www.jped.com.br
ORIGINAL
ARTICLE
Validation
of
a
subjective
global
assessment
questionnaire
夽
,
夽夽
Maiara
Pires
Carniel
a,∗,
Daniele
Santetti
a,
Juliana
Silveira
Andrade
a,
Bianca
Penteado
Favero
b,
Tábata
Moschen
c,
Paola
Almeida
Campos
d,
Helena
Ayako
Sueno
Goldani
e,
Cristina
Toscani
Leal
Dornelles
aaUniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
bPontifíciaUniversidadeCatólicadoRioGrandedoSul(PUCRS),PortoAlegre,RS,Brazil
cCentroUniversitárioLaSalle(UNILASALLE),Canoas,RS,Brazil
dCentroUniversitárioFranciscano(UNIFRA),SantaMaria,RS,Brazil
eDepartmentofPediatrics,UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
Received23October2014;accepted11March2015 Availableonline17July2015
KEYWORDS Nutritional assessment; Children; Adolescents; Anthropometry; Validationstudies
Abstract
Objective: TovalidatetheSubjectiveGlobalNutritionalAssessment(SGNA)questionnairefor Brazilianchildrenandadolescents.
Methods: Across-sectionalstudywith242patients,aged30daysto13years,treatedin pedi-atricunitsofatertiaryhospitalwithacuteillnessandminimumhospitalizationof24h.After permissionfromtheauthorsoftheoriginalstudy,thefollowingcriteriawereobservedtoobtain thevalidationofSGNAinstruments:translationandbacktranslation,concurrentvalidity, pre-dictivevalidity,andinter-observerreliability.Thevariablesstudiedwereage,sex,weightand lengthatbirth,prematurity,andanthropometry(weight,height,bodymassindex,upperarm circumference,tricepsskinfold,andsubscapularskinfold).Theprimaryoutcomewas consid-eredastheneedforadmission/readmissionwithin30daysafterhospitaldischarge.Statistical testsusedincludedANOVA,Kruskal---Wallis,Mann---Whitney,chi-square,andKappacoefficient.
Results: AccordingtoSGNAscore,80%ofpatientswereconsideredaswellnourished,14.5% moderatelymalnourished,and5.4%severelymalnourished.Concurrentvalidityshowedaweak correlationbetweentheSGNAandanthropometricmeasurements(p<0.001).Regarding pre-dictivepower,themainoutcomeassociatedwithSGNAwaslengthofadmission/readmission.
夽 Pleasecitethisarticleas:CarnielMP,SantettiD,AndradeJS,FaveroBP,MoschenT,CamposPA,etal.Validationofasubjectiveglobal
assessmentquestionnaire.JPediatr(RioJ).2015;91:596---602.
夽夽
ThestudywasconductedatPostgraduatePrograminChildandAdolescentHealth,UniversidadeFederaldoRioGrandedoSul(UFRGS), PortoAlegre,RS,Brazil.
∗Correspondingauthor.
E-mail:[email protected](M.P.Carniel). http://dx.doi.org/10.1016/j.jped.2015.03.005
Secondaryoutcomesassociatedincludedthefollowing:lengthofstayattheunitafterSGNA, weight andlengthatbirth, andprematurity(p<0.05).The interobserverreliability showed goodagreementamongexaminers(Kappa=0.74).
Conclusion: This study validated the SGNA in thisgroup of hospitalizedpediatric patients, ensuringitsuseintheclinicalsettingandforresearchpurposesintheBrazilianpopulation. ©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Avaliac¸ãonutricional; Crianc¸as;
Adolescentes; Antropometria; Estudosdevalidac¸ão
Validac¸ãodeumquestionáriodeavaliac¸ãonutricionalsubjetivaglobal
Resumo
Objetivo: Validar o questionário de Avaliac¸ão Nutricional Subjetiva Global (ANSG) para a populac¸ãodecrianc¸aseadolescentesbrasileiros.
Métodos: Estudotransversal,realizado com242pacientes, de30 diasa13anos, atendidos emunidadespediátricasdeumhospitalterciário,comdoenc¸asagudasetempode permanên-ciamínimade24horashospitalizados.Apósautorizac¸ãodosautoresdoestudooriginalforam realizadasasseguintesetapasparaobtenc¸ãodavalidac¸ãodosinstrumentosdeANSG:traduc¸ão (backtranslation),validadedecritérioconcorrenteepreditivaeconfiabilidadeinterobservador. As variáveis em estudo foram: idade, sexo,peso e comprimentoao nascer, prematuridade e antropometria (peso, estatura, índice de massa corporal, circunferência braquial, dobra cutâneatricipitaledobracutâneasubescapular).Odesfechoprincipalconsideradofoi neces-sidadede internac¸ão/reinternac¸ão até30 diasapósaalta hospitalar.Ostestes estatísticos utilizadosforam:ANOVA,Kruskal---Wallis,Mann---Whitney,Qui-quadradoecoeficienteKappa.
