w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Retrospective
analysis
of
the
elective
tests
of
rigid
proctosigmoidoscopy
performed
in
the
service
of
medical
residency
in
Coloproctology
of
Hospital
Santa
Marcelina
夽
Isaac
José
Felippe
Corrêa
Neto
a,b,∗,
Janaína
Wercka
a,
Angelo
Rossi
Silva
Cecchinni
a,
Eduardo
Augusto
Lopes
a,b,
Hugo
Henriques
Watté
a,b,
Rogério
Freitas
Lino
Souza
a,
Alexander
Sá
Rolim
a,b,
Laercio
Robles
a,caServiceofColoproctology,DepartmentofGeneralSurgery,HospitalSantaMarcelina,SãoPaulo,SP,Brazil bSociedadeBrasileiradeColoproctologia,Brazil
cColégioBrasileirodeCirurgia,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30September2015 Accepted25March2016 Availableonline13April2016
Keywords:
Proctologicalexamination Rigidproctosigmoidoscopy Diagnosis
a
b
s
t
r
a
c
t
Introduction:Proctologicexaminationisadeeplyintimateprocedurewhichdealswithabody areainwhichprejudices,taboosandconstraintsprevail,andmayalsorelatetoprevious trauma;yetthisprocedureisofparamountimportancefortheinvestigationofpatients withsymptomsthatforetellpathologiesassociatedwithdistalcolon,rectumandanus. Objectives:Thisstudyaimedtoanalyzeallcasesscheduledofrigidproctosigmoidoscopy performedbytheColoproctologyService,HospitalSantaMarcelina,in8ofits10yearsof residencyinthespecialty.
Materialsandmethods:Weanalyzedmeanage,genderdistribution,device’sheightofreach inrelationtotheanalverge,thepercentageofabnormaltestsstratifiedtoperform,ornot perform,anoscopyandproctosigmoidoscopy,andmajordiseasesdetected.
Results:844rigidproctosigmoidoscopyproceduresscheduledandperformedbythe Colo-proctologyService,HospitalSantaMarcelina,betweenSeptember2006andAugust2014, wereanalyzed.Thedistributionwassimilarbetweengendersandthemeanagewas51.2 years.Withrespecttothedevice’sheightofreachfromtheanalverge,thesevalueswere stratifiedasfollows:distancereached>15cm,10–15cm,and<10cmfromtheanalverge. Distances>15cmfromtheanalvergewereattainedin692(82%ofRR)tests,between10and 15cmin94(11.1%)tests,and<10cmin58(6.9%)tests.
Conclusion:Inthisstudy,itwasfoundthatproctologyexaminationandrigid proctosigmoi-doscopyaremandatoryproceduresincasesofsymptomsdependingonthesepractices.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽
ThisstudywasconductedbytheProgramofMedicalResidencyinColoproctology,DepartmentofGeneralSurgery,HospitalSanta Marcelina,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](I.J.F.C.Neto).
http://dx.doi.org/10.1016/j.jcol.2016.03.007
Análise
retrospectiva
de
exames
eletivos
de
retossigmoidoscopia
rígida
realizadas
no
servic¸o
de
residência
médica
de
Coloproctologia
no
Hospital
Santa
Marcelina
Palavras-chave: Exameproctológico Retossigmoidoscopiarígida Diagnóstico
r
e
s
u
m
o
Introduc¸ão: Oexameproctológico,apesardeprofundamenteíntimoedelidarcomárea do corpo na qual imperam preconceitos, tabus e constrangimento, podendo inclusive relacionar-seatraumasprévios,édesumaimportânciaparaainvestigac¸ãodepacientes comsintomasquepredizempatologiasassociadasaocólondistal,retoeânus.
Objetivos:Analisartodososcasosderetossigmoidoscopiasrígidasrealizadasdeforma agen-dadapeloservic¸odeColoproctologiadoHospitalSantaMarcelinaem8deseus10anosde residênciamédicanaespecialidade.
Materiaisemétodos: Analisou-seamédiadeidade,distribuic¸ãoporsexo,alturadealcance doaparelhoemrelac¸ãoàbordaanal,percentagemdeexamesanormaiscomestratificac¸ão quandorealizadoounãoaanuscopiaeretossigmoidoscopiaeasprincipaisdoenc¸as detec-tadas.
