction:The presence of anti-CCP is an important prognostic tool of rheumatoid arthritis(RA).Butresearchisstillongoingonits relationshipwithdiseaseactivityand functionalcapacity.
Objectives: To study the relationship betweenanti-CCP and diseaseactivity, functional capacityandstructuraldamageindexes,bymeansofconventionalradiography(CR)and magneticresonanceimaging(MRI),incasesofestablishedRA.
Methods:Cross-sectionalstudywithRApatientswith1–10diseaseduration.Participants underwentclinicalevaluationwithanti-CCP.Diseaseactivitywasassessedusingthe Clin-icalDiseaseActivityIndex(CDAI),andfunctionalcapacitythroughtheHealthAssessment Questionnaire(HAQ).CRanalysiswascarriedoutbytheSharpvanderHeijdeindex(SvdH), andMRIanalysisbyRAMRIS(RheumatoidArthritisMagneticResonanceImageScoring).
Results:Weevaluated56patients,withamedian(IqR)ageof55(47.5–60)years;50(89.3%) par-ticipantswerefemaleand37(66.1%)werepositiveforanti-CCP.Medians(IqR)ofCDAI,HAQ, SvdHandRAMRISwere14.75(5.42–24.97)1.06(0.28–1.75),2(0–8)and15(7–35),respectively. Therewasnoassociationbetweenanti-CCPandCDAI,HAQandSvdHandRAMRISscores.
Conclusion: Ourresultshavenotestablishedanassociationofanti-CCPwiththeseverity ofdisease.Todate,wecannotcorroborateanti-CCPasaprognostictoolinpatientswith establishedRA.
©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheRheumatoidArthritisOutpatientClinic,ServiceofRheumatology,SantaCasadeBeloHorizonte,andatthe Post-GraduatePrograminAdultHealth,MedicineSchool,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.S.S.Porto).
http://dx.doi.org/10.1016/j.rbre.2015.07.018
O
anti-CCP
não
é
um
marcador
de
gravidade
da
artrite
reumatoide
estabelecida:
um
estudo
de
ressonância
magnética
Palavras-chave:
Anti-CCP
Atividadededoenc¸a Capacidadefuncional Danoestrutural
r
e
s
u
m
o
Introduc¸ão: Apresenc¸adoanti-CCPconstituiimportanteferramentaprognósticadaartrite reumatoide(AR).Mas,ainda,investiga-sesuarelac¸ãocomaatividadededoenc¸aea capaci-dadefuncional.
Objetivos: Estudararelac¸ãooanti-CCPeosíndicesdeatividadedadoenc¸a,decapacidade funcionalededanoestrutural,atravésderadiografiaconvencional(RC)ederessonância magnética(RM),emARestabelecida.
Métodos: EstudotransversalcompacientescomAR,comuma10anosdedoenc¸a.Os par-ticipantesforamsubmetidosàavaliac¸ãoclínicacompesquisadoAnti-CCP.Aatividadede doenc¸afoiavaliadaatravésClinicalDiseaseActivityIndex(CDAI)eacapacidadefuncional atravésdoHealthAssessmentQuestionnaire(HAQ).AanálisedaRCfoifeitapeloíndicede SharpvanderHeijde(SmvH)edaRMpeloSistemadePontuac¸ãodeImagempor Ressonân-ciaMagnéticanaArtriteReumatoide(RAMRIS,RheumatoidArthritisMagneticResonance ImageScoring).
Resultados: Foramavaliados56pacientes,commediana(IIq)deidadede55(47,5-60)anos, sendo50(89,3%)dosexofemininoe37(66,1%)anti-CCPpositivos.Asmedianas(IIq)do CDAI,doHAQ,deSmvHedoRAMRISforamde14,75(5,42-24,97),1,06(0,28-1,75),2(0-8)e15 (7-35),respectivamente.Nãohouveassociac¸ãodoanti-CCPcomoCDAI,comoHAQecom osescoresSmvHeRAMRIS.
Conclusão: Nossosresultadosnãoestabeleceramaassociac¸ãodoanti-CCPcomagravidade da doenc¸a.Atéomomento,nãopodemoscorroboraroanti-CCPcomoumaferramenta prognósticaemARestabelecida.
©2015ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theprogressionofrheumatoidarthritis(RA)bringsan evo-lutionarypotentialto varyingdegreesofjoint damageand functionaldisability.Thus,specialattentionshouldbegiven totheidentificationofpoorprognosticindicatorparameters, becauseideally thedefinition oftherapeuticintensitylevel shouldbebasedonreliablepredictorsofseverity.Itisalready knownthatsomefeatures,whenpresent,areassociatedwith aworseoutcomeofthedisease,suchasthepresenceof high-titerrheumatoidfactor,smokingandHLA-DRB1.1,2
Regardingtheprognosticroleofanti-CCP,itsassociation withdiseaseactivityandfunctionalcapacityhasstillnotbeen clarified,althoughmanystudiessuggestthatthese antibod-iesareassociatedwithmoresevereanderosivedisease,3–22
especiallyincasesofinitialRA.9,19–21,23–30 Itisworthnoting
themethodologicalheterogeneityofthestudiesthatanalyzed theassociationofanti-CCPwithstructuraldamage.Although moststudieshavemadeuseofconventionalradiography(CR) asan evaluationtool, differentradiographic scoresystems wereused.Additionally,onlyonestudyalsomadeuseof ultra-sonography(US)inasmallsubgroupofpatients.6Thereareno
studiesthathaveusedmagneticresonanceimaging(MRI)for thispurpose.