Resultados: Deacordocomaclassificac¸ãodoANSG80%dospacientesforamclassificadoscomo bemnutridos,14.5%moderadamentedesnutridose5.4%gravementedesnutridos.Avalidade concorrente mostrou fraca aregular correlac¸ão do ANSG com as medidas antropométricas utilizadas (p<0.001). Quantoao poderpreditivo, desfechoprincipal associado ao ANSG foi tempodeinternac¸ão/reinternac¸ão.Osdesfechossecundáriosassociadosforam:tempode per-manêncianaunidadeapósANSG,pesoecomprimentoaonascereprematuridade(p<0.05).A confiabilidadeinterobservadormostrouboaconcordânciaentreosavaliadores(Kappa=0.74).
Conclusão: EsteestudovalidouométododeANSGnessaamostradepacientespediátricos hos-pitalizados,possibilitando seuusoparafinsdeaplicac¸ãoclínicaedepesquisanapopulac¸ão brasileira.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Inrecentdecades,therehasbeenasignificantreductionin theprevalenceofworldwidemalnutritioninchildren.1
Nev-ertheless,deathratesduetoseveremalnutritioninchildren
undergoinghospitaltreatmentremainhigh.2---4Several
stud-ieshavereportedaprevalenceofmalnutritionrelatedtoan
underlyingdiseaseof6---51%inhospitalizedchildren.5---7
However, the lack of consensus regarding the
defini-tion,heterogeneousnutritionalscreeningmethods,andthe
fact that nutrition is not prioritized as part of patient
care are some of the factors responsible for the
under-recognition of malnutrition prevalence and its impact on
clinicalresults.Recently,anewdefinitionofhospital
malnu-tritioninchildrenhasbeenused.Thisdefinitionincorporates
theconceptsofchronicity,etiologyandpathogenesisof
mal-nutrition,itsassociationwithinflammation,anditsimpact
onbodyfunctionalalterations.8
Thus, it is crucialtoknow and monitor the nutritional
statusofhospitalizedchildren,tobetterunderstandfactors
contributingtotheoccurrenceofcomplications,increased
lengthofhospitalstay,and consequentincreasein health
systemcosts.5,9---11
Subjective nutritional assessment is an evaluation
method based on clinical judgment and has been widely
used to assess the nutritional status of adults for
clini-calresearchpurposes,7consideredapredictorofmorbidity
andmortality.12Itdiffersfromothernutritionalassessment
methodsbyencompassingnotonlybodycomposition
alter-ations but alsopatient functionalimpairment,13 assessing
thepossiblepresenceofnutritionalrisks,basedonclinical
historyandphysicalexamination.Itisasimple,fast,
inex-pensive,andnon-invasivemethodthatcanbeperformedat
thebedside.12
The questionnaire adapted by Secker andJeejeebhoy7
forthepediatricpopulationhasbeentermedtheSubjective
GlobalNutritionalAssessment(SGNA),andevaluatesthe
fol-lowing parameters:the child’s current height and weight
history,parentalheight,foodconsumption,frequencyand
duration of gastrointestinal symptoms, and current
func-tional capacity and recent alterations. It also associates
Thepresenceoffunctionalalterationsappearstobethe
determiningfactorintheoccurrenceofcomplications
asso-ciatedwithmalnutrition.Thus,itisofutmostimportanceto
attainearlydetectionofnutritionalriskthroughamethod
thatisadequate,sensitivetoidentifyearlyalterations,
spe-cificenoughtobechangedonlybynutritionalimbalances,
andcorrectedbasedonanutritionintervention.14
Considering the need to validate a reliable method of
nutritionalassessmentforchildrenandadolescentsinBrazil,
theaimofthisstudywastovalidatetheSGNAinapopulation
ofBrazilianchildrenandadolescents.
Methods
Population
Thiswasacross-sectionalstudycarriedoutwith242patients aged30daysto13 years,in thecity of PortoAlegre, RS, Southern Brazil. Patients were enrolled in the Pediatric Emergencyand Inpatient Units of Hospital de Clinicas de PortoAlegre,RS,consideringasastudyfactorthenutritional statusassessmentbasedonobjectiveandsubjectivedata. The analyzed outcomes were need for hospitaladmission (patientsfrom theemergency observation room)or read-mission(patientsfromthepediatricward).Datacollection occurredfromMay2012toJune2013.