Resultados: Foramavaliadas844retossigmoidoscopiasrígidasrealizadaspeloservic¸ode ColoproctologiadoHospitalsantaMarcelina,deformaagendada,entresetembrode2006e agostode2014.Adistribuic¸ãofoisemelhanteentreossexoseamédiadeidadefoide51,2 anos.
Comrelac¸ãoàalturaemrelac¸ãoàbordaanal,estratificou-seessesvaloresemmaiorque 15cm,entre10e15cmdabordaanalealcanceinferiora10cmdabordaanal.Em692exames foipossívelalcancesuperiora15cmdabordaanal(82%dasRR),em94(11,1%)entre10e 15cm,eem58(6,9%)exames,abaixode10cm.
Conclusão: Verificou-seemnossoestudoqueoexameproctológicoearetossigmoidoscopia rígidasãomandatórioemcasosdesintomatologiaqueassimonecessitem.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este éumartigoOpenAccesssobalicençadeCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Proctologicexaminationisadeeplyintimateprocedure,which dealswithabodyareainwhichprejudices,taboosand con-straintsprevail,andmayalsorelatetoprevioustraumaand abuseissues;yetthisprocedureisofparamountimportance forthe investigation ofpatients with symptomsthat fore-tell pathologies associated with distal colon, rectum and anus,suchasbleeding,changeinbowelhabits,abdominalor perinealpain,mucorrhea,tenesmus,rectalpull,anal inconti-nence,analprolapseortumor,anemia,andothers.
Therefore, it is emphasized that this approach should be done (where appropriate, depending on patient’s com-plaints)byallmedicalassistants,notonlybygeneralsurgeons, digestivetractsurgeonsand,morespecifically,by coloproc-tologists.However,amoredetailed assessmentofthe anal area,rectumanddistalcolonwiththehelpofanoscopyand rigidproctosigmoidoscopyshouldbeperformed,preferablyby morejadedprofessionals.Rigidproctosigmoidoscopy(RR)is thatpartofaproctologicphysicalexaminationthatdepends on greater expertise and knowledge of the region. This examinationconsistsofdirectvisualization ofthemucosal surfaceoftherectumanddistalsigmoidcoloninavariable length,dependingontheequipment,thephysician’s exper-tise,andthepatient’sanatomicalconfiguration,notablyatthe
rectosigmoidtransition.InordertoachieveaneffectiveRR, someprinciplesshouldbefollowed1:
- speed:theexaminationshouldbeperformedintheshortest possibletimeandwithdueeffectiveness;
- minimum air-blowing: excess air during the procedure causesdiscomfortandpaintothepatient;
- thedoctorshouldtalktothepatientduringthe examina-tion:theobjectiveistoexplain,reassureand,ifpossible,to distractthepatient;
- onedoesnotcauseiatrogenicproblems,mainlybleeding, mucosallaceration,andthemostdreadedofall complica-tions:rectalperforationduringtheexamination.
Themaincontraindicationstothis examinationare rep-resented by an acute diverticulitis, suspected peritonitis, hemorrhoidalthrombosis,analfissure,perianalabscess,anal stenosisandanearlypostoperativeperiodofacolorectalor orificialsurgery.
Objective
Materials
and
methods
Thisisaretrospectiveanalysisofall RRexaminations per-formedelectivelybythe ServiceofColoproctology, Hospital SantaMarcelina,in8ofits10yearsofmedicalresidencyin thespecialty.
Previouslytotheexamination,allpatientsunderwent ret-rogradebowelpreparationwithaglycerinsolution12%.Forthe examination,patientshaveadoptedtheknee-chestposition, exceptwhentherewerecontraindicationsoranyage-related limitation.
Meanage, genderdistribution, the origin ofthe patient (i.e.,whetherfrominternalorexternalservice),thedevice’s height ofreach from the anal verge, percentage of abnor-maltestswithstratification(withor withoutanoscopyand proctosigmoidoscopy),andmajordiseasesdetected.RR pro-ceduresperformedduringoutpatientvisitswereexcluded.