Thisstudy aimed toinvestigatethe association of anti-CCPpositivitywithdiseaseseverityasmeasuredbydisease activity,functionalcapacityandstructuraldamage,measured usingCRandMRI.
Patients
and
methods
This is a cross-sectional study, which involved patients seeninanoutpatientclinic.Allparticipantswerediagnosed with established RA according to the American Collegeof Rheumatology (ACR – 1987)31 or the American College of
Rheumatology/The European League Against Rheumatism (ACR/EULAR–201032)criteria,aged18ormoreyearsoldand
with1–10yearsofdiseaseduration.
Because of the possibility of performing MRI, patients withcreatinineclearance<60ml/min/1.73m2,metal
prosthe-sisusers,patientswithaninabilitytoaccesstheexamination table,andpregnantwomenwereexcludedfromthestudy.On theotherhand,patientswithprevioussurgeryand/orfracture inthehandalsowereexcluded.
ThestudywasapprovedbytheResearchEthics Commit-teeand,aftersigningtheconsentform,patientswhoagreed to participateinthe study underwent aclinical evaluation and completed a specific questionnaire containing demo-graphicand clinicaldata(durationofdisease,timeelapsed betweenonsetofsymptomsandRAdiagnosis,smoking his-tory, rheumatoid factor status, presence of extra-articular manifestations, treatment, and CDAI33 and HAQ validated
forPortugueseidiom34).Asampleofbloodwascollectedfor
anti-CCP survey with the use of second-generation meth-ods:EliACCPTM fluorenzyme-immunoassaytest(Pharmacia
Patients were divided into two groups, according to test positivity and to the reference value of the kit used (>10U/ml for fluorenzyme-immunoassay and >5U/ml for chemiluminescence).
Radiographicevaluationwasperformedbymeansofhand andwristCRsinaposterior–anteriorview.X-rayscarriedout intheperioduptothreemonthsbeforeorafterthedata col-lectionwereaccepted.TheSvdHmethod35waschosenforan
analysisofhandsandwrists.21
Asubgroupof35patientswasreferredforMRI examina-tioninuptofourweeksaftertheinterview;forthispurpose, a GE Signa 1.5T HDxT system (GE Healthcare, Milwaukee, WI, USA) was used. For resonance analysis, the RAMRIS36
protocolofthe OutcomeMeasuresinRheumatoid Arthritis ClinicalTrials(OMERACT)forwristandmetacarpophalangeal analysiswasused.Theexaminationswereperformedonthe dominanthand,using coronal(T1- andT2-weighted imag-ingwithfatsuppression),axial(T1-weightedimagingbefore and afterthe use of intravenousgadolinium contrast) and axialandcoronal(T1-weightedimagingwithfatsaturation) sequences.
TheMRIandX-rayanalyzeswereperformedbyasingle radiologistwhowasunawareoftheclinicalconditionofthe patient.TheintraobserveragreementforSvdHscorewas cal-culated,andtheintraclasscorrelationcoefficientwas0.958. Wewereunabletocalculatetheintraclasscoefficientfor RAM-RIS because, to obtain this data, it would benecessary to calculatethevariationcomponent,whichresultedina neg-ativevalue.Thus,adecisionwasmadeinfavorofcalculating theSpearmancoefficient,withavalueof0.96.
Storageofdataandallstatisticalanalyzeswereperformed with the IBM Statistical Package for Social Sciences soft-ware(SPSSversion 19). Forcategoricalvariables, frequency distributionswere presented;and forcontinuous variables, measuresofnumericalsynthesiswereemployed.The asso-ciationbetweencategoricalvariableswasanalyzedusingthe chi-squaredorFisher’sexact test.Thenormalityof contin-uous variables was verified by the Shapiro–Wilk test. For variableswithoutnormaldistribution,theanalysiswas per-formedusing the nonparametric Mann–Whitney Utest. To verifythe associationbetweentwonon-normalcontinuous variables,thenonparametricSpearmantestwasused.Forthis study,a5%significancelevelwasset.
Results
FromAugust2011toAugust2013,56patientswithestablished RAdiagnosiswereevaluated.Table1summarizesthe demo-graphic,clinical,functionalandimagingprofilesofpatients.
Theunivariateanalysisoftheassociationofdemographic and clinical characteristics with the presence of anti-CCP showedthatthisantibodywassignificantlyassociatedwith RF(OR=6.6;95%CI,1.9–22.9;p<0.01)andsmoking(OR=7.8; 95%CI,1.9–31.6;p<0.01).