Thestudyinclusioncriteriawerethefollowing:children and adolescents, aged30 days to 19 years, of both gen-ders,withclinicaldiagnosisofacutediseases15andminimum
lengthofstayof24hinthePediatricEmergencyand
Inpa-tientUnits.
Exclusion criteria were as follows: neuropsychomotor
development delay (according to parental information);
underlying chronic diseases (congenital malformations,
inborn errors of metabolism, heart disease, neuropathy,
liver disease, immunocompromised patients, children of
HIV+mothers);chronicuseofmedicationexceptforferrous
sulfate and multivitamins at prophylactic doses; hospital
admission in the 30-day period prior to the study
assess-ment;patientsyoungerthanonemonth;infectiousprocess
inthepastsevendays;incapacitytoperform
anthropomet-ricmeasurements;andpatientsandcaregiverswhodidnot
speak Portuguese.The clinical informationrelated tothe
underlying diseases were collected from medical records
andconfirmedbytheassistantmedicalteam.
The research project designed for the developmentof
thisstudywasapprovedbytheResearchEthicsCommittee
ofHospitaldeClínicasdePortoAlegre(ProjectNo.11-0339).
Parentsand/orguardianssignedaninformedconsentprior
tostudyenrollment.
Toolvalidationprocess
Initially permission was obtained from the authors to reproduce and use the SGNA questionnaires originating from the PhD thesis entitled ‘‘Nutritional Assessment in Children:AComparisonofClinicalJudgmentandObjective Measures.’’16 Next, the questionnaires were translated
through the back-translation method,17 according to
the following steps: first, translation from English into
Portuguese; subsequently, the new questionnaires were
translatedfromPortuguesebackintoEnglish.
At the third step, a comparison of the tools was
per-formed by a bilingual translator whose native language
is English, who verified whether the new questionnaires
wereaccurateaccordingtotheoriginalcontentand
struc-ture.Thestepsofthistranslationprocesswereperformed
bythreeindependenttranslators.Subsequently,translation
validationwasperformed,consisting ofthereliabilityand
validityassessment.
Studydesign
Afterresearchertrainingtostandardizecollectionof anthro-pometric measurements18 andSGNA questionnaire use,7,19
each child was assessed by two independent researchers
blinded to each other; one researcher collected
anthro-pometric data, whereas the other applied the SGNA
questionnaire. To test SGNA interobserver reproducibility,
61randomlyselectedpatients(25%ofthestudypopulation)
wereevaluatedbyathirdcollaborator,whoalsoappliedthe
SGNAquestionnaire.
Theobjectiveandsubjectivedatawerecollectedwithin
48h after patient hospital admission. Thirty days after
patient hospital discharge, a search was carried out in
the medical files to observe the outcome of need for
hospitaladmission/readmission. Datawere entered intoa
databaseusingMicrosoft Excelsoftware(Microsoft®,2007,
USA) and exported to SPSS (version 18.0, Chicago, USA).
AnthroandAnthroPlussoftware(version3.2.2,WorldHealth
Organization, Geneva, Switzerland) were used to assess
anthropometricdata.
Subjectiveglobalnutritionalassessment
Objectivenutritionalassessment
The following anthropometric measurements were ana-lyzed:weightandheight;bodymassindex(BMI);upperarm circumference (AC); triceps skinfold (TSF), and subscapu-lar skinfold (SSF). For children younger than 24 months, weightwasmeasuredwiththechildrenwearingnoclothes ordiapers.Childrenolderthan24monthsandadolescents wereweighed withagown andwithout shoes. AFilizola® electronicscale(Filizola®,SP,Brazil)wasusedtomeasure weight.
Height measurements were performed using a wood boardwithafixed bladeononesideandmoveableonthe other,thetopoftheheadonthefixedpart(WCS®,Brazil), withthemoveablepartarrangedtobeinparallelwiththe child’slegs.Inchildrenyoungerthan24months,thelength wasmeasured in the supinepositionby measuringwith a rulerattachedtotheboard.Childrenolderthan24months andadolescentsweremeasuredinthestandingpositionwith ananthropometricruler(WISO®,Brazil)fixedonthewalland mobilecursorgraduatedincentimeters.
AC measurementswere measured using a flexible and retractablefiberglassmeasuringtape,surroundingthe mid-dleportionofthenon-dominantarm,withthearmrelaxed. TSFmeasurementswereperformedintheposteriorregion ofthenon-dominantarm,paralleltothelongitudinalaxis, atmidpointbetweentheacromionandolecranon.SSF mea-surements were performed with the non-dominant arm relaxed at the side of the body, obliquely tothe longitu-dinalaxis,followingtheorientationoftheribs,locatedtwo centimetersbelowthelowerangleofthescapula.