Results
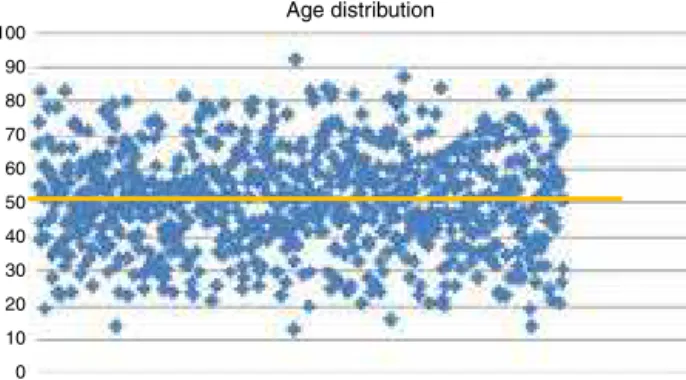
Weevaluated844 RR procedures scheduledand conducted bythe ServiceofColoproctology, HospitalSanta Marcelina, betweenSeptember2006andAugust2014.Themeanagewas 51.2years(13–92years)(Fig.1)and414(49.05%)patientswere male;mostofthetestscamefrominternalhospitalservices, i.e.,622tests(73.7%).Regardingthedevice’sheightofreach fromthe analverge,thevalueswere stratifiedindistances >15cm,10–15cmand<10cmfromtheanalverge.In692 exam-inations,adistance>15cmfromtheanalverge(82%ofRRs) wasreached;in94(11.1%),between10and15cm;andin58 (6.9%)patientsthedevice’sprogressiononlywasupto10cm fromtheanalverge(Fig.2).Inallinwhichtheheightofreach <10cm,thecausewasaninadequatepreparation,painora stenotictumor.Moreover,in14of94tests(14.9%)with progres-sionfrom10to15cm,anexcessiveangulationwasobserved. Theproctosigmoidoscopyhadnormalresultsin677patients (80.2%);butwithrespecttothesecases,inonly270(39.9%)the wholeproctologicalexaminationwasnormal;intheother407 tests(60.1%),somechangewasfound,eitherattheinspection, duringpalpationoratanoscopy.
Ontheother hand,whenthe proctologicalanalysiswas takenasawhole(i.e.,inspection,digitalrectalexamination and palpation,anoscopy and rigidproctosigmoidoscopy),it wasfoundthatthetesthadabnormalresultsin574patients
100
Age distribution
90
80
70
60
50
40
30
20
10
0
Fig.1–Agedistribution.
82.00%
11.10%
>15cm 10-15cm <10cm
6.90%
Fig.2–Heightofrigidrectosigmoidoscopereachinrelation totheanalverge.
(68%),andinonly28.6%ofthesepatientsmoretrainingand expertisewereneededtoachieveadiagnosisbyanoscopyand RR.Thus,ingeneral,thediagnosisoforificialpathologywas onlypossiblewiththeuseofanoscopyandRRin144patients (17.06%);and onlywiththe use ofRR in20patients (2.4%) (Fig.3).
Cancer was diagnosed in63 procedures (7.4%); in44 of these(69.8%),thedigitalrectalexaminationwassufficientfor obtainingthediagnosis ofneoplasia.Thus,itwasobserved thatfrom844RRsperformed,in44(5.2%)ofthemthedigital rectalexaminationwassufficientforthediagnosisofatumor (Fig.4).
Discussion
AccordingtodatafromINCA,2between2012and2013518,510 new casesofcancer were diagnosedinBrazil, and specifi-cally withrespecttocolorectal malignancy,30,140subjects wereaffected,withanequivalentdistributionbetween gen-ders.Thisneoplasiaisthefourthmostcommoncancerinmen andthethirdinwomen.Between55and67%3,4ofcases, colo-rectalcancerisfoundinthedistalsegmentoftheintestinal tract,i.e.inthesigmoidcolonandrectum,andabout35%of thesetumorsarespecificallylocatedintherectum.5
Inthisregard,whenreaching25cmfromtheanalverge, RRallowstheestablishmentofadiagnosisinabout65%ofall colorectalcancers.6However,inonly50%oftheprocedures, the device will progressup to20cmfrom theanal verge.6 Moreover,beingarigidtube,theproctosigmoidoscopeisstill quitesensitiveandspecificinordertomeasuretheheightof thetumorfromtheanalvergeorrectumvalves.
