w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Correlation
of
the
three-dimensional
ultrasound
findings
with
pathology
in
patients
with
deep
pelvic
infiltrating
endometriosis
submitted
to
surgery
夽
Maria
Cecilia
Lunardelli
da
Silva
a,
Doryane
Maria
dos
Reis
Lima
a,b,∗,
Univaldo
Etsuo
Sagae
b,c,daFaculdadeAssisGurgacz(FAG),Cascavel,PR,Brazil
bUniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
cUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
dUniversidadeEstadualdoOestedoParaná(UNIOESTE),FozdoIguac¸u,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12August2013 Accepted3March2015 Availableonline21March2016
Keywords:
Endometriosis Correlation Ultrasound Pathology Diagnosis
a
b
s
t
r
a
c
t
Objective:Thisstudyaimstocorrelatethefindingsofthethree-dimensionalanorectal ultra-sonography(3D-AUS) withpathologicalfindingsinpatientswithdeeppelvicinfiltrating endometriosis.
Methods:Prospectivestudyofaseriesof40patientswithdeeppelvicinfiltrating endometri-osisdiagnosedbythree-dimensionalanorectalultrasonographyandwhoweresubmittedto alaparoscopy.Thespecimenswereexaminedhistologicallyandcomparedwiththeresults ofthethree-dimensionalanorectalultrasonography.Theresearchwasconductedbetween March2008andMarch2011.
Results:Theresultsoftheexaminationswere:72.5%ofpatients(n=29)withendometriosis, 12.5% (n=5)withnonspecificchronic inflammatoryreaction,5%(n=2)withnonspecific fibroustissue,2.5%(n=1)withadenomyoma,2.5%(n=1)withcolonicmucosawithfoci ofrecenthemorrhage,edemaoflaminapropriaandsuperficialerosions,2.5%(n=1)with hyperplasiaoflymphoidfollicles,andtheremaining2.5%(n=1)withperitonealtissuewithin normallimits.
Conclusion: Weconcludethattheuseofthree-dimensionalanorectalultrasonographyin patientswithdeeppelvicinfiltratingendometriosisaidinthediagnosisofrectallesions, whencomparedwiththepathologicalfindingsofsurgicalspecimens.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽
ThisstudywasconductedinHospitalGenesis,GastroclínicaCascavel,Cascavel,PR,BrazilandintheFaculdadeAssisGurgacz(FAG), Cascavel,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.M.dosReisLima).
http://dx.doi.org/10.1016/j.jcol.2015.03.005
Correlac¸ão
dos
achados
da
ultrassonografia
tridimensional
com
o
anatomopatológico
em
pacientes
com
endometriose
pélvica
infiltrativa
profunda
submetidos
a
tratamento
cirúrgico
Palavras-chave:
Endometriose Correlac¸ão Ultrassonografia Anatomopatológico Diagnóstico
r
e
s
u
m
o
Objetivo: Esteestudovisacorrelacionarosachadosdaultrassonografiatridimensionalcom osachadosanatomopatológicosempacientescomendometriosepélvicainfiltrativa pro-fundasubmetidosatratamentocirúrgico.
Métodos: Estudoprospectivodeumasériede40pacientescomendometriosepélvica infil-trativaprofundadiagnosticadospelaUSR-3Desubmetidosàvideolaparoscopia.Aspec¸as cirúrgicasforamanalisadashistologicamenteecomparadascomosresultadosdasUSR-3D. Apesquisafoidesenvolvidaentremarc¸ode2008amarc¸ode2011.
Resultados: Osresultadosdosestudoshistopatológicosforam:72,5%daspacientes(n=29) comendometriose,12,5%(n=5)comreac¸ãoinflamatóriacrônicainespecífica,5%(n=2)com tecidofibrosoinespecífico,2,5%(n=1)comadenomioma,2,5%(n=1)commucosacolônica compresenc¸adefocosdehemorragiarecente,edemadelâminaprópriaeerosões superfi-ciais,2,5%(n=1)comhiperplasiadefolículoslinfoideseorestante,2,5%(n=1),comtecido peritonealdentrodoslimitesdanormalidade.
