BrazJOtorhinolaryngol.2015;81(6):681---683
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
CASE
REPORT
Deviant
facial
nerve
course
in
the
middle
ear
cavity
夽
Trajeto
anômalo
do
nervo
facial
na
cavidade
da
orelha
média
Jungkyu
Cho,
Nayeon
Choi,
Sung
Hwa
Hong,
Il
Joon
Moon
∗DepartmentofOtorhinolaryngology-HeadandNeckSurgery,SamsungMedicalCenter,SungkyunkwanUniversitySchoolof
Medicine,Seoul,RepublicofKorea
Received27December2014;accepted17March2015 Availableonline7September2015
Introduction
Anomalousfacialnerve(FN)course canbefound ina
sig-nificant number of cases with auralanomalies. The most
commonanomaly oftheFNinvolves thetympanicportion
overlying the oval window.1---3 Facial canal dehiscence of
thetympanicportionmayberesponsiblefortheanomalous courseofFNovertheovalwindow.Theincidenceoffacial canaldehiscencefoundduringotologicsurgeryisrelatively frequent and is usually related with cholesteatomas.4,5
Aberrant FN course in a patient without accompanying anomalyorcholesteatomahasbeendemonstratedina pre-viouscasereport.6However,thepatienthadnotundergone
imaging evaluation. Herein, the authors report an abnor-malFNcoursein thetympanicportion,without anyother associatedanomalies.
Case
report
An 18-year-old male presented to the outpatient clinic with left-sided non-progressive hearing loss since child-hood.Otoscopicexaminationrevealedbundle-likestructure behind the posterior portion of the tympanic membrane
夽
Please citethisarticle as:ChoJ,ChoiN, HongSH,MoonIJ. Deviantfacialnervecourseinthemiddleearcavity.BrazJ Otorhi-nolaryngol.2015;81:681---3.
∗Correspondingauthor.
E-mail:[email protected](I.J.Moon).
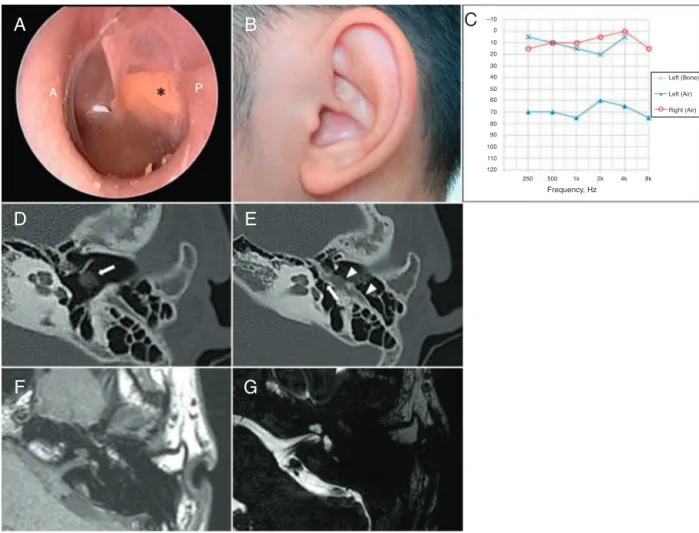
(Fig. 1A). Other physical exams showed no facial nerve palsy or auricular anomaly (Fig. 1B). Pure-tone average (0.5, 1, 2, and 3kHz) showed air-bone gap of 58dB (averagebone-conductionthreshold=3.75dB, average air-conduction threshold=62.5dB) (Fig. 1C). Accordingly, computedtomography(CT)scanofthetemporalbonewas performedforevaluationofthemiddleearcavityalongwith ossicularstructures.CTrevealedahypoplastic middle ear cavity,incudostapedialjointseparation,andlateralization of the tympanic segment of the facial nerve, which was observedbehindthetympanicmembrane (Fig.1D andE). Internalauditory canalMRI demonstratednoanomalies in theinnerear(Fig.1FandG).Sinceaberrantcourseofthe tympanicsegment of facial nerve was identified, further surgicalexplorationwasdeferred.