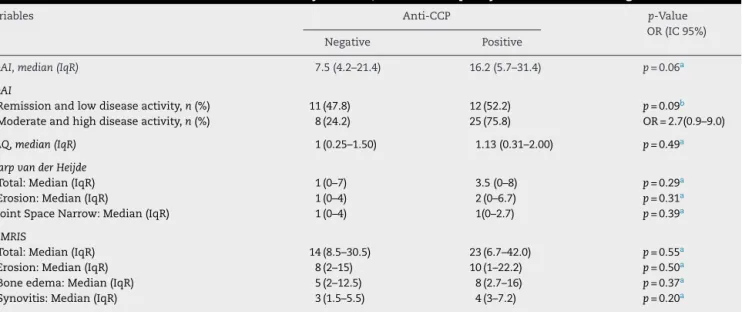
Univariate analysis of anti-CCP association with CDAI, HAQ,SvdH,andRAMRISarepresentedinTable2.Asto dis-easeactivity,theCDAImedianvaluewashigherinthegroupof
Table1–Characteristicsofthepatients.
Variables Measures
Age:Median(IqR) 55(47.5–60.0)
Females:n(%) 50(89.3)
Diseasedurationinyears:Median (IqR)
6(3–9)
Timeelapsedbetweendiseaseand diagnosis,inyears:Median(IqR)
0(0–1)
Positiverheumatoidfactor:n(%) 31(55.4)
Positiveanti-CCP:n(%) 37(66.1)
Smokerorformersmoker,n(%) 25(44.6) Presenceofrheumatoidnodules:n(%) 8(14.3)
Pulmonaryinvolvement:n(%) 6(10.7)
PresenceofSjögren’ssyndrome:n(%) 2(3.6) Patientstakingcorticosteroids:n(%) 49(87.5) PatientstakingsyntheticDMARDs:n
(%)
43(76.8)
Methotrexate:n(%) 15(26.8)
Leflunomide:n(%) 5(8.9)
Hydroxychloroquine:n(%) 3(5.4)
Methotrexate/leflunomide:n(%) 9(16.1) Methotrexate/hydroxychloroquine:n
(%)
9(16.1)
Methotrexate/hydroxychloroquine/sulfasalazine: n(%)
1(1.8)
Cyclosporin:n(%) 1(1.8)
PatientsonbiologicalDMARDs:n(%) 11(19.6)
Adalimumab:n(%) 4(7.1)
Etanercept:n(%) 2(3.6)
Infliximab:n(%) 3(5.4)
Tocilizumab:n(%) 2(3.6)
PatientswithoutDMARDs:n(%) 2(3.6)
CDAI:Median:(IqR) 14.7(5.4–25.0)
Remission(≤2.8):n(%) 8(14.3)
Remissionandlowactivity(≤10):n (%)
23(41)
Moderateactivity(>10≤22):n(%) 17(30.4)
Highactivity(>22):n(%) 16(28.6)
HAQ:Median(IqR) 1.06(0.28–1.75)
Normal(=0):n(%) 9(16.1)
Mildtomoderatedifficulty(>0and
≤1):n(%)
19(33.9)
Moderatetoseveredifficulty(>1and
≤2):n(%)
18(32.1)
Severetoveryseveredifficulty(>2and
≤3):n(%)
10(17.9)
SharpvanderHeijdea
Total:Median(IqR) 2(0–8) Erosion:Median(IqR) 1(0–6) JointSpaceNarrow:Median(IqR) 1(0–5.5)
RAMRISb
Total:Median(IqR) 15(7–35) Erosion:Median(IqR) 8(1–19) Boneedema:Median(IqR) 6(2–14) Synovitis:Median(IqR) 4(2–6)
n,numberofpatientswithrheumatoidarthritis;IqR, interquar-tile range; anti-CCP, anti-cyclic citrullinated peptide antibody; CDAI,clinicalindexofdiseaseactivity;HAQ,HealthAssessment Questionnaire;RAMRIS,RheumatoidArthritisMagneticResonance ImageScoring;DMARDsDiseasemodifyingantirheumaticdrugs.
Table2–Associationofanti-CCPwithdiseaseactivityindexes,functionalcapacityandstructuraldamage.
Variables Anti-CCP p-Value
OR(IC95%)
Negative Positive
CDAI,median(IqR) 7.5(4.2–21.4) 16.2(5.7–31.4) p=0.06a
CDAI
Remissionandlowdiseaseactivity,n(%) 11(47.8) 12(52.2) p=0.09b Moderateandhighdiseaseactivity,n(%) 8(24.2) 25(75.8) OR=2.7(0.9–9.0)
HAQ,median(IqR) 1(0.25–1.50) 1.13(0.31–2.00) p=0.49a
SharpvanderHeijde
Total:Median(IqR) 1(0–7) 3.5(0–8) p=0.29a
Erosion:Median(IqR) 1(0–4) 2(0–6.7) p=0.31a
JointSpaceNarrow:Median(IqR) 1(0–4) 1(0–2.7) p=0.39a
RAMRIS
Total:Median(IqR) 14(8.5–30.5) 23(6.7–42.0) p=0.55a
Erosion:Median(IqR) 8(2–15) 10(1–22.2) p=0.50a
Boneedema:Median(IqR) 5(2–12.5) 8(2.7–16) p=0.37a
Synovitis:Median(IqR) 3(1.5–5.5) 4(3–7.2) p=0.20a
n,numberofpatients;anti-CCP,anti-cycliccitrullinatedpeptideantibody;CDAI,clinicalindexofdiseaseactivity;HAQ,HealthAssessment Questionnaire;RAMRIS,RheumatoidArthritisMagneticResonanceImageScoring.