Conclusão: Conclui-se, portanto que a ultrassonografia anorretal tridimensional em pacientesportadorasdeendometriosepélvicainfiltrativaprofundaajudanodiagnóstico delesõesretais,quandoessatécnicaécomparadacomosachadosanatomopatológicosdas pec¸ascirúrgicas.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este éumartigoOpenAccesssobalicençadeCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Endometriosisischaracterizedbythepresenceoftissue simi-lartotheendometriumoutsidetheuterus,leadingtoachronic inflammatoryreaction.1 Theestimatedprevalenceof
endo-metriosisis5–15%ofallwomenofchildbearingage.2,3Among
womensufferingfrominfertility,20–68%showanassociated endometriosis.4 Studies reportthat 15–30%ofwomen with
endometriosishaveprofoundinfiltrativedisease.5,6Colorectal
involvementispresentinabout5–10%ofcasesofthedisease initsdeepinfiltrativeform.7
Physical examination, even during menstruation, has a limited ability to diagnose and quantify the disease.8 The
diagnosis is usually established by laboratory tests, espe-ciallybyimagingtechniquessuchastransvaginalultrasound (TVUS),9–12 anorectalultrasonography(AUS),13,14endoscopic
transrectalultrasonography(ETRUS),9,15magneticresonance
imaging(MRI),10 computed tomography (CT),16 and barium
enema.17Theimagingproceduremustbeabletoindicatethe
numberoffocipresent,thesizeanddepthofthelesion,as wellasitsdistancefromtheanalmargin.18,19 Manystudies
haverecently shown that preoperativeAUS may beuseful inpredictingrectalinfiltrationinpatientswithdeep pelvic endometriosis,18,20 and in the surgical decision making in
favorofanintestinalresection.13
With the recent development of ultrasound equipment with multiplanar vision and the acquisition of automatic images,themodethatusesthethree-dimensionalprobewas establishedintheanorectalcomplexassessmentforthestudy ofbenignandmalignantdiseases,21–27makingitpossibleto
evaluate and accuratelymeasuring the longitudinallength oflesionsandtheirdistancetothesphinctermuscles;thus, additionalinformationnecessaryforchoosingthetherapeutic approachcanbeobtained.
Todate,surgeryremainsasthemostsuccessfuloptionfor treatingendometriosis,eveninthefaceofthepossible limi-tations,complicationsandsequelae.28
This study intends to correlate the findings of three-dimensionalultrasonographywithhistopathologicalstudies inpatientswithdeeppelvicinfiltratingendometriosis submit-tedtosurgery.
Materials
and
methods
Thisisaprospectivestudyofaseriesof40patientswith sus-pecteddeeppelvicinfiltratingendometriosis(DPIE)referred fromtheGynecologyoutpatientclinictotheColoproctology Serviceoutpatientclinic,HospitalGenesis/Gastroclínica Cas-cavel,intheperiodbetweenMarch2008andMarch2011.The patientshadcomplaintssuchasdyspareunia,rectalpain,pain inrightiliacfossa(RIF),constipationand/ortenesmus.
3D-AUSwasperformedbyacolorectalsurgeonwith2-year experienceinthistypeofexam.Thedeviceusedinthisstudy wasa BKMedical(Herlev, Denmark),withPro-Focus probe withtransducerwith360,model2050rotatorywithfrequency of9–16MHz,withafocallengthof2.8–6.2cm,witha50s auto-maticscan, resultingina3-Dcubedisplayedasamultiple sequenceofaxialimages,asacubeimage.For this exami-nation,thepatientswerepositionedinleftlateraldecubitus, afterarectalenemaperformed2hbeforetheexaminationand usingadigitalrectalexamination,allofthemunderanesthetic sedationandwithoutusingarigidrectoscope.Fourautomatic scanswere performedin order toevaluatethe anal canal, anorectaljunction,andthelowerandmiddleaspectsofthe rectum,respectively.Theimagesobtainedwereevaluatedin theaxialandlongitudinalplanesand,ifneeded,were associ-atedwiththediagonalplane.Aftercompletionofthescans, stillimageshavebeenproperlyanalyzed.Weconsideredas normalthosepatientswithnochangeinperirectalfat,and withintactrectalwalllayers.
Thecharacteristicsoftheultrasoundlesionswereas fol-lows:sizeoftheendometrioticfocus;thedistancefromthis focus to the puborectal muscle, and which layers of the intestinalwallthatwereaffected.Thesefindingsallowedthe surgeontochoose his/hersurgicalapproach. Theanalyzed histopathological criteria were:areas offibrosis associated withendometrialtissue,characterizedbyglandsandstroma welldifferentiatedandwithoutatypia.