Despite being aninvasive and uncomfortable procedure tothepatient,Elias etal.7conductedastudy toverify the patient’simpressionwithrespecttotheproctology examina-tion bythe residentphysician.In thisstudy,these authors
844 patients
Abnormal - 574
Inspection and DRE – 71.4%
Anoscopy and RR – 28.6%
Diagnosis with anoscopy: 17.6%
Diagnosis with rigid proctosigmoidoscopy: 2.4% Normal - 270
No 93%
Yes 7%
Fig.4–Percentageofneoplasmdiagnosesinanorectal examinationsbyinspection,digitalrectalexamination,
anoscopyandrigidproctosigmoidoscopy.
analyzed100patientsundergoingconsultationandafull proc-tologicaltestthroughectoscopy, digitalrectalexamination, anoscopyandrigidproctosigmoidoscopy.Eliasetal.showed that87%ofpatientsacceptedwellthepresenceofresidents, 11%remainedindifferent,1%foundtheirpresence unpleas-ant,and1%didnotanswer.Regardingtheresidents’gender, nostatisticallysignificantcorrelationwasfoundbetweenthis variableand therefusal oracceptanceoftheirpresenceby patients.
Similarly,Simpson et al. 8 conductedan interview with colorectalsurgeonsfromAustraliaandNewZealand.Ofthe 35professionals who answeredthe questionnaire,30 (85%) routinelyperformRRintheiroffices.
Inthiscontext,Diogenesetal.9 intendedtoevaluatethe proctosigmoidoscopyfindingsinacolorectalcancerscreening inasymptomaticpatientsover50years.Withthatinmind, theseauthors studied208patientsintheperiodof approx-imately one year, achieving 94.73% of normal results; in theremaining5.26%,thepresenceofhyperplasticor adeno-matouspolypswasdiagnosed,andnotonecaseofmalignancy inthesamplestudiedwasfound.
Between1989and1996,Balkanetal.10evaluated119RR proceduresin100patientsaged8monthsto14years with complaintsofanalbleeding.Theseauthorsusedasexclusion criteriathe presenceofanal fissure,hemorrhoidsand anal infection.Theprocedurehadabnormalresultsin60patients andtheprimarydiagnosiswasarectalpolypin53.3%ofcases, followedbyproctitisin26.7%.Ofthosepatientswitharectal polyp,theauthorsestablishedthediagnosisbydigitalrectal examinationin66%ofcases,withafalse-positiverateof25% andafalse-negativerateof12%.
Studiesontheapplicability ofRR arerelatively rareand dated,mainlywithreferencetotheacquisitionand progres-sivedevelopmentofmodernmethodsfortherectalwork-up.
Selbyetal.6showedthatpatientsundergoingrigid proctosig-moidoscopy in colorectal cancer screenings in the 10-year periodpriortothe study hadonly30% offatalcancerrisk versussubjectsnotscreenedformalignancyinthegroupof patientsalreadyknowntobecarriersofrectal,rectosigmoid transition,ordistalsigmoidcancer.
In addition, and highlighting the usefulness of RR – even whenthe most advancedpropaedeutics are available – Schoellhammer et al.11 set out to determine the degree towhich rectaland rectosigmoidtumorsshowed achange intheirtreatment, basedontheheightofmeasuredinjury obtainedwithRRandcolonoscopy.Withthatinmind,these authorssubdividedtheir53patientsexaminedbycolonoscopy intocarriersofinjuryinthelower rectum(0–7cmfrom the anal verge), middle rectum (8–11cm from the anal verge), highrectum(12–15cmfromtheanalverge)andrectosigmoid region(>15cmfromtheanalverge);thisdone,theseauthors comparedtheirfindingswiththesedistancesobtainedwith RR.