a Mann–WhitneyUtest. b Chi-squaredtest.
patientspositiveforanti-CCP,butthisratiowasnotsignificant (p=0.06).Moreover,thepresenceofanegativeanti-CCPwas notassociatedwiththeoccurrenceofremissionorastateof lowdiseaseactivity(OR=2.9;95%CI,0.9–9;p=0.09).HAQ,SvdH (total,erosion,jointspacenarrowing)andRAMRIS(total, ero-sion,boneedema,andsynovitis)scoreswerenotassociated withthepresenceofanti-CCP.
In search of a multivariate model to explain anti-CCP variable,alogisticregression modelwasadjusted. All vari-ablescorrelatingwithanti-CCPwithp<0.20(gender,timeof diagnosis,smoking,rheumatoidfactor,extra-articular man-ifestations, rheumatoid nodules, pulmonary involvement, CDAIandHAQ)wereusedintheinitialmodeladjustment.In thefinalmodel,anti-CCPwasrelatedonlywithsmokingand rheumatoidfactor(p<0.05).Themodelindicatedthat smok-ersandformersmokersare5.3timesmorelikelytohavea positiveresultforanti-CCP(95%CI,1.2–22.9)andthosewith positiveRFare4.4timesmorelikelytohaveapositiveresult foranti-CCP(95%CI,1.2–16.6).Thelogisticregressionmodel isshowninTable3.
TheSpearmancorrelationcoefficientbetweenCDAI and image(SvdH and RAMRIS) indexeswas calculated,and no associationamongthesewasfound.Ofthe35patientswho underwentMRI,13wereinremissionorinlow-disease activ-ity(CDAI≤10).Ofthese,12(92.3%)patientshadedemaand12
(92.3%)hadsynovitis,andinonlytwoofthemthesynovitis was>5.0mm(16.6%).RegardingRAMRIS,thefollowing medi-ans (IqR) were obtained: Total index, 21 (11.5–34), erosion score, 9 (3.5–15.1),edema score, 6(3.5 –12.5) and synovitis score, 3 (2.1–5.7). Among the 22 (95.6%) patients showing moderate-to-highactivity,21(95.6%)patientshadedemaand 21 patientshad synovitis.Regarding RAMRIS,thefollowing medians(IqR)wereobtained:Totalindex,13(6–31),erosion score,5(1–17),edemascore,5(2–14)andsynovitisscore,3.5 (2–6).ForallRAMRISindexes,nostatisticallysignificant dif-ferencebetweenpatientsinremissionandwithlowdisease activityversusthoseatmoderate-tohighdiseaseactivitywas observed.
Discussion
Thepresentstudyexaminedthedemographic,clinical, func-tional, and image characteristics ofBrazilian patientswith establishedRA,inordertodeterminetherelationshipof anti-CCPwithseverityofdisease.
Inthestudypopulation,anti-CCPpositivityreached66.1%, a rate similar to that found by Silva et al.18 for Brazilian
patients withestablishedRA.RF positivitywas55.4%.This lowprevalencecanbeexplainedbythefluctuationofantibody
Table3–Multivariatelogisticregressionwithrespecttoanti-CCP.
Variables Beta Standarderror OR CI95%OR p-Value
Smoking 1.7 0.7 5.3 (1.2–22.9) 0.027
levelsduringthecourseofdiseaseinresponsetotreatment,19
orduetothestudydesign,inwhichtheinformationonRF positivitywasbasedonmedicalrecorddata.Itisknownthat anti-CCPand RFtestsarerelated. Studieshaveshownthat mostpatientswithRAandwithapositiveresultforRFare alsopositive foranti-CCP.3,19 Thus,our study isconsistent
withtheliterature.
SmokingisthemainenvironmentalprocessrelatedtoRA, mainlyinHLA-DRB1-positivepatients,andthecitrullination isinduced bytobaccosubstances-the potential pathophy-siologicalmechanismofthisprocess.37Thisstudyshoweda
significantassociationbetweensmokingandanti-CCP posi-tivity.ThisresultisinagreementwiththatfoundbyPedersen etal.,38,39whosestudyevaluatedvariousenvironmentalrisks
associatedwithanti-CCPandHLA-DRB1,andwiththe find-ings of Goeldner et al.,40 who studied the association of
smokingwithanti-CCPinBrazilianpatientswithestablished RA.
The assessment of disease activity in our study was carried out by CDAI, which correlates well with the other assessmentindexes.29,33,41Ourresultsshowedthat
anti-CCP-positivepatients hada medianvalueofCDAI greater than anti-CCP-negativepatients,butwithmarginalstatistical sig-nificance(p=0.06).Ourresultsareinagreementwiththoseof Choeetal.,29whoevaluatedtheassociationofanti-CCPlevels
withDAS28,SDAIandCDAIactivityindexesinpatientswith establishedRA,withnosignificantassociation.