The skinfolds were measured in triplicate using a sci-entific adipometer (Cescorf®, Brazil). All equipment was calibratedandthetechniquesusedtoobtainmeasurements were standardized.18 The anthropometric assessment and
nutritionalstatus classificationwere carriedout basedon
thefollowingcriteriaandtoolsoftheWHO20,21:
Childrenagedzerotofiveyears:theWHO’sAnthroPlus
software(version 3.2.2,2011, WorldHealthOrganization,
Geneva,Switzerland)wasused,whichdeterminesz-scores
fortheweight/height(W/H),weight/age(W/A),height/age
(H/A), body mass index/age (BMI/A), upper arm
circum-ference/age (AC/A), tricipital skinfold/age (TSF/A), and
subscapularskinfold/Age(SSF/A)ratios.
Children olderthan five years: the WHO’sAnthro Plus
software(version 3.2.2,2009, WorldHealthOrganization,
Geneva,Switzerland)wasused,whichdeterminesz-scores
for W/A, H/A, and BMI/A ratios. z-score data for AC/A,
TSF/A and SSF/A ratios were evaluated according to the
reference values of Frisancho.22 The premature infants
(n=18) were evaluated using the corrected age up to 2
years.23
Statisticalanalysis
Samplesizewascalculatedconsideringthemeansand stan-darddeviationofhospitallengthofstayfoundinthestudy bySeckerandJeejeebhoy,7of5.3±5.0daysforthegroup
ofwell-nourishedchildrenand8.2±10daysfor thegroup
of malnourishedchildren, witha power of 80%and a
sig-nificancelevelof0.05,resultinginatotalof236patients.
Therequiredsamplesizetotestinterobserverreliabilitywas
calculatedbasedontheKappavalueof 0.6,consideringa
powerof80% andsignificancelevelof 0.05,resultingina
subgroupof61patients.
Quantitative variables were expressed as mean and
standarddeviationormedianandinterquartilerange.
Cat-egoricalvariablesweredescribedasabsoluteandrelative
frequencies.One-way ANOVAwithposthocTukeytestwas
applied to compare means between groups. In case of
asymmetry, Kruskal---Wallis test was used. When
compar-ingproportionsbetweengroups,Pearson’schi-squaredtest
andprevalence ratiowitha 95%confidence intervalwere
applied. The association between nutritional assessment
methodswasassessedbyKendallcoefficient.Theagreement
betweenthemethodswasevaluatedbyKappacoefficient.
Thesignificancelevelwassetat5%(p<0.05).
Results
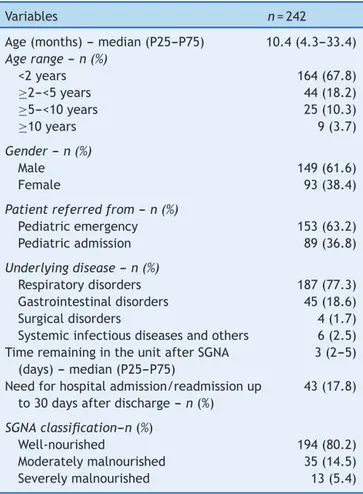
The sample comprised 242 patients, with a median age of approximately 10 months (25th---75th percentiles: 4.3---33.4),withminimumofonemonthandamaximumof 162months.Theagerangeyoungerthan2years predomi-nated(67.8%),aswellasthemalegender(61.6%).Sample characterizationisshowninTable1.
Table1 Characterizationofthestudysample.
Variables n=242
Age(months)---median(P25---P75) 10.4(4.3---33.4)
Agerange---n(%)
<2years 164(67.8)
≥2---<5years 44(18.2)
≥5---<10years 25(10.3)
≥10years 9(3.7)
Gender---n(%)
Male 149(61.6)
Female 93(38.4)
Patientreferredfrom---n(%)
Pediatricemergency 153(63.2)
Pediatricadmission 89(36.8)
Underlyingdisease---n(%)
Respiratorydisorders 187(77.3) Gastrointestinaldisorders 45(18.6)
Surgicaldisorders 4(1.7)
Systemicinfectiousdiseasesandothers 6(2.5) TimeremainingintheunitafterSGNA
(days)---median(P25---P75)
3(2---5)
Needforhospitaladmission/readmissionup to30daysafterdischarge---n(%)
43(17.8)
SGNAclassification---n(%)
Well-nourished 194(80.2)
Moderatelymalnourished 35(14.5)
Severelymalnourished 13(5.4)
SGNA,SubjectiveGlobalNutritionalAssessment.
Table2 AssociationbetweenSubjectiveGlobalNutritionalAssessment(SGNA)dataandobjectiveanthropometric measure-ments(z-score).