Patientswithdeeppelvicinfiltrating endometriosis con-firmedby3D-AUS whounderwent videolaparoscopybythe teamsofgynecologicsurgeryand ofcolorectalsurgery,and who subsequently obtainedhistopathological results, were includedinthisstudy.Patientswithdeependometriosiswho refusedtheexamination,patientswhounderwentthe exam-ination,butwithnegativeresults,patientswhohadapositive resultof3D-AUSbutwerenotsubmittedtolaparoscopy,and patientswhorefusedtoparticipateinthestudywereexcluded fromthestudy.
The study was approved by the Ethics Committee in ResearchofFaculdadeAssisGurgacz(protocol232/2012).
Results
Themeanageofpatientsinthisstudywas35.1(21–47)years. Ofthe40patientsevaluated,13(32.5%)hadasmain indica-tion anendometriosis, and had previously beendiagnosed andtreatedwithhormone.Ninepatients (22.5%)had clini-calpainwhendefecatinginthemenstrualperiod,associated withdysmenorrheaanddyspareunia.Sevenpatients(17.5%) hadabdominalcomplaintsofpaininthelowerabdomen,with worseningduringmenstruation,inassociationwith dyspare-unia.Fivepatients(12.5%)reportedonlydysmenorrhea.Four patients(10%)reportedinfertilityanddyspareunia,andtwo otherpatients(5%)reportedpaininthelowerabdomen, dys-pareuniaandconstipation.
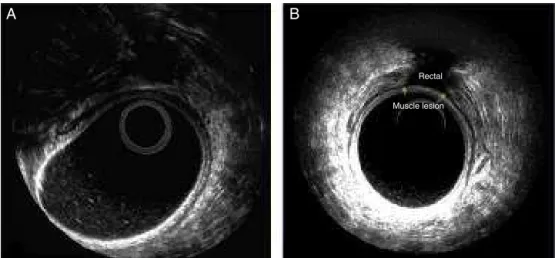
The characteristics of 3D-AUS lesions are round or tri-angular, irregular, heterogeneous hypoechoic masses, with abehaviorofaninvasionofthe rectuminto theperirectal intestinallumen(locatedonlyintheperirectalfat)(Fig.1A). Suchfindingwasfound25patients(62.5%)inthisstudy,or
already invadingatleastthemuscular layeroftherectum, whichwasobservedin15patients(37.5%)(Fig.1B).Themean sizeofthefociwas2.1(0.5–4)cm,theaveragedistancefrom thefocustotheanalsphincterwas4.2(1.5–6)cm(Fig.2Aand B).
Threetypesofsurgerywerecarriedout:20patients(50%) underwentexcisionofendometriosisfoci,13patients(32.5%) weretreatedwithrectosigmoidectomy,and7patients(17.5%) underwentasegmentalcolectomywithastapled anastomo-sis.Decisionswerebasedon3D-AUSandlaparoscopyfindings. Thesurgicalspecimensweresentforhistopathological eval-uationby2pathologists.
The histopathological results were as follows: 72.5% of patientswithendometriosis,12.5%withnonspecificchronic inflammatory reaction, 5% with nonspecific fibrous tissue, 2.5%withadenomyoma,2.5%withcolonicmucosawithfociof recenthemorrhage,edemaoflaminapropriaandsuperficial erosions,2.5%withhyperplasiaoflymphoidfollicles,andthe remaining2.5%withperitonealtissuewithinnormallimits.
Discussion
Incasesofdeependometriosis,isnotalwaysthatthe clini-caltreatmentiseffective,duetothehighrateofoccurrence offibrouslesionsthatarelesslikelytorespondtohormonal therapy.6Surgicaltreatmentmaybetheonlyappropriate
ther-apeutic option for severe endometriosis.29 However, if the
lesions havenotbeen previouslydiagnosed, thesepatients will undergo an incomplete surgical treatment, and often theremay beaneedformorethan onesurgery.Thereare severalmodalitiesforstagingtheselesions;themore accu-rateonesare thenuclear magneticresonance imagingand transvaginal ultrasonography with preparation.30 AUS has
beenusedasanalternativetothesemodalitiesinthe eval-uationofrectalinfiltrationbyendometriosis.31
Thepurposeofthisstudy wastoemphasizethe impor-tance ofthethree-dimensional anorectaltransducerinthe posterior pelvic assessment in patients with endometri-osis.Due tothe limitationtothe examinationofimagesin the longitudinalplane, a transducer was developed which allowsthree-dimensionalreconstructionafterthecaptureof images intwo-dimensional mode.With AUStogether with three-dimensional mode used preoperatively, the surgeon can evaluatethe lesionsinmultipleplanesandalso deter-mine accurately the longitudinal length and the distance with respecttothe sphincter muscles. Thus,critical infor-mation for choosingthe therapeutic approachis obtained. Thediagnosticaccuracyprovidedby3D-AUSisof fundamen-talimportanceforpatientswithendometriosis,especiallyfor youngwomenwhoareseekingfertility,becausethismodality preventscountlesssurgeries.