Sincethe remission or low disease activity stateis the maintherapeutictarget,42 weopted also byananalysis of
anti-CCP associationwiththe occurrenceofremission and low disease activity. Our results showed that an anti-CCP negativeresult was not associated with the occurrence of remissionandlowdiseaseactivity(p=0.08).Motaetal.,30who
evaluatedBrazilianpatientswithearlyRA,foundno relation-shipbetweennegativefindingsforanti-CCPandremissionby DAS28.
InprospectivestudiesonearlyRA,Kastbometal.24 and
Rönnelidetal.10 foundanassociationofanti-CCPwithESR
andCRPlevelsandwithDAS28.Ontheotherhand,Nelletal.9
noticedaworsetherapeuticresponseinDAS28in seroposi-tivepatientsafter5and10yearsoffollow-up;nevertheless, thisresultdidnotachieve statisticalsignificance.In estab-lishedRA,disease activity relates irregularlywithanti-CCP positivity.19,20,23
Our study found no association between anti-CCP and HAQ. Functional disability in early RA, assessed by HAQ, seemsnottobeassociatedwiththepresenceofanti-CCP.24,26
The same result has been reported in established RA.19,23
In their evaluation of the association of anti-CCP with a Japanese version of HAQ, Shidara et al.28 found a
signifi-cantassociation;butthehigherdegreeofdisabilityresulting froma20-yearmeandurationofdiseasechallengesan inde-pendent association between the antibody and functional outcomesofRA.InBrazil,Silvaetal.18studied100patients
with established RA, with a mean of eight years of dis-ease.Theseauthorsfoundanassociationbetweenanti-CCP andHAQ,whileMotaetal.,26intheircross-sectionalstudy
evaluating65patientswithearlyRA,foundnosuch associa-tion.
Radiographicanalysisisconsideredoneofthemore objec-tive methods to assess severity of RA. The SvdH method, althoughthemostdetailedanddifficulttoimplement,is con-sideredthemostsensitiveandaccuratetoolinthedetection ofsmallchanges overtime.43 Althoughtheliteratureshow
anassociationbetweenthepresenceofanti-CCPand struc-tural damagemeasured byCR in earlyRA,3–15 in the case
ofestablishedRAtheresultswerenotasconclusive.15–23 It
is noteworthy that most of these studies used the Larsen orSharpmethodintheirradiographicevaluation.Håfström etal.,44inaprospectivestudyexaminingtheroleofRFand
anti-CCPbasedontheradiologicalprogressionwiththeuse oftheSvdHmethodinpatientswithearlyRA,accordingto prednisoloneuse,foundthatRFandanti-CCPwerepredictors ofradiographicprogressiononlyinpatientswhodidnotuse steroids.Ourworkalsodidnotestablishanassociationof anti-CCP withstructuraldamage,asassessedbySvdHin estab-lishedRAcases,whichisinaccordancewithHåfströmetal.’s study,since87.5%ofourpatientswerestillbeingmedicated with prednisone.On the other hand,Gandjbakhchet al.,45
inaprospectivestudy whichanalyzedthe factorsinvolved withradiographicprogression(SvdH)inagroupofpatients inremissionandshowinglowdiseaseactivity,alsofoundno significantassociationbetweenanti-CCPandstructural dam-age. Themean structuraldamageindexinoursamplewas muchlower,whencomparedtootherstudiesinpatientswith establishedRAwiththeuseofSvdHmethod.19,21 This
sug-geststhatoursampleconsistedofpatientswithlesssevere anderosivediseaseand/orwithagoodresponsetotherapeutic intervention.
Tothebestofourknowledge,thisstudyisthefirstto exam-inetheassociationofanti-CCPwithstructuraldamageinRA asmeasuredbyMRI.Ourresultsshowednostatistically signif-icantdifferencesintheparametersevaluatedbyMRIamong anti-CCPpositiveandnegativepatients.Incomparisonwith otherstudies,46,47wefoundlowervaluesfortheRAMRISscore
forsynovitis,boneedemaanderosion,indicatingonceagain thatoursamplewascomposedofamajorityofindividuals withamilderandlesserosivedisease.Itisnoteworthythat theuseofMRIformonitoringtreatmentwithbiologicalagents canselecthighdiseaseactivitypatients.