Variables N SGNA p rKendall
Well-nourished Moderatelymalnourished Severelymalnourished
Mean±SD Mean±SD Mean±SD
W/H---zscore 208 0.72±1.40b −0.82±0.97a −1.04±2.66a <0.001 −0.36 W/A---zscore 233 0.31±1.13b −1.57±0.51a −2.23±0.76a <0.001 −0.53 H/A---zscore 242 −0.16±1.23c −1.49±0.98b −2.43±2.04a <0.001 −0.37 BMI/A---zscore 242 0.57±1.43b −0.98±1.14a −0.77±2.87a <0.001 −0.34 AC/A---zscore 198 0.45±1.12b −0.65±1.06a −0.83±1.76a <0.001 −0.32 TSF/A---zscore 198 0.63±1.25b −0.23±1.06ab −0.52±1.24a <0.001 −0.23 SSF/A---zscore 198 0.82±1.38b −0.25±1.20a −0.29±1.34a <0.001 −0.25
SGNA,subjectiveglobalnutritionalassessment;W/H,weightforheight;W/A,weightforage;H/A,heightforage;BMI/A,bodymass indexforage;AC/A,upperarmcircumferenceforage;TSF/A,tricepsskinfoldthicknessforage;SSF/A,subscapularskinfoldthickness forage.
Datawereexpressedasmean±standarddeviation.
a,bEquallettersdonotdifferbyTukeytestatthe5%significancelevel.
Of the totalsample, 153patients were treated at the EmergencyPediatric Unit (63.2%) and89 at theInpatient Pediatric Unit (36.8%). The most frequent diagnosis was respiratorydisease(77.3%),followedbygastrointestinal dis-ease(18.6%).
Psychometricproperties
Concurrentvalidity
Nutritionalstatus, as determinedby the SGNA, was com-pared with anthropometric measurements. According to the SGNA, 194 patients (80.2%) were classified as well-nourished,35patients(14.5%)asmoderatelymalnourished, and13patients(5.4%)asseverelymalnourished.
Overall,therewasasignificantdifferencebetweenthe groups;thegroupclassifiedaswell-nourishedshowed signi-ficantlyhighervaluesthantheother two(moderatelyand severelymalnourished)inallnutritionalassessment meth-ods(objectiveandsubjective). However,amongthe mod-eratelyandseverelymalnourished,thedifferencewasonly significantinrelationtoheight/ageratio(Table2).Kendall
coefficients disclosed the weak-to-regular associations
betweenthenutritionalassessmentmethods.Theratiothat
showedthegreatestassociationwithSGNAwasweight/age.
Predictivevalidity
The need for hospital admission/readmission occurred in 43 cases (17.8%). The median (25th---75th percentiles) of timeofadmission/readmissionwastwodays.The probabil-ityofadmission/readmissionwasapproximatelyfourtimes higherinmoderatelymalnourishedpatientswhencompared to normal weight ones (PR=3.96; 95% CI: 2.27---6.91). In severelymalnourishedpatients,theprobabilityofhospital admission/readmissionwasapproximatelyfivetimesgreater when comparedtonormal weightones(PR=4.97; 95%CI: 2.61---9.48).
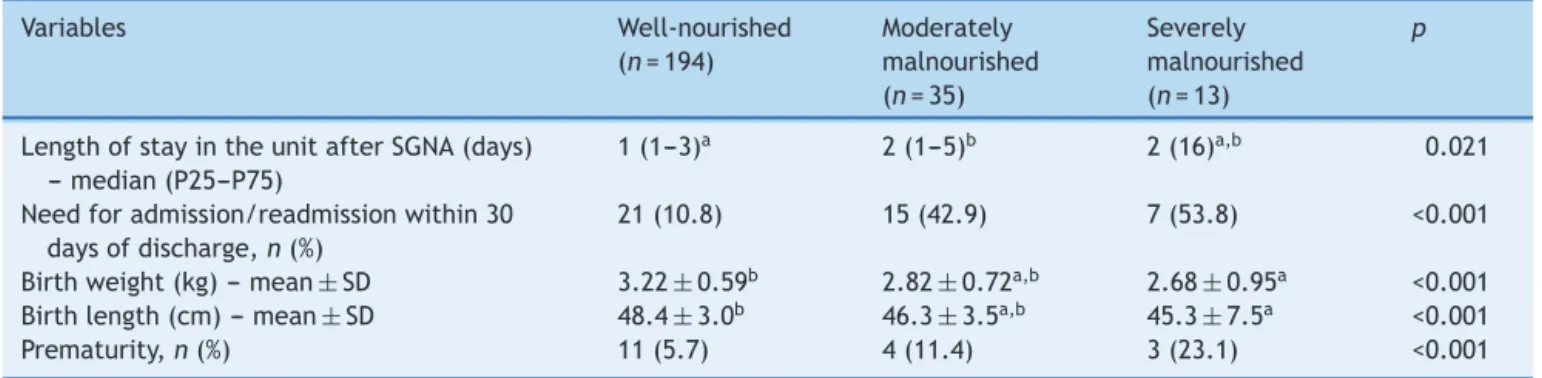
Nutritional status classified by SGNA was associated withall assessed outcomes (Table3). Patientsconsidered
by SGNA as severely malnourished had lower weight and
length at birth than the group of patients considered
well nourished (p<0.05). Moreover,the need for hospital
admission/readmission and prematurity increasedwithan
increasingdegreeofmalnutrition(p<0.001).