MRIisthemostcompletetestforthestagingofdeeppelvic lesions;however,thismethodislesseffectiveforthediagnosis ofposteriorpelvicendometriosis,becauseitdonotaccurately assessestheinfiltrationoftherectalwalllayers.18,20Magnetic
Rectal
Muscle lesion
A
B
Fig.1–Injuriesanalyzedby3D-AUS(axialcuts).(A)Lesioninvolvingperirectaltissueand(B)alesioninvolvingtherectal musclelayer.
cities and, in addition, is an expensive examination. Ser-vicesthatdonothaveMRImayhavecomputedtomography; however,thismodalityprovestobemoredifficultin distin-guishinganddelimitingpelvicorgansandinjuries.Asarule, MRIprovides less important informationincomparison to thoseobtainedwithatransvaginalultrasoundperformedby anexperiencedprofessional.33,34
Thedevelopmentofimagingmethodsprovidedimportant qualitative and quantitative contributions to the diagnosis andthustodefinethemostappropriatetherapeuticapproach. Thus,thereisatendencyinfavoroftheincorporationofthese testsinthepreoperativeroutine.
The staging of the lesions with 3D-AUS preoperatively favorstheorientationwithrespecttothesurgicalprocedureto beadoptedineachcase.Thus,onecanpredicttheneed,ornot, ofanapproachand/orintestinalresection,aswellasthe pos-sibilityofaprotectiveostomy.With3D-AUS,thesurgeonwill obtainimportantinformation,suchasthedistancefromthe endometrioticlesiontotheanalsphincter,andwhetherinthis lesionthereisperirectalfatorrectuminvasion.Intheother hand,thismodalitycandefineiftheinvasionaffectsmuscle
and/or,submucosallayer,orrectalmucosa.Thus,itmaybe suggestedthatincasesoffocigreaterthan2cminlengthor occurringinmorethanonethirdofrectalcircumference,it wouldbelesslikelyalocaleconomicresection.
Amongpatientsdiagnosedwithendometriosis,the corre-lationofthepathologyreportwith3D-AUSfindingsoccurred in 72.5% of 40 patients undergoing surgery for removalof lesions suggestive of endometriosis and detected by this examination.
Microscopically, endometriosis is defined by the pres-enceoftypicalendometrialglandsandstroma,depositionof hemosiderin,erythrocytes,andmacrophages,andfibrous tis-suecontaininginflammatorycells.Thefactofnothavinga correlationinallcasesmayberelatedtoapreviousmedical treatment,orbybeingolderlesions,withscarsandperitoneal retraction.Theanatomopathologicalcorrelationisgenerally observedinactivelesions.35Pathologicalexaminationofthe
lesions should be usedas an auxiliary method of diagno-sis,bynotbeingpositiveinallcases.Themainlimitationof ourstudy arisesfrom theneedfortraining pathologists,in ordertoreviewthe surgicalpiecesofendometriosisforthe
Lower rectum
A
B
Uterus
Puborectal Puborectal
Muscle lesion
1
2 1
definitivediagnosis.Anotherlimitingfactor isthefactthat ours isa referral service and that, moreover,many ofthe patients had already undergone medical treatment and/or surgery.Thus,theresultinginjurieslosttheirglandular his-tologicalcharacteristic.
Conclusion
Thus, we can conclude that the use ofthree-dimensional anorectalultrasonographyinpatientswithdeeppelvic infil-tratingendometriosis aidinthediagnosis ofrectallesions, when compared with the pathological findings ofsurgical specimens.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. KennedyS,BergqvistA,ChapronC,D’HoogheT,Dunselman
G,GrebR,etal.ESHREguidelineforthediagnosisand
treatmentofendometriosis.HumReprod.2005;20:2698–704.
2. LeyendeckerG,HerbertzM,KunzG,MallG.Endometriosis
resultsfromthedislocationofbasalendometrium.Hum
Reprod.2002;17:2725–36.