Patients in remission and showing low disease activity can, inspiteofclinical control,exhibitsigns ofactivity on MRI,48,49 and thesechangesmay determineafuture
radio-graphicprogression.50Theresultsofthisstudyindicatedno
associationbetweendiseaseactivityandRAMRISscores.On theotherhand,92.1%ofourpatientswhowereinremissionor inlowdiseaseactivityshowedsignsofinflammation(edema and synovitis) on MRI, although onlytwo of them (16.6%) hadasynovitis>5mm.AccordingtoGandjbakhchetal.,45in
Inconclusion,inthesampleinvestigatedtheresultsdidnot establishanassociationofanti-CCPwithdiseaseseverity.The presenceofconfoundingvariables,suchasanearlydiagnosis andanappropriateresponsetotherapeuticintervention, con-tributedtosettingupagroupofpatientswithlesssevereand slightlyerosivedisease.Itisbelievedthatthewayofselecting participantsinourstudy(onlyindividualsunder10yearsof diseasedurationandwithoutdifficultytomeettheresearch protocolwereaccepted)mayalsohavelimitedtheexposure oftheentireuniverseofRA.Nonetheless,thisresultallows ustoquestionifanti-CCPwouldhavelessinfluenceon prog-nosisforpatientswithamorefavorablediseaseprofile.On theotherhand,duetothesmallsamplesize,thisstudymay havefailedtodetectthemostsignificantdifferences. There-fore,itisbelievedthattheevaluationofalargernumberof individuals,possiblywithamulticentricdistributionin long-termprospectiveobservationalstudiesand,ifpossible,with greatercontrolofconfoundingvariables,couldcontributeto theultimateresolutionofthisissue.Todate,wecannot sup-porttheindicationforanti-CCPdeterminationasaprognostic toolinestablishedRA.
Funding
Roche(apharmaceuticalcompany)donatedanti-CCPkits.The ECOARimageinstitutedonatedmagneticresonances.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
WethankDr.RenatoRezendeAlvarengaforhisfundamental contributionandDr.PauloMadureiradePaduaforhissupport andcontribution.
r
e
f
e
r
e
n
c
e
s
1. MotaLM,CruzBA,BrenolCV,PereiraIA,FronzaLS,Bertolo MB,etal.ConsensusoftheBrazilianSocietyofRheumatology fordiagnosisandearlyassessmentofrheumatoidarthritis. RevBrasReumatol.2011;51:199–219.
2. MarkatseliTE,PapagorasC,DrososAA.Prognosticfactorsfor erosiverheumatoidarthritis.ClinExpRheumatol.
2010;28:114–23.
3. KrootEJ,deJongBA,vanLeeuwenMA,SwinkelsH,vanden HoogenFH,van’tHofM,etal.Theprognosticvalueof anti-cycliccitrullinatedpeptideantibodyinpatientswith recent-onsetrheumatoidarthritis.ArthritisRheum. 2000;43:1831–5.
4. VencovskyJ,MachacekS,SedovaL,KafkovaJ,GatterovaJ, PesakovaV,etal.Autoantibodiescanbeprognosticmarkers ofanerosivediseaseinearlyrheumatoidarthritis.Ann RheumDis.2003;62:427–30.
5. MeyerO,LabarreC,DoudadosM,GoupilleP,CantagrelA, DuboisA,etal.Anticitrullinatedprotein/peptideantibody assaysinearlyrheumatoidarthritisforpredictingfiveyear
radiographicdamage.AnnRheumDis.2003;62: 120–6.
6.BongiSM,ManettiR,MelchiorreD,TurchiniS,BoccacciniP, VanniL,etal.Anti-cycliccitrullinatedpeptideantibodiesare highlyassociatedwithseverebonelesionsinrheumatoid arthritisanti-CCPandbonedamageinRA.Autoimmunity. 2004;37:495–501.
7.ForslindK,AhlménM,EberhardtK,HafströmI,SvenssonB. Predictionofradiologicaloutcomeinearlyrheumatoid arthritisinclinicalpractice:roleofantibodiestocitrullinated peptides(anti-CCP).AnnRheumDis.2004;63:1090–5.
8.QuinnMA,GoughAK,GreenMJ,DevlinJ,HensorEM, GreensteinA,etal.Anti-CCPantibodiesmeasuredatdisease onsethelpidentifyseronegativerheumatoidarthritisand predictradiologicalandfunctionaloutcome.Rheumatology. 2006;45:478–80.
9.NellVP,MacholdKP,StammTA,EberlG,HeinzlH,Uffmann M,etal.Autoantibodyprofilingasearlydiagnosticand prognostictoolforrheumatoidarthritis.AnnRheumDis. 2005;64:1731–6.
10.RonnelidJ,WickMC,LampaJ,LindbladS,NordmarkB, KlareskogL,etal.Longitudinalanalysisofcitrullinated protein/peptideantibodies(anti-CP)during5yearfollowup inearlyrheumatoidarthritis:anti-CPstatuspredictsworse diseaseactivityandgreaterradiologicalprogression.Ann RheumDis.2005;64:1744–9.
11.LindqvistE,EberhardtK,BendtzenK,HeinegardD,SaxneT. Prognosticlaboratorymarkersofjointdamageinrheumatoid arthritis.AnnRheumDis.2005;64:196–201.
12.SanmartiR,Gomez-CentenoA,ErcillaG,LarrosaM,VinasO, VazquezI,etal.Prognosticfactorsofradiographic
progressioninearlyrheumatoidarthritis:atwoyear prospectivestudyafterastructuredtherapeuticstrategy usingDMARDsandverylowdosesofglucocorticoids.Clin Rheumatol.2007;26:1111–8.
13.KaltenhauserS,PiererM,ArnoldS,KampradM,BaerwaldC, HantzschelH,etal.Antibodiesagainstcycliccitrullinated peptideareassociatedwiththeDRB1sharedepitopeand predictjointerosioninrheumatoidarthritis.Rheumatology. 2007;46:100–4.
