RevBrasAnestesiol.2017;67(4):439---441
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
LETTERS
TO
THE
EDITOR
Sedation
with
dexmedetomidine
on
Klippel
Feil
Syndrome
infant
patient
Sedac
¸ão
com
dexmedetomidina
em
paciente
pediátrico
com
síndrome
de
Klippel-Feil
DearEditor,
Klippel Feil Syndrome (KFS) is a congenital malformation whichhasa failureofsegmantationof cervicalsomitesin the8thweeksofgestationandfusionatleasttwocervical segments.1 It is described asthe triadof short neck,low
posterior hairline and decreased range of neck motions.2
Especiallydecreasedrangeofneckmotionsleadmany anes-thesiologists todifficult airway management. Dexmedeto-midine is usedfor sedation especiallywithout respiratory depression and for use in very early age group pediatric patientswasnotobservedinreportedcases.3Inthiscase;
weaimedtopresentsuccessfulsedationby dexmedetomi-dinetoinfantpatientwhois65daysaged,diagnosedKFS, limitedneckmotionsandknowndifficultairway.
Infantpatient,whois 65daysaged,4kgweight,81cm height anddiagnosed KFS, wasscheduled for a neck MRI. On evaluation of patient; short neck, low posterior hair-line, thorax deformity and floatingfinger wasfound. The mouth opening of patient was normal but the extension of neck wasparticularly restricted. Systemicexamination revealed no other abnormalities. The chest X-ray showed hypoplastic ribs. In medical history of patient; therewas
180 171
96
25
Begining Preop 5. min (bolus)
Preop 10. min (bolus)
Op 1. min (inf)
Op 5. min (inf)
Op 10. min (inf)
Op 15. min (inf)
Op 20. min (inf)
Postop 5. min
Postop 10. min
Postop 15. min
25 23 25 25 26 24 25 30 30 31
99 99 99 99 99 99 98 99 98 99
146
130 132 132 133 130 130 137 141
145 160
140
120
100
80
60
40
20
02 saturation Heart rate Respiration rate
0
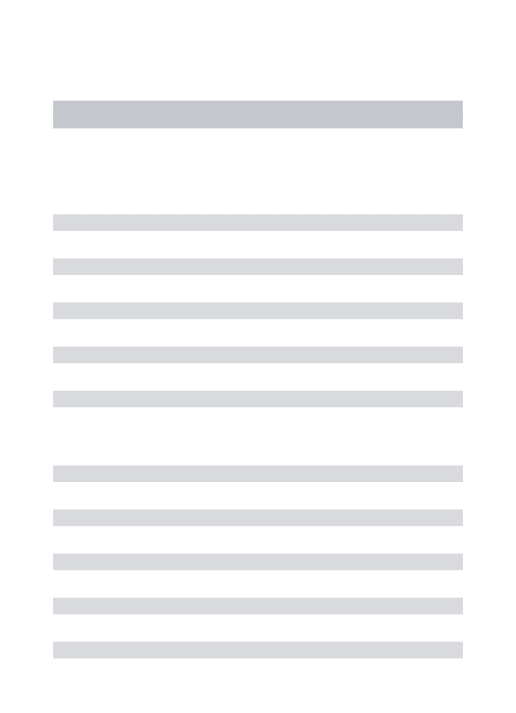
Figure1 Monitorizationdata.
intermittent respiratory distress. The patient was taken totheanesthetic preparationroom. Standard monitoriza-tion (electrocardiography, heart rate, oxygen saturation) were performed and intravenous (IV) line was obtained. After preoxygenation for 5min by facemask, dexmedeto-midine infusion was administeredby IVroute asbolus of 0.5mcg.kg−1dosefor10min.Monitorizationdataand Ram-seySedationScoreofthepatientwererecordedatintervals of 5min. Ear plugs was inserted into patient for protec-tionofloudsoundsinMRIroom.Afterbolusadministration, dexmedetomidineinfusionwascontinuedformaintenance dose as 0.6mg.kg−1.h−1. Dexmedetomidine infusion was continuedfor20min throughout theprocedure.Mean val-ues of monitoring data of the patient were recorded as peripheraloxygensaturation:98%(range96---99),heartrate: 138beats/min (range 130---171), respiratory rate: 26/min (range23---30)(Fig.1).Duringtheprocess,RamseySedation Scorewasfound 4. Dexmedetomidine infusion was termi-natedat the end of operation and patient follow-up was continuedinthepostanesthesiacareunit.Patientwassent toserviceafterthefullawakenessandthepatientwas dis-chargedonthesameday.