3. LeyendeckerG,KunzG,NoeM,HerbertzM,MallG.
Endometriosis:adysfunctionanddiseaseofthearchimetra.
HumReprodUpdate.1998;4:752–62.
4. KoninckxPR,MeulemanC,DemeyereS,LesaffreE,Cornillie
FJ.Suggestiveevidencethatpelvicendometriosisisa
progressivedisease,whereasdeeplyinfiltrating
endometriosisisassociatedwithpelvicpain.FertilSteril. 1991;55:759–65.
5. KecksteinJ,UlrichU,KandolfO,WiesingerH,WustlichM.
Laparoscopictherapyofintestinalendometriosisandthe
rankingofdrugtreatment.ZentralblGynako.2003;125:259–66.
6. FauconnierA,ChapronC.Endometriosisandpelvicpain:
epidemiologicalevidenceoftherelationshipand
implications.HumReprodUpdate.2005;11:595–606.
7. BalleyguierC,ChapronC,DubuissonJB,KinkelK,Fauconnier
A,VieiraM,etal.Comparisonofmagneticresonanceimaging
andtransvaginalultrasonographyindiagnosingbladder
endometriosis.JAmAssocGynecolLaparosc.2002;9:15–23.
8. KoninckxPR,MartinD.Treatmentofdeeplyinfiltrating
endometriosis.CurrOpinObstetGynecol.1994;6:231–41.
9. BazotM,DetchevR,CortezA,AmouyalP,UzanS,DaraiE.
Transvaginalsonographyandrectalendoscopicsonography
fortheassessmentofpelvicendometriosis:apreliminary
comparison.HumReprod.2003;18:1686–92.
10.AbrãoMS,Gonc¸alvesMOC,DiasJAJr,PodgaecS,ChamieLP,
BlasbalgR.Comparisonbetweenclinicalexamination,
transvaginalsonographyandmagneticresonanceimaging
forthediagnosisofdeependometriosis.HumReprod.
2007;22:3092–7.
11.MenadaMV,RemorgidaV,AbbamonteLH,FulcheriE,RagniN,
FerreroS.Transvaginalultrasonographycombinedwith
water-contrastintherectuminthediagnosisofrectovaginal
endometriosisinfiltratingthebowel.FertilSteril. 2008;89:699–700.
12.GuerrieroS,AjossaS,GeradM,VirgilioB,AngioniS,MelisGB.
Diagnosticvalueoftransvaginal‘tenderness-guided’
ultrasonographyforthepredictionoflocationofdeep
endometriosis.HumReprod.2008;23:2452–7.
13.ChapronC,DumontierI,DoussetB,FritelX,TardifD,Roseau
G,etal.Resultsandroleofrectalendoscopicultrasonography
forpatientswithdeeppelvicendometriosis.HumReprod.
1998;13:2266–70.
14.KogaK,OsugaY,YanoT,MomoedaM,YoshinoO,HirotaY,
etal.Characteristicimagesofdeeplyinfiltratingrectosigmoïd
endometriosisontransvaginalandtransrectal
ultrasonography.HumReprod.2003;18:1328–33.
15.AbraoMS,NemeRM,AverbachM,PettaCA,AldrighiJM.
Rectalendoscopicultrasoundwitharadicalprobeinthe
assessmentofrectovaginalendometriosis.JAmAssoc
GynecolLaparosc.2004;11:50–4.
16.BiscaldiE,FerreroS,FulcheriE,RagniN,RemorgidaV,
RollandiGA.MDCTenteroclysisurographywithsplit-bolus
techniqueprovidesinformationonureteralinvolvementin
patientswithsuspectedbowelendometriosis.AmJ
Roentgenol.2011;196:W635–40.
17.RibeiroHSAA,RibeiroPAAG,RodriguesFC,DonadioN,Auge
APF,AokiT.Valordoenemadebáriocomduplocontrasteo
diagnósticodaendometriosedoretoesigmóide.RevBras
GinecolObstet.2008;30:400–5.
18.ChapronC,VieiraM,ChopinN,BalleyguierC,BarakatH,
DumontierI,etal.Accuracyofrectalendoscopic
ultrasonographyandmagneticresonanceimaginginthe
diagnosisofrectalinvolvementforpatientspresentingwith
deeplyinfiltratingendometriosis.UltrasoundObstetGynecol.
2004;24:175–9.