Table3 AssociationbetweenSubjectiveGlobalNutritionalAssessment(SGNA)dataandoutcomes.
Variables Well-nourished
(n=194)
Moderately malnourished (n=35)
Severely malnourished (n=13)
p
LengthofstayintheunitafterSGNA(days) ---median(P25---P75)
1(1---3)a 2(1---5)b 2(16)a,b 0.021
Needforadmission/readmissionwithin30 daysofdischarge,n(%)
21(10.8) 15(42.9) 7(53.8) <0.001
Birthweight(kg)---mean±SD 3.22±0.59b 2.82±0.72a,b 2.68±0.95a <0.001 Birthlength(cm)---mean±SD 48.4±3.0b 46.3±3.5a,b 45.3±7.5a <0.001
Prematurity,n(%) 11(5.7) 4(11.4) 3(23.1) <0.001
SGNA,SubjectiveGlobalNutritionalAssessment.
Datawereexpressedasmean±standarddeviation,median(P25---P75),orabsolutenumber(%)asindicated.
Interobserverreliability
There was good interobserver agreement (kappa=0.74; p<0.001), and the percentage of well-nourished, moder-atelymalnourished,andseverelymalnourishedindividuals weresimilarforthetwoobservers.Thecorrelationoccurred in56of61cases(92%).
Discussion
Subjective global assessment has been widely used, asit isaneasy-to-performmethodthatdoesnotrequire expen-siveresourcesandcanbeperformedby professionalsthat comprisethemultidisciplinaryteam.14
This study translated and validated the SGNA for the
Brazilian pediatric population, through the following
psy-chometricproperties:concurrentandpredictivevalidityand
interobserverreliability.
Concurrent validityassessesthecorrelation of thetool
withanothermeasure(thegoldstandard)usedtomeasure
whatisbeingassessed,bothappliedsimultaneously.24This
studyfoundasignificantassociationbetweenSGNAand
com-monlyusedanthropometricmeasures,asreportedby
Brazil-ianstudiesinvolvingadultswithdifferentpathologies.3,25---27
Theresultswerealsosimilartothosefoundintheoriginal
studybySeekerandJeejeebhoy7involvingchildren
under-goingsmallsurgicalprocedures.However,itis noteworthy
thattheagreementobserved betweenthemethods, SGNA
andanthropometricmeasures, wasweak-to-regularinthis
study(p<0.001).
The predictive validity includes future predictions,
regardingthequalitywithwhichatoolcanpredictafuture
criterion.24 The nutritional status evaluatedby SGNA was
associated with all assessed outcomes (need for hospital
admission/readmission within 30 days after hospital
dis-charge, length of hospital stay after SGNA, weight and
length at birth,and prematurity)(p<0.05). An increasing
degreeofmalnutritionaccordingtotheSGNAclassification
wasassociatedwithincreasedcomplications.Studiesusing
subjectiveassessmentasanevaluationmethodofthe
nutri-tionalstatusof hospitalizedpatientshave alsoshown this
power.7,26,28
Theinterobserverreliabilityevaluatesthe
reproducibil-ity of a tool through its application by two or more
observers.24 In this study, there was good reliability
(Kappa=0.74;p<0.001),higherthantheonefoundin the
originalstudybySeckerandJeejeebhoy.7
Becausethisisasubjectivemethod,theSGNA
diagnos-ticaccuracydependsonobserver’sexperienceandtraining,
whichisitsmaindisadvantage.However,studiescarriedout
with adultsalso attained a level of agreementsimilar to
thatobtainedinthisstudy.Inanearlystudyonnutritional
status assessment,Baker etal.15 showedgood agreement
between their evaluators (Kappa=0.72), as well as
Det-sky et al.29 when they standardized the clinical method,
creatingasubjective nutritionalassessmentquestionnaire
(Kappa=0.78).Inmorerecentstudies,aweak-to-moderate
concordancewasobservedbetweentheevaluators.Secker
and Jeejeebhoy,7 studyingsurgical pediatric patients in a
hospitalinCanada,obtainedKappa=0.28.Beguettoetal.,30
studyingadultpatientsadmittedtoauniversitygeneral
hos-pitalinPortoAlegre,RS,foundKappa=0.46.