14.HetlandML,PedersenKS,JunkerP,OstergaardM,EjbjergBJ, JacobsenS,etal.Radigraphicprogressionandremissionrates inearlyrheumatoidarthritis–MRIboneoedemaand anti-CCPpredictedradiographicprogressioninthe5-year extensionofthedouble-blindrandomisedCimestratrial.Ann RheumDis.2010;69:1789–95.
15.KimHH,KimJ,ParkS,KimS,KimO,ChoeJ.Correlationof anti-cycliccitrullinatedantibodywithhandjointerosion scoreinrheumatoidarthritispatients.KoreanJInternMed. 2010;25:201–6.
16.RyckeL,PeeneI,HoffmanIE,KruithofE,UnionA,MeheusL. Rheumatoidfactorandanticitrullinatedproteinantibodiesin rheumatoidarthritis:diagnosticvalue,associationswith radiologicalprogressionrate,andextra-articular manifestations.AnnRheumDis.2004;63:1587–93.
17.MewarD,CooteA,MooreDJ,MarinouI,KeyworthJ,Dickson MC,etal.Independentassociationsofanti-cyclic
citrullinatedpeptideantibodiesandrheumatoidefactorwith radiographicseverityofrheumatoidarthritis.ArthritisRes Ther.2006;8:R128.
18.SilvaAFMAN,LimaAMS,LimaEF,CorreaMI,CarvalhoEM. Associationofanti-cycliccitrullinatedpeptideantibodyand severerheumatoidarthritis.RevBras.Reumatol.
2006;46:165–73.
20.AlexiouI,GermenisA,ZiogasA,TheodoridouK,SakkasLI. Diagnosticvalueofanti-cycliccitrullinatedpeptide antibodiesinGreekpatientswithrheumatoidarthritis.BMC MusculoskeletDis.2007;8:37.
21.SyversenSW,GaarderPI,GollGL,OdegardS,Haavardsholm EA,MowinckelP,etal.Highanti-cycliccitrullinatedpeptide levelsandanalgorithmoffourvariablespredictradiographic progressioninpatientswithrheumatoidarthritis:results froma10-yearlongitudinalstudy.AnnRheumDis. 2008;67(2):212–7.
22.Nieto-ColoniaAM,SantosWS,KeusseyanSP,CaldanaW, FernandesAR,AndradeLE.Antibodiestocitrullinated peptidesarenotassociatedwiththerateofjointdestruction inpatientswithawell-establisheddiagnosisofrheumatoid arthritis.BrazJMedBiolRes.2008;41:188–92.
23.GuptaR,ThabahMM,AnejaR,KumarA,VargheseT, ChandrasenanPJ.Usefulnessofanti-CCPantibodiesin rheumaticdiseasesinIndianpatients.IndianJMedSci. 2009;63:92–100.
24.KastbomA,StrandbergG,LindroosA,SkoghT.Anti-CCP antibodytestpredictsthediseasecourseduring3yearsin earlyrheumatoidarthritis(theSwedishTIRAproject).Ann RheumDis.2004;63:1085–9.
25.KorkmazC,UsT,KasifogluT,AkgünY.Anti-cyclic citrullinatedpeptide(CCP)antibodiesinpatientswith long-standingrheumatoidarthritisandtheirrelationship withextra-articularmanifestations.ClinBiochem. 2006;39:61–5.
26.MotaLM,NetoLS,BurlingameRW,MénardHA,PereiraIA, CarvalhoJF,etal.Disabilityandquality-of-lifearenot influencedbytheprevalenceofautoantibodiesinearly rheumatoidarthritispatients–resultsoftheBrasíliaCohort. RevBrasReumatol.2012;52:819–29.
27.LiHH,SongW,LiY,LiuY,BaiJ,LiX,etal.Diagnosticvalueof anti-cycliccitrullinatedpeptideantibodiesinnorthern ChineseHanpatientswithrheumatoidarthritisandits correlationwithdiseaseactivity.ClinRheumatol. 2010;29:413–7.
28.ShidaraK,InoueE,HoshiD,SatoE,NakajimaA,MomoharaS, etal.Anti-cycliccitrullinatedpeptideantibodypredicts functionaldisabilityinpatientswithrheumatoidarthritisin alargeprospectiveobservationalcohortinJapan.Rheumatol Int.2012;32:361–6.
29.ChoeJY,BaeJ,LeeH,BaeSC,KimSK.Relationofrheumatoid fatorandanti-cycliccitrullinatedpeptideantibodywith diseaseactivityinrheumatoidarthritis:cross-sectionalstudy. RheumatolInt.2013;33:2373–9.
30.MotaLM,NetoLL,deCarvalhoJF,PereiraIA,BurlingameR, MénardHA,etal.Thepresenceofanti-citrullinatedprotein antibodies(ACPA)andrheumatoidfactoronpatientswith rheumatoidarthritis(RA)doesnotinterferewiththechance ofclinicalremissioninfolow-upof3years.RheumatolInt. 2012;32:3807–12.