Alsointhisstudy,whenlow,mediumandhighrectaland rectosigmoidtumorswereanalyzed,itsauthorsobserved dif-ferencesinthemeasureddistancefromtheanalvergetothe injurybycolonoscopyversusRR:0.8cm,1.8cm, 3.1cm and 5cmrespectively.Thus,anintermediateKappaindexbetween thedifferencesofheightmeasurementsofthelesioninthe highrectumandthesigmoidregionwasobtained,showing thatthemostproximaltheneoplasiawaslocatedrelativeto theanalverge,thegreaterthediscrepancybetweenthe mea-surementsobtainedbycolonoscopyandRR.Moreover,these authorsreportedthattheadditionofRRpreviouslytothe ther-apeuticdecisionmakingchangedthetreatmentplanin25% ofpatients.11
Although this isa testusuallyapplied during coloproc-tological consultation, the presenceoffecal residue in the rectummaycompromiseitseffectivenessinsuchawaythat, withrespecttotheneedtopreparetheareaforarigid proc-tosigmoidoscopy,itisknownthatabout50%ofthetestshave limitationsduetothepresenceoffecalresidue.12
Withthatinmind,Bulmeretal.13 conducteda random-izedstudyinvolving131patientsinordertocomparesubjects withretrogradedistalmechanicalpreparationversus those whodidnotmakeanypreparation.Itwasfoundthatamong thosepatientsundergoingbowelpreparation,itwaspossible toinspectmorethan75%oftherectalmucosacircumference in79%ofpatients.Ontheotherhand,amongthosesubjects who didnotundergopreparation,thiswasonlypossiblein 26.2%(p<0.05).Moreover,amongthosesubjectsundergoing bowel preparation, it was possible to introducethe device in 83.3%ofpatients; asto those subjectswithout prepara-tion,thiswasonlypossiblein46.2%oftheexaminedpatients (p<0.05).
Conclusion
orificialpathology.Thus,thankstoitssimplicityandthe abil-itytobecarried out anypracticing doctor, thistestshould neverbeoverlooked.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SobradoCW,CorrêaNetoIJF.In:SobradoCW,NadalSR,Souza AHSJr,editors.Manualdedoenc¸asanorretais:aspectos práticos.Exameproctológico:quandoecomorealizar.Office Editora;2013.p.403–15.
2. INCA:Availableat:http://www.inca.gov.br/estimativa/2014/
[Accessedon30September2015].
3. VikramR,IyerRB.PET/CTimaginginthediagnosis,staging, andfollow-upofcolorectalcancer.CancerImaging. 2008:S46–51.
4. HayneD,BrownRS,McCormackM,QuinnMJ,PayneHA,Babb P.Currenttrendsincolorectalcancer:site,incidence, mortalityandsurvivalinEnglandandWales.ClinOncol. 2001;13:448–52.
5.RajputA,DunnKB.Surgicalmanagementofrectalcancer. SeminOncol.2007;34:241–9.
6.SelbyJV,FriedmanGD,QuesenberryCP,WeissNS.A
case–controlstudyofscreeningsigmoidoscopyandmortality fromcolorectalcancer.NewEnglJMed.1992;326:653–7.
7.EliasIP,LacerdaFilhoA,MansurES,CamaraFG,SenaKA. Visãodopacientequantoàparticipac¸ãodoresidenteno exameproctológicoemambulatório.RevBrasColoproct. 2006;26:389–93.
8.SimpsonPJB,McMurrickPJ,PolglaseAL,KohCE.Comparison ofequipmentmanagementandcleaningprotocolsforrigid sigmoidoscopy.ANZJSurg.2010;80:728–31.
9.DiogenesCVVN,MarianelliR,SoaresRPS,AbudRM,Falleiros V,Vilari ˜noTC.Achadosderetossigmoidoscopiano
rastreamentodecâncercolorretalempacientes assintomáticosacimade50anos.RevBrasColoproct. 2007;27:403–7.
10.BalkanE,Kırıs¸tıo ˘gluI,GürpınarA,ÖzelI,SınmazK,Do ˘gruyol H.ArchDisChild.1998;78:267–8.
11.SchoellhammerHF,GregorianAC,SarkisyanGG,PetrieBA. Howimportantisrigidprostosigmoidoscopyinlocalizing rectalcancer.AmJSurg.2008;196:904–8.
12.LeeM.Comparisonofthreebowelpreparationsfor sigmoidoscopy.WestIndiesMedJ.1993;42:118–20.