There wasnoneed an application suchas mask venti-lation,laryngoscopy,intubationandlaryngeal maskinthis casewithdifficultairway. Ithasbeen reportedthe useof dexmedetomidine has provide adequate sedation without respiratorydepression.4
440 LETTERSTOTHEEDITOR
motionsanddifficult airway. We believethat dexmedeto-midineis anagent maybepreferredan alternativeagent ensuring respiratory control in anesthesia procedures for sedation.
Conflicts
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Manivel S, Prasad R, Jacob R. Anesthetic management of a childwithKlippel-Feilsyndromeintheradiologysuite.Paediatr Anaesth.2005;15:171---2.
2.CakmakkayaOS,Kaya G,AltintasF,et al.Anesthetic manage-mentofachildwithArnold-ChiarimalformationandKlippel-Feil syndrome.PaediatrAnaesth.2006;16:355---6.
3.Subramanyam R, Cudilo EM, Hossain MM, et al. To pretreat ornottopretreat: prophylacticanticholinergicadministration before dexmedetomidine in pediatric imaging. Anesth Analg. 2015;121:479---85.
4.ShahTH,BadveMS,OlajideKO,etal.Dexmedetomidineforan awake fiber-optic intubation of a parturient withKlippel-Feil syndrome.Type I Arnold Chiari malformation and status post releasedtethered spinal cord presenting for repeat cesarean section.ClinPract.2011;1:57.
AhmetSelimOzkan∗,SedatAkbas,MehmetAliErdogan,
RamazanKırteke,MahmutDurmus
TurgutOzalMedicineCenter,DepartmentofAnesthesia, Malatya,Turkey
∗Correspondingauthor.
E-mail:[email protected](A.S.Ozkan). Availableonline10May2016
http://dx.doi.org/10.1016/j.bjane.2016.02.001
0104-0014/
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Cardiac
arrest
animal
model:
a
simple
device
for
small
animals’
chest
compression
Modelo
animal
de
parada
cardíaca:
um
dispositivo
simples
para
a
compressão
torácica
em
pequenos
animais
DearEditor,
Basedon the poor outcome of Cardiac Arrest(CA), many animal models have been proposed to better understand thepathophysiologyofthisevent.Animalmodelshavealso been used to understand the effects of Cardiopulmonary Resuscitation(CPR)inpatientswithCA.However, develop-mentofCAmodelsisdifficult,especiallywhendealingwith smallanimals.Smallanimalsaremoreeconomiccompared tolarge animal, but they have far more complex instru-mentation,poorsurvival,monitoring difficultiesandsome specificpurposesdevicesarenotavailable.
Oneofthemaindifficulties,especiallywhendealingwith CAforsmallanimals,isthechestcompression.Mostofthe studiesuseeithermanualor expensivedesignedmachines for chestcompressions.1,2 The main problemwithmanual
chest compression is the lack of consistency of the CPR, resultingindifferencesofthechestcompression(i.e.depth andfrequency),fatigueoftheCPRperformer,andpossible internalorgandamagefromovercompression.Thus,theuse ofamechanicaldeviceishighlydesirablefor agreat con-sistency.However,thereisnotamachineavailablethatis designedforthispurpose,thenadaptationsordevelopment ofnewmachinesarenecessary.Gazmurietal.developeda custom-madepneumaticchestcompressionthatallowsfor frequency and depth regulation.1 The main problem with
this machine is the price, as it needs to be customized parts.
One solution that our lab has adopted recently was the use of a modified sewing machine that was able to provide mechanical chestcompression withlow cost.The machinehadallsewing-relatedpartsremoved(throatplate, bobbinhousing,looptakerandbedshafts)andaspeed con-trollersubstitutedthepedal(Fig.1).Thepresserfootwas removed andthe needlebarwascut. A smallpistol head was fitterto the needlebar in orderto adequately com-press the heart. These modifications allowed good chest compressionandratecontrol.Byremovingthebobbin hous-ing,the animal couldbefittedunder thepistonfor chest compression. The depth of the chest compression could be adjusted by the height of table which the animal is laying.
In order to test the machine, seven male Wistar rats (300g) weresubmittedto femoralarteryand right exter-nal jugularvein cannulation. After cannulation, the right ventricle was stimulated with 1mA at 60Hz to induce and ventricular fibrillation. The stimulation was kept for 3minutesinordertopreventspontaneousdefibrillation.The CAwasalsonotedbytheabsenceofarterialbloodpressure onthemonitor.AfterfiveminutesofCA,themachinewas turnedontoarateof200chestcompressionsperminute, adoseof20mcg/kgofepinephrinewasinjectedanda dia-stolicbloodpressuregreaterthan20mmHgwasaimed.The chest compressionsdepth wascalculatedtomaintain one third of the antero-posterior chest diameter. In order to minimizepossible intrathoracicorganlesion,thedepth of chestcompressionwaskepttolessthan17mm.1Withthree