19.Gonc¸alvesMO,DiasJAJr,PodgaecS,AverbachM,AbrãoMS.
Transvaginalultrasoundfordiagnosisofdeeplyinfiltrating
endometriosis.IntJGynaecolObstet.2009;104:156–60.
20.CamagnaO,DhainautC,DupuisO,SonciniE,MartinB,
PalazzoL,etal.Surgicalmanagementofrectovaginalseptum
endometriosisfromacontinuousseriesof50cases.Gynecol
ObstetFertil.2004;32:199–209.
21.ChristensenAF,NielsenMB,EngeholmSA,RoedH,Svendsen
LB,ChristensenH.Three-dimensionalanalendosonography
mayimprovestagingofanalcancercomparedwith
two-dimensionalendosonography.DisColonRectum.
2004;47:341–5.
22.Murad-RegadasSM,RegadasFSP,RodriguesLV,SilvaFRS,
LimaDMR,Regadas-FilhoFSP,etal.Three-dimensional
echodefecographyanovelproceduretoassessanterior
anorectoceleinwomen.TechColoproct.2006.
23.Murad-RegadasSM,RegadasFSP,RodriguesLV,EscalanteRD,
SilvaFRS,LimaDMR,etal.EcodefecografiaTridimensional
Dinâmica.NovaTécnicaparaAvaliac¸ãodaSíndromeda
Defecac¸ãoObstruída(SDO).RevBrasColoproct.
2006;26:168–77.
24.Murad-RegadasSM,RegadasFSP,WexnerSD,RodriguesLV,
SilvaFRS,LimaDMR,etal.Anorectalthree-dimensional
endosonographyandanalmanometryinassessinganterior
rectoceleinwomen:anewpathogenesisconceptandthe
basicsurgicalprinciple.ColorectalDis.2007;9:80–5.
25.Murad-RegadasSM,RegadasFSP,RodriguesL,SouzaMHLP,
LimaDMR,SilvaFRS,etal.Anovelproceduretoassess
anismususingthree-dimensionaldynamicultrasonography.
ColorectalDis.2007;9:159–65.
26.Murad-RegadasSM,RegadasFSP.Ultrassonografiaanorretal
dinâmica–novastécnicas.In:RegadasFSP,Murad-Regadas
SM,editors.Distúrbiosfuncionaisdoassoalhopélvico.Riode
Janeiro:Revinter;2006.p.79–94.
27.RegadasSMM,RegadasFSP,RodriguesLV,SilvaFR,LimaDMR,
Regadas-FilhoFSP.Importânciadoultra-somtridimensional
naavaliac¸ãoanorretal.ArqGastroenterol.2005;42:226–32.
28.DaraiE,BazotM,RouzierR,HouryS,DubernardG.Outcome
oflaparoscopiccolorectalresectionforendometriosis.Curr
29.RomanH,KouteichK,GromezA,HochainP,ReschB,Marpeau
L.Endorectalultrasoundaccuracyinthediagnosisofrectal
endometriosisinfiltrationdepth.FertilSteril.2008;90: 1008–13.
30.Gonc¸alvesMO,PodgaecS,DiasJAJr,GonzalezM,AbraoMS.
Transvaginalultrasonographywithbowelpreparationisable
topredictthenumberoflesionsandrectosigmoidlayers
affectedincasesofdeependometriosis,definingsurgical
strategy.HumReprod.2010;25:665–71.
31.SagaeUE,LimaDMR,CavalliN,SagaeLMT,TanakaTM,
BonattoMW,etal.Importânciadaultra-sonografiaanorretal
tridimensionalnadecisãoterapêuticadaendometriose
profunda.RevBrasColoproct.2009;29:435–42.
32.BazotM,DaraiE,HouraniR,ThomassinI,CortezA,UzanS,
etal.Deeppelvicendometriosis:MRimagingfordiagnosis
andpredictionofextensionofdisease.Radiology.
2004;232:379–89.
33.TranKT,KuijpersHC,WillemsenWN,BultenH.Sugical
treatmenteofsymptomaticrectosigmoidendometriosis.EurJ
Surg.1996;162:139–41.
34.DumontierI,RoseauG,VincentB,ChapronC,DoussetB,
ChaussadeS,etal.Comparisonofendoscopicultrasoundand
magneticresonanceimaginginseverepelvivendometriosis.
GastroenterolClinBiol.2000;24:1197–204.
35.BergqvistA.Therelationshipbetweenendometrioticlesions