The evaluation of the psychometric properties of the
SGNAinthisstudyshowedthetoolhasgoodinterobserver
reliability,in additiontohavingconfirmed theconcurrent
andpredictivevalidityofthequestionnaires.Itsapplication
inBrazilianchildrenandadolescentsandin different
clin-icalsituationsfromthatoftheoriginalstudyshowedgood
results.Afterthetranslationand studyofthe
psychomet-ricpropertiesoftheSGNA,thetoolshowedtobereliable
andvalidforassessingthenutritionalstatusofchildrenand
adolescents.
In this study,hospital stay showed noassociation with
theSGNA,unlikewhatotherstudiesreported.7,9,25 A
possi-bleexplanationmaybe duetothe factthat theselected
patients had acute diseases and were admitted through
thePediatricEmergencyUnit. In thestudy by Seckerand
Jeejeebhoy,7patientswerefromtheSurgicalInpatient
Pedi-atricUnit.
Alimitationofthisstudywasthedifficultyofperforming
biochemicalteststoconfirm thediagnosisofthepatient’s
nutritionalstatus.However,thepositiveaspectofthestudy
wasthedemonstration ofthehigh sensitivityoftheSGNA
questionnairefor nutritionalrisk andmalnutrition
diagno-sis.The fact that it considers the clinical and functional
alterations, which can lead the patient to a situation of
protein,energy,andimmunecompetenceloss,favoredthe
immediatediagnosisofnutritionalriskandmalnutrition.
SGNAvalidationfortheBrazilianpediatricpopulationcan
beastimulusfortheutilization ofthismethodas
system-aticassessment in pediatric services, in different clinical
situations. This can be performed as soon asthe patient
arrivesatthehospital,facilitatingtheidentificationofthose
whomaybeatnutritionalrisk,sothatthemostappropriate
nutritionalinterventioncanbeperformed.
Themethodologyusedandthecarefultranslationprocess
allowfor the conclusionthat SGNA isa valid andreliable
instrumentfor theassessment of thenutritional statusof
Brazilianpediatricpatients.
SGNAisausefuldiagnostictoolforassessingnutritional
status,withsimilarefficacytoanthropometricparameters,
regardlessoftheclinicalstatusofpatients.Thisstudy
vali-datedtheSGNAquestionnaireinthissampleofhospitalized
pediatricpatients,allowingitsuseforclinicalapplications
andforresearchpurposesintheBrazilianpopulation.
Funding
ThestudyreceivedsupportfromFIPE,Researchand Gradu-ateStudy Group,Hospital deClinicasdePortoAlegreand Conselho Nacional de Desenvolvimento Científico e Tec-nológico(CNPq).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Appendix
A.
Supplementary
data
Supplementary data associated with this article can be found, in the online version, at doi:10.1016/j.jped. 2015.03.005.
References
1.RamosCV,DumithSC,CésarJA.Prevalenceand factors asso-ciatedwithstuntingand excessweightin childrenaged 0---5 years from the Braziliansemi-arid region.J Pediatr (Rio J). 2015;91:175---82.
2.JoostenKF,HulstJM.Malnutritioninpediatrichospitalpatients: currentissues.Nutrition.2011;27:133---7.
3.RaslanM,GonzalesMC,DiasMC,Paes-BarbosaFC,Cecconello I,WaitzbergDL.Applicabilityofnutritionalscreeningmethods inhospitalizedpatients.RevNutr.2008;21:553---61.
4.Rocha GA,RochaEJ, Martins CV. Theeffects of hospitaliza-tion on thenutritional status ofchildren. J Pediatr (Rio J). 2006;82:70---4.
5.Hendricks KM,Duggan C,Gallagher L, CarlinAC,Richardson DS, Collier SB, et al. Malnutrition in hospitalized pedi-atricpatients:currentprevalence.ArchPediatrAdolescMed. 1995;149:1118---22.
6.PawellekI,DokoupilK,KoletzkoB.Prevalenceofmalnutrition inpaediatrichospitalpatients.ClinNutr.2008;27:72---6. 7.SeckerDJ,JeejeebhoyKN.SubjectiveGlobalNutritional
Assess-mentforchildren.AmJClinNutr.2007;85:1083---9.
8.Mehta NM, Corkins MR,Lyman B, Malone A, Goday PS, Car-neyLN,etal.Definingpediatricmalnutrition:aparadigmshift toward etiology-related definitions. JPEN J Parenter Enteral Nutr.2013;37:460---81.