Discussion
Most patients with FN anomaly do not have any clin-ical symptoms. Conductive hearing loss, mainly due to associated ossicular disruption, may be the only clinical presentation. Therefore, it is difficult to suspect middle earmass asan unusual presentation of the FNcourse or evenasa structural or passage anomaly, especiallywhen other associated anomalies are not noted. Furthermore, cases of FN dehiscence shown in previous studies were mainlyassociatedwithcholesteatomasor congenitalaural atresias.2,3,5
However,aberrant course of FNlateral to the ossicles withoutaccompanyingauricularanomalywasreportedina
http://dx.doi.org/10.1016/j.bjorl.2015.03.011
682 ChoJetal.
D
P A
A
G
E
F
0
Right (Air) Left (Air) Left (Bone)
8k 4k 2k
Frequency, Hz
1k 500 250 120 110 100 90 80 70 60 50 40 30 20 10 –10
C
B
Figure1 (A)Otoscopicexaminationrevealsstreak-likestructure(asterisk)behindtheeardrum.Yellowishbundle-likestructure isplacedatpostero-superiorquadrant.P, posteriorcanal wall;A,anteriorcanal wall.(B)External earshows normalstructure withoutanomaly.(C)Puretoneaudiometryshowsconductivehearingloss;air-boneconductiongapof58dBintheleftear.(D) Facialnervedehiscenceoftympanicsegment,whichisseenbehindthetympanicmembrane(whitearrow).(E)Incudostapedial dislocation(whitearrow)withlateralizedfacialnerve(whitearrowhead).(F)Intermediatesignalintensityoftheaberrantfacial nervecourse.(G)Well-delineatedfacialandvestibulocochlearnerveininternalauditorycanal.
priorcase.6Hence, itisadvisablenottoexcludeaberrant
FNpathwayinpatients withoutaccompanying anomaly or other middle ear disease.In the previous report of aber-rantFNcoursewithoutotheranomalies,imagingevaluation was not performed preoperatively. Surgical exploration withelectricalstimulationmonitoringwasusedtoconfirm the middle ear mass as the FN.6 However, these
surgi-calprocedures in the middle ear cavity couldlead to FN damage.Thus,ifanomalousFNissuspected,preoperative imagingevaluationismandatory.Inthepresentcase, radio-logic evaluation was performed before planning surgical exploration.
CTimagingprovidesprecisepredictionoftheFNcourse, coincidingwithsurgicalfindings inmost casesof congeni-talauralatresia.2Therefore,theprimaryimagingmodality
forevaluationoftheFNcourseshouldincludehigh resolu-tionCT.InpreviousstudiesofanomalousFNofthetympanic portion,theFNrunsmoreanterolaterallyinthemiddleear cavitythaninnormalpatients.
Therefore, physicians should suspect the mass located intheposteriormiddleearcavityasavariationof theFN pathway and performimaging evaluation before planning interventions.1,2,4,6
Final
comments
Unusual structure seen through the tympanic membrane shouldbeevaluatedbyimagingbeforedefinitivetreatment. CTis especiallyuseful for thispurpose, becausethe tym-panic segmentof the FNlying lateral tothe ossicles can be easily identified. If aberrant course of the FN is sus-pectedbysymptomsandclinicalfindings,physiciansshould be cautiousin determining surgical interventions, suchas ventilationtubeinsertionorexplorativetympanotomy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Fu Y, Zhang T. Facial nerve lying lateral to ossicles in one caseofcongenitalauralatresia.IntJPediatrOtorhinolaryngol. 2011;75:597---9.
Deviantfacialnervecourseinthemiddleearcavity 683
preoperativeCTscanningandsurgicalfindings.ActaOtolaryngol. 2008;128:1375---80.
3.HuangBR,JuanCJ,WangCH.Infantilefacialnervecourseinan adultpatientwithcongenitalauraldysplasia.OtolaryngolHead NeckSurg.2008;139:470---1.
4.Selesnick SH, Lynn-MacraeAG. The incidence of facial nerve dehiscence at surgery for cholesteatoma. Otol Neurotol. 2001;22:129---32.
5.Di Martino E, Sellhaus B, Haensel J, Schlegel JG, Westhofen M,PrescherA.Fallopiancanaldehiscences:asurveyofclinical and anatomicalfindings. EurArchOtorhinolaryngol. 2005;262: 120---6.