31.ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
32.AletahaD,NeogiT,SilmanAJ,FunovitsJ,FelsonDT,Bingham CO3rd,etal.2010rheumatoidarthritisclassificationcriteria: anAmericanCollegeofRheumatology/EuropeanLeague AgainstRheumatismcollaborativeinitiative.AnnRheumDis. 2010;69:1580–8.
33.AletahaD,NellVP,StammT,UffmannM,PflugbeilS,Machold K,etal.Acutephasereactantsaddlittletocompositedisease activityindicesforrheumatoidarthritis:validationofa clinicalactivityscore.ArthritisResTher.2005;7:R796–806.
34.FerrazMB,OliveiraLM,AraujoPM,AtraE,TugwellP. Crossculturalreliabilityofthephysicalabilitydimensionof
thehealthassessmentquestionnaire.JRheumatol. 1990;17:813–7.
35.VanderHeijdeD.Howtoreadradiographicsaccordingtothe Sharp/vanderHeijdemethod.JRheumatol.1999;26:743–5.
36.OstergaardM,PeterfyC,ConaghanP,McQueenF,BirdP, EjbjergB,etal.Omeractrheumatoidarthritismagnetic resonanceimagingstudies.CoresetofMRIacquisitions,joint pathologydefinitions,andtheOmeractRA-MRIscoring system.JRheumatol.2003;30:1385–6.
37.KlareskogL,StoltP,LundbergK,KallbergH,BengtssonC, GrunewaldJ,etal.Anewmodelforanetiologyofrheumatoid arthritis:smokingmaytriggerHLA-DR(shared
epitope)-restrictedimmunereactionstoautoantigens modifiedbycitrullination.ArthritisRheum.2006;54:38–46.
38.PedersenM,JacobsenS,GarredP,MadsenHO,KlarlundM, SvejgaardA,etal.Strongcombinedgene-environmenteffects inanti-cycliccitrullinatedpeptide-positiverheumatoid arthritis.ArthritisRheum.2007;56:1446–53.
39.PedersenM,JacobsenS,KlarlundM,PedersenBV,WiikA, WohlfahrtJ,etal.Environmentalriskfactorsdifferbetween rheumatoidarthritiswithandwithoutautoantibodiesagainst cycliccitrullinatedpeptides.ArthritisResTher.2006;8:R133.
40.GoeldnerI,SkareTL,ReasonIT,NisiharaRM,SilvaMB, UtiyamaSR.Associationofanticycliccitrullinatedpeptide antibodieswithextra-articularmanifestations,gender,and tabagisminrheumatoidarthritispatientsfromsouthern Brazil.ClinRheumatol.2011;30:975–80.
41.AletahaD,NellVP,StammT,UffmannM,PflugbeilS,Machold K,etal.TheSimplifiedDiseaseActivityIndex(SDAI)andthe ClinicalDiseaseActivityIndex(CDAI):areviewoftheir usefulnessandvalidityinrheumatoidarthritis.ClinExp Rheumatol.2005;23Suppl.39:S100–8.
42.SmolenJS,LandewéR,BreedveldFC,BuchM,BurmesterG, DougadosM,etal.EULARrecommendationsforthe managementofrheumatoidarthritiswithsyntheticand biologicaldisease-modifyingantirheumaticdrugs:2013 update.AnnRheumDis.2014;73:492–509.
43.RavindranV,RachapalliS.Anoverviewofcommonlyused radiographicscoringmethodsinrheumatoidarthritisclinical trials.ClinRheumatol.2011;30:1–6.
44.HafströmI,EngrealI-L,RönnelidJ,BoonenA,VanderHeijde D,SvenssonB.Rheumatoidfactorandanti-CCPdonot predictprogressivejointdamageinpatientswithearly rheumatoidarthritistreatedwithprednisolone:a randomisedstudy.BMJOpen.2014;4:e005246,
http://dx.doi.org/10.1136/bmjopen-2014-005246.
45.GandjbakhchF,HaavardsholmEA,ConaghanPG,EjbjergB, FoltsV,BrownAK,etal.Determiningamagneticresonance imaginginflamatoryactivityaccptablestatewithout subsequentradiographicprogressioninrheumatoidarthritis: resultsfromafollowupMRIstudyof254patientsinclinical remissionorlowdiseaseactivity.JRheumatol.
2014;41:398–406.
46.ConaghanPG,EmeryP,OstergaardM,KeystoneEC,Genovese MC,HsiaEC,etal.AssessmentbyMRIofinflammatioand damageinrheumatoidarthritispatientswithmethotrexat inadequateresponsereceivinggolimumabe:resultsofthego forwardtrial.AnnRheumDis.2011;70:1968–74.
47.OstergaardM,EmeryP,ConaghanG,FleischmannR,HsiaEC, XuWeichun,etal.Significantimprovementinsynovitis, osteitis,andboneerosionfollowinggolimumaband methotrexatecombinationtherapyascomparedwith methotrexatealone.ArthritisRheum.2011;63:712–22.
49.BrownAK,QuinnMA,KarimZ,ConaghanPG,PeterfyCG, HensorE,etal.Presenceofsignificantsynovitisin rheumatoidarthritispatientswithdisease-modifying antirheumaticdrug-inducedclinicalremission.Arthritis Rheum.2006;54:3761–73.