9.SarniRO,CarvalhoMdeF,doMonteCM,AlbuquerqueZP,Souza FI.Anthropometricevaluation,riskfactorsformalnutrition,and nutritionaltherapyforchildreninteachinghospitalsinBrazil. JPediatr(RioJ).2009;85:223---8.
10.KyleUG,GentonL,PichardC.Hospitallengthofstayand nutri-tionalstatus.CurrOpinClinNutrMetabCare.2005;8:397---402. 11.ChimaCS.Dietmanualstopracticemanuals:theevolutionof
nutritioncare.NLNConvPap.2007;22:89---100.
12.Barbosa-SilvaMC,BarrosAJ.Indicationsandlimitationsofthe use of subjective global assessment in clinical practice: an update.CurrOpinClinNutrMetabCare.2006;9:263---9. 13.Barbosa-Silva MC, de Barros AJ. Subjective global
assess-ment: Part 2. Review of its adaptations and utilization in different clinical specialties. Arq Gastroenterol. 2002;39: 248---52.
14.Seres DS. Surrogate nutrition markers, malnutrition, and adequacy of nutrition support. NLN Conv Pap. 2005;20: 308---13.
15.Organizac¸ãoMundialdaSaúde.Classificac¸ãoEstatística Inter-nacionaldeDoenc¸aseProblemasRelacionadosàSaúde/CID-10 10arevisão.In:Traduc¸ãodoCentrocolaboradordaOMSpara
a Classificac¸ãode Doenc¸as emPortuguês.5thed.São Paulo: EDUSP;1997.
16.Baker JP, Detsky AS, Wesson DE, Wolman SL, Stewart S, WhitewellJ, et al. Nutritional assessment: a comparison of clinicaljudgmentandobjectivemeasurements.NEnglJMed. 1982;306:969---72.
17.AlvesMM,CarvalhoPR,WagnerMB,CastoldiA,BeckerMM,Silva CC.Cross-validationoftheChildren’sandInfants’Postoperative PainScaleinBrazilianchildren.PainPract.2008;8:171---6. 18.Orientac¸õesparaacoletaeanálisededadosantropométricos
emservic¸osdesaúde:NormaTécnicadoSistemadeVigilância AlimentareNutricional---SISVAN.Brasília:MinistériodaSaúde, Secretaria de Atenc¸ão à Saúde, Departamento de Atenc¸ão Básica;2011.
19.Secker DJ, Jeejeebhoy KN. How to perform Subjective Global Nutritionalassessment inchildren. J AcadNutrDiet. 2012;112:424---31.
20.World Health Organization (WHO). WHO Child Growth Standards:length/height-for-age,weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methodsanddevelopment.Geneva:WorldHealthOrganization; 2006.
21.World Health Organization (WHO). WHO Child Growth Stan-dards:methodsanddevelopment:headcircumference-for-age, armcircumference-for-age, tricepsskinfold-for-ageand sub-scapularskinfold-for-age.Geneva:WorldHealthOrganization; 2007.
22.FrisanchoA. Anthropometric standards:aninteractive nutri-tionalreferenceofbodysizeandbodycompositionforchildren andadults. 2nded.Ann Arbor:UniversityofMichiganPress; 2008.
23.FentonTR,KimJH.Asystematicreviewandmeta-analysisto revisetheFentongrowthchartforpreterminfants.BMCPediatr. 2013;13:59.
24.BlackerD,EndicottJ.Psychometricproperties:conceptsof reli-abilityandvalidity.In:RushAJ,editor.Handbookofpsychiatric measures.Washington, DC:AmericanPsychiatric Association; 2000.p.7---14.
25.BaccaroF,MorenoJB,BorlenghiC,AquinoL,ArmestoG,Plaza G,etal.Subjectiveglobalassessmentintheclinicalsetting. JPENJParenterEnteralNutr.2007;31:406---9.
26.YamautiAK,OchiaiME,BifulcoPS,deAraújoMA,AlonsoRR, RibeiroRH,et al.Subjectiveglobalassessmentofnutritional statusincardiacpatients.ArqBrasCardiol.2006;87:772---7. 27.Coppini LZ, Waitzberg DL, Ferrini MT, da Silva ML,
Gama-Rodrigues J, Ciosak SL. Comparison of thesubjective global nutrition assessment×objective nutrition evaluation. Rev AssocMedBras.1995;41:6---10.
28.Detsky AS, Baker JP, O’Rourke K, Johnston N, Whitwell J, Mendelson RA, et al. Predicting nutrition-associated complicationsforpatientsundergoinggastrointestinalsurgery. JPENJParenterEnteralNutr.1987;11:440---6.